You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- American Government Stories of A Nation Essentials Edition 1st Edition Abernathy Test Bank 1Document50 pagesAmerican Government Stories of A Nation Essentials Edition 1st Edition Abernathy Test Bank 1kevin100% (30)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- MCQ 1Document5 pagesMCQ 1hbusyNo ratings yet
- MCQ 1Document5 pagesMCQ 1hbusyNo ratings yet
- MCQ 2Document5 pagesMCQ 2hbusyNo ratings yet
- Other Primary Oral Healthcare Programmes: 1. Pre-School Dental ProgrammeDocument1 pageOther Primary Oral Healthcare Programmes: 1. Pre-School Dental ProgrammehbusyNo ratings yet
- Dental TreatmentDocument2 pagesDental TreatmenthbusyNo ratings yet
- Location of Oral Health Division at The Ministry of HealthDocument1 pageLocation of Oral Health Division at The Ministry of HealthhbusyNo ratings yet
- Organization Chart (Important To Know For SPA Interview)Document1 pageOrganization Chart (Important To Know For SPA Interview)hbusyNo ratings yet
- Important Elements of School Dental Service (Exam Question)Document2 pagesImportant Elements of School Dental Service (Exam Question)hbusyNo ratings yet
- Factors Influencing Repair of Dental Restorations With Resin CompositeDocument7 pagesFactors Influencing Repair of Dental Restorations With Resin CompositehbusyNo ratings yet
- ProfessionalDocument6 pagesProfessionalhbusyNo ratings yet
- All Ceramic Crowns and Shade SelectionDocument13 pagesAll Ceramic Crowns and Shade Selectionhbusy100% (1)
- BenghaziDocument7 pagesBenghazihbusyNo ratings yet
- Korean Cinema and Kim-Ki DukDocument8 pagesKorean Cinema and Kim-Ki DukTayaz FakhriNo ratings yet
- PNL Account Cashflow Forecast: Missing ValuesDocument5 pagesPNL Account Cashflow Forecast: Missing ValuespiyaNo ratings yet
- Supply Chain Management of BanglalinkDocument20 pagesSupply Chain Management of BanglalinkSindhu Nath Chowdhury100% (1)
- Regulators Reguladores: Alternators. Starters and PartsDocument18 pagesRegulators Reguladores: Alternators. Starters and Partsjohn jairo guzmanNo ratings yet
- South Yarra Cable Tram Engine House and Tram ShedDocument18 pagesSouth Yarra Cable Tram Engine House and Tram ShedGary VinesNo ratings yet
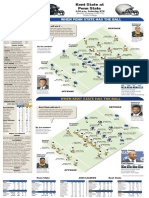
- Kent State at Penn StateDocument1 pageKent State at Penn StatedlevarseNo ratings yet
- Compro Persada Group - PSDDocument13 pagesCompro Persada Group - PSDLinda NababanNo ratings yet
- Project FoilDocument11 pagesProject FoilSanjay KumarNo ratings yet
- 2022 Bravecto Sentinel Consumer RebateDocument2 pages2022 Bravecto Sentinel Consumer RebatebatanggapoNo ratings yet
- OIG Compliance Program For Third-Party Medical Billing CompaniesDocument15 pagesOIG Compliance Program For Third-Party Medical Billing CompaniesaaronborosNo ratings yet
- Tests of Significance Notes PDFDocument12 pagesTests of Significance Notes PDFManish KNo ratings yet
- Department of Education: Republic of The PhilippinesDocument7 pagesDepartment of Education: Republic of The PhilippinesRochelle May CanlasNo ratings yet
- Ic Engines and Gas TurbineDocument3 pagesIc Engines and Gas TurbineLippin PaulyNo ratings yet
- Los 10 Mandamientos Del Médico InternoDocument3 pagesLos 10 Mandamientos Del Médico InternoEyder Alexander RodriguezNo ratings yet
- Cereal CropsDocument34 pagesCereal CropsJe-ar ColipanoNo ratings yet
- Cambridge English For Engineering PDF (Dragged) 3Document1 pageCambridge English For Engineering PDF (Dragged) 3Alex GunaratnaNo ratings yet
- Yas HistoryDocument7 pagesYas HistoryRafaela Raposo Righi100% (1)
- Panasonic TH42PA20ADocument80 pagesPanasonic TH42PA20AgondifNo ratings yet
- Direct Recruitment of Assistant Professors in Tamil Nadu Collegiate Educational Service For Govt. Arts & Science COLLEGES - 2012Document18 pagesDirect Recruitment of Assistant Professors in Tamil Nadu Collegiate Educational Service For Govt. Arts & Science COLLEGES - 2012nellai kumarNo ratings yet
- Pythagoras' & Trigonometry Past Paper QuestionsDocument46 pagesPythagoras' & Trigonometry Past Paper QuestionsinternationalmakkhayarNo ratings yet
- Technical Specification MBGDocument5 pagesTechnical Specification MBGM RikoNo ratings yet
- Module 1 Work Study & Productivity ILODocument24 pagesModule 1 Work Study & Productivity ILOSangam KadoleNo ratings yet
- EnglishDocument32 pagesEnglishVilitzaNo ratings yet
- Fequently Asked Questions (Faqs) On FcraDocument10 pagesFequently Asked Questions (Faqs) On FcraJATEENKAPADIA123No ratings yet
- Object Oriented Programmimg Micro Project Proposal ON Hotel Mangement SystemDocument9 pagesObject Oriented Programmimg Micro Project Proposal ON Hotel Mangement Systemgirish desaiNo ratings yet
- XND-8020R/8030R/8040R: 5M Network IR Dome CameraDocument1 pageXND-8020R/8030R/8040R: 5M Network IR Dome CameracesarNo ratings yet
- Effects of Sleep Pattern, Duration, and Quality On Premenstrual Syndrome and Primary Dysmenorrhea in Korean High School GirlsDocument14 pagesEffects of Sleep Pattern, Duration, and Quality On Premenstrual Syndrome and Primary Dysmenorrhea in Korean High School Girlssahariam.palaguyanNo ratings yet
- Britannia Studio Equipment ListDocument4 pagesBritannia Studio Equipment ListJuan BastidasNo ratings yet
- Educational Leadership Management - Exam - July 2017Document1 pageEducational Leadership Management - Exam - July 2017Mazuba MutintaNo ratings yet