You might also like
- How To DrawDocument676 pagesHow To DrawPreethi Gopalan83% (6)
- Encyclopedia of Cancer PDFDocument461 pagesEncyclopedia of Cancer PDFBachtiar Muhammad ArifNo ratings yet
- How To Study & Improve at ChessDocument16 pagesHow To Study & Improve at Chessprashant100% (8)
- Fine Art of The Big TalkDocument251 pagesFine Art of The Big Talkdiometh100% (2)
- Edit - The Monster Guide To Candlestick PatternsDocument34 pagesEdit - The Monster Guide To Candlestick PatternsArif Wira Adyatama100% (4)
- Classification AO PediatricDocument36 pagesClassification AO PediatricdvcmartinsNo ratings yet
- Therapeutic Drug Monitoring: By: Adewale Akinseloyin Oluwatimilehin Agboola Oluwatosin AjibadeDocument33 pagesTherapeutic Drug Monitoring: By: Adewale Akinseloyin Oluwatimilehin Agboola Oluwatosin AjibadeJoe AjibadeNo ratings yet
- AmputationDocument160 pagesAmputationChamalla Deepak100% (4)
- Ketorolac (Drug Study)Document2 pagesKetorolac (Drug Study)Cassandra Grace Labial Paynter89% (18)
- Rotational Flap Closure of 1st and 5nth Met HeadDocument8 pagesRotational Flap Closure of 1st and 5nth Met HeadleahbayNo ratings yet
- AmputationDocument14 pagesAmputationJuanitoCabatañaLimIIINo ratings yet
- 24.amputations of The Foot and AnkleDocument29 pages24.amputations of The Foot and AnklesteoeviciNo ratings yet
- Nursing Care Plan PPROM 1Document1 pageNursing Care Plan PPROM 1Nickaela Calalang100% (1)
- Medical Case History - Acute Appendicitis TEXTDocument2 pagesMedical Case History - Acute Appendicitis TEXTEliza IancuNo ratings yet
- Caries Activity TestDocument8 pagesCaries Activity TestSaransh MalotNo ratings yet
- Aaos Elbow Surgical Approaches-1Document9 pagesAaos Elbow Surgical Approaches-1Mossa SultanyNo ratings yet
- Above Elbow and Below Elbow AmputationDocument6 pagesAbove Elbow and Below Elbow AmputationJohan harjonoNo ratings yet
- Amputation and Rehabilitation 2013 Surgery OxfordDocument4 pagesAmputation and Rehabilitation 2013 Surgery OxfordSanjaya SenevirathneNo ratings yet
- Amputation and RehabilitationDocument4 pagesAmputation and RehabilitationimherestudyingNo ratings yet
- Modifying Syme Amputation Prevents Heel Pad MigrationDocument5 pagesModifying Syme Amputation Prevents Heel Pad MigrationdamonenNo ratings yet
- Lowe Limb AmputationDocument11 pagesLowe Limb AmputationNadya ZahraNo ratings yet
- symeDocument5 pagessymepascallindaNo ratings yet
- DEFINATION: Amputation Is The Removal of ADocument22 pagesDEFINATION: Amputation Is The Removal of AsurchadNo ratings yet
- The Syme AmputationDocument8 pagesThe Syme AmputationAngiologia CMN La RazaNo ratings yet
- Comminuted Intraarticular Fractures of The Tibial Plateau Lead To Posttraumatic Osteoarthritis of The Knee: Current Treatment ReviewDocument7 pagesComminuted Intraarticular Fractures of The Tibial Plateau Lead To Posttraumatic Osteoarthritis of The Knee: Current Treatment ReviewGustavoBecerraNo ratings yet
- Digital AmputationsDocument10 pagesDigital AmputationsENnie TentjeNo ratings yet
- AMPUTAÇÃODocument7 pagesAMPUTAÇÃODani SNo ratings yet
- Bilateral Sagittal Split Mandibular Ramus Osteotomy TechniqueDocument10 pagesBilateral Sagittal Split Mandibular Ramus Osteotomy TechniqueBenjie LawNo ratings yet
- Toe DisarticulationDocument4 pagesToe Disarticulationadel santosNo ratings yet
- Combat Foot and Ankle Trauma: LT Scott M. Tintle, MD, CDR John J. Keeling, MD, and LTC Scott B. Shawen, MDDocument7 pagesCombat Foot and Ankle Trauma: LT Scott M. Tintle, MD, CDR John J. Keeling, MD, and LTC Scott B. Shawen, MDbaljinderNo ratings yet
- Tibial Fractures Useful Plastering Technique: MethodDocument4 pagesTibial Fractures Useful Plastering Technique: MethodgregraynerNo ratings yet
- 1 s2.0 S0011853222001604 MainDocument20 pages1 s2.0 S0011853222001604 MainDANTE DELEGUERYNo ratings yet
- Proximal Humerus Fracture Fixation Surgical TechnicDocument6 pagesProximal Humerus Fracture Fixation Surgical TechnicAdhimas WicaksanaNo ratings yet
- Amputation of The Foot PDFDocument29 pagesAmputation of The Foot PDFNyoman MaharmayaNo ratings yet
- AMPUTATION SEVERITY SCOREDocument4 pagesAMPUTATION SEVERITY SCOREMalueth AnguiNo ratings yet
- Wrist Arthrodesis With Femoral Head Structural.9Document5 pagesWrist Arthrodesis With Femoral Head Structural.9juanit45No ratings yet
- AmputationDocument4 pagesAmputationFalah IsmailNo ratings yet
- DIPJ Denervation Arenas-PratDocument3 pagesDIPJ Denervation Arenas-PratanindyaNo ratings yet
- Amputations Below The Knee: Ernest M. Burgess. M.D. Joseph H. Zettl, C.PDocument12 pagesAmputations Below The Knee: Ernest M. Burgess. M.D. Joseph H. Zettl, C.PLuqmanul HakimNo ratings yet
- An ABC Technical Algorithm To Mangled HandDocument10 pagesAn ABC Technical Algorithm To Mangled HandRoxana LungociNo ratings yet
- Nexgen Complete Knee Solution: ZimmerDocument37 pagesNexgen Complete Knee Solution: Zimmerflo1987No ratings yet
- Pi Is 2212628717302013Document5 pagesPi Is 2212628717302013DrManoj JagarlamudiNo ratings yet
- Pa Tho Physiology of AmputationDocument5 pagesPa Tho Physiology of AmputationMary Karen Rose BorjaNo ratings yet
- Strategies To Improve Outcomes From Operative Childhood Management of DDHDocument9 pagesStrategies To Improve Outcomes From Operative Childhood Management of DDHVALENTINA LOPEZ MARINNo ratings yet
- Cephalomedullary Nailing of Pertrochanteric Femur Fractures Using A Large Distractor and Standard Radiolucent TableDocument4 pagesCephalomedullary Nailing of Pertrochanteric Femur Fractures Using A Large Distractor and Standard Radiolucent Tabledrbane123No ratings yet
- Amputation and Rehabilitation 2010Document4 pagesAmputation and Rehabilitation 2010Amal KamalNo ratings yet
- Hip Disarticulation Procedure Guide - Removal of Lower Extremity Through Hip JointDocument13 pagesHip Disarticulation Procedure Guide - Removal of Lower Extremity Through Hip JointSomeshwar GuptNo ratings yet
- Lefort Osteotomy PPT (Ing)Document15 pagesLefort Osteotomy PPT (Ing)Chandra BudiNo ratings yet
- Friel 2009Document17 pagesFriel 2009sidharthNo ratings yet
- Amputation and ProstheticsDocument45 pagesAmputation and Prostheticspriyanka0% (1)
- Inside Out Meniscus Repair 2013 Arthroscopy TechniquesDocument8 pagesInside Out Meniscus Repair 2013 Arthroscopy TechniqueschinthakawijedasaNo ratings yet
- partial footDocument15 pagespartial footpascallindaNo ratings yet
- AmputationDocument35 pagesAmputationNannieNo ratings yet
- Treating Onychomycosis, Intermittent Claudication, Dermatitis, Charcot Arthropathy, Trophic UlcersDocument9 pagesTreating Onychomycosis, Intermittent Claudication, Dermatitis, Charcot Arthropathy, Trophic UlcersJairah CandaoNo ratings yet
- Swanson: Flexible Hinge Toe ImplantDocument14 pagesSwanson: Flexible Hinge Toe ImplantAnonymous kdBDppigENo ratings yet
- Amputation FingerDocument36 pagesAmputation Fingerlolianton87No ratings yet
- Revision THRDocument11 pagesRevision THRJayNo ratings yet
- Hakan 2007 Extended Lateral Supramalleolar Flap For Very Distal Foot Coverage A Case With Arteriovenous MalformationDocument4 pagesHakan 2007 Extended Lateral Supramalleolar Flap For Very Distal Foot Coverage A Case With Arteriovenous MalformationThach Nguyen NgocNo ratings yet
- Upton 2011Document9 pagesUpton 2011FeliciaDewiNo ratings yet
- Median Sternotomy ProcedureDocument5 pagesMedian Sternotomy ProcedureNelly NehNo ratings yet
- Current Concepts in Upper-Extremity Amputation: Key WordsDocument10 pagesCurrent Concepts in Upper-Extremity Amputation: Key WordsCarlos GonzalesNo ratings yet
- CHAPTER 19 - Mini Open Rota - 2008 - Surgical Techniques of The Shoulder ElbowDocument7 pagesCHAPTER 19 - Mini Open Rota - 2008 - Surgical Techniques of The Shoulder ElbowJaime Vázquez ZárateNo ratings yet
- Surgicaltreatmentof Intra-Articularcalcaneal Fractures: John J. Stapleton,, Thomas ZgonisDocument8 pagesSurgicaltreatmentof Intra-Articularcalcaneal Fractures: John J. Stapleton,, Thomas Zgonisthzone1986No ratings yet
- Crawley 2015Document6 pagesCrawley 2015Eduardo HernándezNo ratings yet
- The Treatment of Intrabony Defects With Bone Grafts: P S. R M A. R & G M. BDocument16 pagesThe Treatment of Intrabony Defects With Bone Grafts: P S. R M A. R & G M. BMohamedAtefNo ratings yet
- Periosteal Releasing Incision For Successful Coverage of Augmented Sites. A Technical NoteDocument6 pagesPeriosteal Releasing Incision For Successful Coverage of Augmented Sites. A Technical NotemaxNo ratings yet
- LWBK836 Ch98 p1021-1030Document10 pagesLWBK836 Ch98 p1021-1030metasoniko81No ratings yet
- HTTPS://WWW - Scribd.com/book/443365556/this Is Going To Hurt Secret Diaries of A Medical Resident by Adam Kay Conversation StartersDocument9 pagesHTTPS://WWW - Scribd.com/book/443365556/this Is Going To Hurt Secret Diaries of A Medical Resident by Adam Kay Conversation Startersreemali69No ratings yet
- Secondary Flexor RepairDocument10 pagesSecondary Flexor RepairŠišmišova DevojkaNo ratings yet
- Endoscopic Procedures on the SpineFrom EverandEndoscopic Procedures on the SpineJin-Sung KimNo ratings yet
- How To Be A Good Boyfriend 1Document6 pagesHow To Be A Good Boyfriend 1JonyPopescuNo ratings yet
- Best Places For First Dates PDFDocument8 pagesBest Places For First Dates PDFJonyPopescuNo ratings yet
- How To Impress Your Date PDFDocument3 pagesHow To Impress Your Date PDFmarkNo ratings yet
- How To Date Well PDFDocument2 pagesHow To Date Well PDFmarkNo ratings yet
- Dating & Falling in LoveDocument35 pagesDating & Falling in LovetantratriggershivaNo ratings yet
- Deeper VoiceDocument12 pagesDeeper VoiceJavier ZaffaroniNo ratings yet
- Principles For DatingDocument6 pagesPrinciples For DatingJesus LivesNo ratings yet
- Massage Techniques PDFDocument2 pagesMassage Techniques PDFmarkNo ratings yet
- The Ultimate Guide To Start A Profitable Part Time Income Through Trading Forex - v2 1 PDFDocument91 pagesThe Ultimate Guide To Start A Profitable Part Time Income Through Trading Forex - v2 1 PDFnixNo ratings yet
- Tips For Successful Dating and RelationshipsDocument2 pagesTips For Successful Dating and RelationshipsIoana BogdanNo ratings yet
- Spica CastDocument10 pagesSpica CastSetia ningrum WibisanaNo ratings yet
- Quadricep Tendon Rupture-Repair Protocol: PRECAUTIONS: Avoid Impact Loads/sudden Activation (Eccentric Load) GoalsDocument3 pagesQuadricep Tendon Rupture-Repair Protocol: PRECAUTIONS: Avoid Impact Loads/sudden Activation (Eccentric Load) GoalsmarkNo ratings yet
- Quadriceps and Patellar Tendon Repair RehabilitationDocument14 pagesQuadriceps and Patellar Tendon Repair Rehabilitationdhikaprasetya11_1969No ratings yet
- Harvesting The Free Fibular Graft A Modified ApproDocument4 pagesHarvesting The Free Fibular Graft A Modified AppromarkNo ratings yet
- Ilizarov-Bone TransportDocument6 pagesIlizarov-Bone TransportmarkNo ratings yet
- AOOTA Classification 2018 Info Booklet 17122101Document24 pagesAOOTA Classification 2018 Info Booklet 17122101Virgy AgudoNo ratings yet
- Handbook of COVID-19 Prevention (English Version)Document68 pagesHandbook of COVID-19 Prevention (English Version)adi wibowo yudo pranoto80% (5)
- Suture Anchor Technique for Muscle Belly RepairDocument2 pagesSuture Anchor Technique for Muscle Belly RepairmarkNo ratings yet
- Help CfponsetiDocument32 pagesHelp CfponsetiShAi_MyStERiOuSNo ratings yet
- PG List 2016 17Document4 pagesPG List 2016 17Sundeep ArcheliesNo ratings yet
- Cebu Doctors' University College of Medicine Level III Block I Modules 1-4 Compiled QuestionsDocument2 pagesCebu Doctors' University College of Medicine Level III Block I Modules 1-4 Compiled QuestionsNeil Victor Ongco PajugotNo ratings yet
- Comprehensive Cleft CareDocument9 pagesComprehensive Cleft CareEvgeniya KocherginaNo ratings yet
- Methadone Hydro ChlorideDocument4 pagesMethadone Hydro Chlorideapi-3797941100% (1)
- Doh 1Document3 pagesDoh 1Fitz Dyan TorresNo ratings yet
- NCP - Ineffective Breathing PatternDocument4 pagesNCP - Ineffective Breathing PatternPRINCESS KOBAYASHINo ratings yet
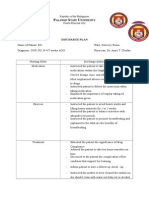
- Discharge Plan: Alawan Tate NiversityDocument2 pagesDischarge Plan: Alawan Tate NiversityLenieGracePascoNo ratings yet
- Heart SurgeonDocument8 pagesHeart SurgeonayaanmalikyaseenNo ratings yet
- Chronic Marginal PeriodontitisDocument21 pagesChronic Marginal PeriodontitisLaslo Mihaela Larisa100% (1)
- Postmortem Toxicology - Farmasi ForensikDocument20 pagesPostmortem Toxicology - Farmasi Forensikedrina elfia rosaNo ratings yet
- A Model To Predict Short-Term Death or Readmission After Intensive Care Unit DischargeDocument10 pagesA Model To Predict Short-Term Death or Readmission After Intensive Care Unit DischargeInnani Wildania HusnaNo ratings yet
- Periodontal DiseasesDocument47 pagesPeriodontal DiseasesPratikNo ratings yet
- Ultrasound Supraclavicular Plexus Block Enhances Arteriovenous Fistula Blood Flow in ESRDDocument14 pagesUltrasound Supraclavicular Plexus Block Enhances Arteriovenous Fistula Blood Flow in ESRDaymankahlaNo ratings yet
- Rose Geranium in Sesame Oil NasalDocument3 pagesRose Geranium in Sesame Oil NasalHolly JonesNo ratings yet
- D.S.S. Aiims Prepration Test Series - 10 DR - SANJAY 7014964651 All Subject MCQDocument24 pagesD.S.S. Aiims Prepration Test Series - 10 DR - SANJAY 7014964651 All Subject MCQDr-Sanjay SinghaniaNo ratings yet
- Upper Gastrointestinal Bleeding (UGIB) : Practice EssentialsDocument52 pagesUpper Gastrointestinal Bleeding (UGIB) : Practice EssentialsrishaNo ratings yet
- Implant ProstheticsDocument8 pagesImplant Prostheticssaggar65No ratings yet
- Understanding The Carbon Dioxide Gaps: ReviewDocument9 pagesUnderstanding The Carbon Dioxide Gaps: ReviewLaura A M MNo ratings yet
- HIV RNA Virus Classification and PathogenesisDocument2 pagesHIV RNA Virus Classification and PathogenesisBONNA FAYE CHRISZEL HUI YING TANNo ratings yet
- Macrocytic anemia causes and treatmentDocument2 pagesMacrocytic anemia causes and treatmentLefteris ChatzidoukasNo ratings yet
- Hypothyroidism Diagnosis and TreatmentDocument59 pagesHypothyroidism Diagnosis and TreatmentAmir Mahmoud100% (1)
- W3health6 q1 Mod1of2 PersonalHealthIssuesSelf-MngtSkills v2-1Document22 pagesW3health6 q1 Mod1of2 PersonalHealthIssuesSelf-MngtSkills v2-1Rona DindangNo ratings yet
- Fall Risk Factors For The Learner 1Document13 pagesFall Risk Factors For The Learner 1StokleyCNo ratings yet
- Infectious Bronchitis and Its Effect On Egg Production and Egg QualityDocument2 pagesInfectious Bronchitis and Its Effect On Egg Production and Egg QualityPrima Puji RaharjoNo ratings yet