You might also like
- RTS 2011Document8 pagesRTS 2011Puspa AmandatyNo ratings yet
- A Long Short-Term Memory Ensemble Approach For Improving The Output Prediction in ICUDocument11 pagesA Long Short-Term Memory Ensemble Approach For Improving The Output Prediction in ICUIdris RabiuNo ratings yet
- Developing A Predictive Model of Stroke Using Support Vector MachineDocument6 pagesDeveloping A Predictive Model of Stroke Using Support Vector MachineAlexander HernandezNo ratings yet
- s12883 022 03003 7Document7 pagess12883 022 03003 7donadoguillermoNo ratings yet
- Proposal On Machine Learning Based System For Prediction of Cardiovascular and Chronic Respiratory DiseaseDocument3 pagesProposal On Machine Learning Based System For Prediction of Cardiovascular and Chronic Respiratory Diseasemafuz biolaNo ratings yet
- Machine Learning Solutions Applied To Amyotrophic Lateral Sclerosis Prognosis: A ReviewDocument12 pagesMachine Learning Solutions Applied To Amyotrophic Lateral Sclerosis Prognosis: A ReviewJoel ArraisNo ratings yet
- Prognostic Models in Severe Traumatic Brain Injury: A Systematic Review and Meta-AnalysisDocument16 pagesPrognostic Models in Severe Traumatic Brain Injury: A Systematic Review and Meta-AnalysisCaroline FelicianoNo ratings yet
- ML Sa 1Document5 pagesML Sa 1Abhay RaichandNo ratings yet
- 2nd ReviewDocument21 pages2nd ReviewShivank YadavNo ratings yet
- International Journal of Medical Informatics: Zhe Wang, Lijuan Yao, Dongdong Li, Tong Ruan, Min Liu, Ju GaoDocument8 pagesInternational Journal of Medical Informatics: Zhe Wang, Lijuan Yao, Dongdong Li, Tong Ruan, Min Liu, Ju GaoMuzamilNo ratings yet
- A Machine Learning Model For Predicting Favorable Outcome in Severe Traumatic Brain Injury Patients After 6 MonthsDocument8 pagesA Machine Learning Model For Predicting Favorable Outcome in Severe Traumatic Brain Injury Patients After 6 MonthsRashellya RasyidaNo ratings yet
- 2021 Article 120Document14 pages2021 Article 120Fitri ainun MalahayatiNo ratings yet
- Three Dimensional Model For Diagnostic Prediction: A Data Mining ApproachDocument5 pagesThree Dimensional Model For Diagnostic Prediction: A Data Mining ApproachInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- Main 25Document6 pagesMain 25pokharelriwaj82No ratings yet
- 2019 DsadaşsklDocument8 pages2019 DsadaşsklAhmet KaragozNo ratings yet
- Machine Learning Prediction of Coronary Heart DiseaseDocument6 pagesMachine Learning Prediction of Coronary Heart DiseaseNowreen HaqueNo ratings yet
- Buettner 2019Document6 pagesBuettner 2019äBHïSHëK DHöTëNo ratings yet
- SynopsisDocument5 pagesSynopsisPriyankaNo ratings yet
- IntroductionDocument8 pagesIntroductiontarunkumarsj117No ratings yet
- Goto2018 PDFDocument5 pagesGoto2018 PDFsangram singhNo ratings yet
- Final 12Document10 pagesFinal 12uzeefeshan76No ratings yet
- Combining Structured and Unstructured Data Forpredictive Models A Deep Learning ApproachDocument10 pagesCombining Structured and Unstructured Data Forpredictive Models A Deep Learning ApproachSarmad N. MOHAMMEDNo ratings yet
- IRB Proposal - PSU Aorta NLP ProjectDocument39 pagesIRB Proposal - PSU Aorta NLP Projectjhk0428No ratings yet
- Heart Attack Predictions Using Machine LearningDocument8 pagesHeart Attack Predictions Using Machine LearningIJRASETPublicationsNo ratings yet
- Predicting Heart Attacks and Anxiety Using AIDocument7 pagesPredicting Heart Attacks and Anxiety Using AIShirsendu JhaNo ratings yet
- Machine Learning Based Models To Support Decision Maki - 2021 - International JoDocument7 pagesMachine Learning Based Models To Support Decision Maki - 2021 - International JobasubuetNo ratings yet
- (IJCST-V11I3P11) :Kalaiselvi.P, Vasanth.G, Aravinth.P, Elamugilan.A, Prasanth.SDocument4 pages(IJCST-V11I3P11) :Kalaiselvi.P, Vasanth.G, Aravinth.P, Elamugilan.A, Prasanth.SEighthSenseGroupNo ratings yet
- Second Progres ReportDocument10 pagesSecond Progres ReportManish RajNo ratings yet
- Paper 8846Document4 pagesPaper 8846IJARSCT JournalNo ratings yet
- Cardiac Attack Prediction Using MLDocument10 pagesCardiac Attack Prediction Using MLC RAHUL RAO.571No ratings yet
- Fuzzy Inference SystemDocument9 pagesFuzzy Inference SystemramadwidodoNo ratings yet
- A Prediction of Heart Disease Using Machine Learning AlgorithmsDocument8 pagesA Prediction of Heart Disease Using Machine Learning AlgorithmsNowreen HaqueNo ratings yet
- Eng p3 Heartdisease Forecasting-V7Document25 pagesEng p3 Heartdisease Forecasting-V7Cevi HerdianNo ratings yet
- AI in MedicineDocument4 pagesAI in MedicinemjNo ratings yet
- Predicting Heart Disease Using Machine Learning AlgorithmsDocument6 pagesPredicting Heart Disease Using Machine Learning AlgorithmstechieNo ratings yet
- A Machine Learning Algorithm To Identify Patients With Tibial Shaft Fractures at Risk For Infection After Operative TreatmentDocument9 pagesA Machine Learning Algorithm To Identify Patients With Tibial Shaft Fractures at Risk For Infection After Operative TreatmentarchchayaNo ratings yet
- Analysis of Hybrid Machine Learning Algorithm For Heart Disease PredictionDocument7 pagesAnalysis of Hybrid Machine Learning Algorithm For Heart Disease PredictionIJRASETPublicationsNo ratings yet
- 2nd Review ReportDocument6 pages2nd Review ReportHarshNo ratings yet
- 3806 Disease Prediction by Using Machine Learning PDFDocument6 pages3806 Disease Prediction by Using Machine Learning PDFJhon tNo ratings yet
- Automated Prediction of Brain Stroke Disease Classification Using Machine Learning Algorithm TechniquesDocument8 pagesAutomated Prediction of Brain Stroke Disease Classification Using Machine Learning Algorithm TechniquesIJRASETPublicationsNo ratings yet
- IJCRT2106047Document5 pagesIJCRT2106047fakok62897No ratings yet
- Heart Disease rp5Document15 pagesHeart Disease rp5EkanshNo ratings yet
- GJHS 8 152Document6 pagesGJHS 8 152Ika PuspitaNo ratings yet
- Ferro 2009Document7 pagesFerro 2009Carlos RiquelmeNo ratings yet
- Disease Prediction and Treatment Recommendation Using Machine LearningDocument8 pagesDisease Prediction and Treatment Recommendation Using Machine LearningIJRASETPublicationsNo ratings yet
- 1 s2.0 S105230572300006X MainDocument14 pages1 s2.0 S105230572300006X MainIda Ayu Trisna DewiNo ratings yet
- Ewss PDFDocument6 pagesEwss PDFChintia Meliana Kathy SiraitNo ratings yet
- Thesis Summary 1Document5 pagesThesis Summary 1RAJANNo ratings yet
- JOCC - Volume 2 - Issue 1 - Pages 50-65Document16 pagesJOCC - Volume 2 - Issue 1 - Pages 50-65Ananya DhuriaNo ratings yet
- 1 s2.0 S1532046420302768 MainDocument10 pages1 s2.0 S1532046420302768 MainDenzo NaldaNo ratings yet
- Heart Disease Prediction Using Machine LearningDocument4 pagesHeart Disease Prediction Using Machine LearningIJRASETPublicationsNo ratings yet
- Breaking The Breach in Latin America: A Pilot Study of Mechanical Thrombectomy in The Public Healthcare System in ChileDocument5 pagesBreaking The Breach in Latin America: A Pilot Study of Mechanical Thrombectomy in The Public Healthcare System in ChileDiego Rodríguez IrelandNo ratings yet
- Detection of Heart Diseases Using Machine Learning and Data MiningDocument7 pagesDetection of Heart Diseases Using Machine Learning and Data MiningazmiNo ratings yet
- Acuity of Undifferentiated Patients Entering The Emergency Care System: A Systematic ReviewDocument13 pagesAcuity of Undifferentiated Patients Entering The Emergency Care System: A Systematic ReviewBudi RiyantoPrabowoNo ratings yet
- Prediction of Stroke Using Deep Learning Model: October 2017Document10 pagesPrediction of Stroke Using Deep Learning Model: October 2017darNo ratings yet
- Heart Disease PredictionDocument15 pagesHeart Disease PredictionNIYATI KARANINo ratings yet
- Article BI Knowledge Grid Support For Treatment of Traumatic Brain Injury VictimsDocument10 pagesArticle BI Knowledge Grid Support For Treatment of Traumatic Brain Injury VictimsjlkazadiNo ratings yet
- ITPML32-FULLDocument19 pagesITPML32-FULLpushpamurugesan19622No ratings yet
- Báo KHDocument12 pagesBáo KHDUY VÕ HUỲNH NHẬTNo ratings yet
- The Psychology Book, Big Ideas Simply Explained - Nigel Benson PDFDocument354 pagesThe Psychology Book, Big Ideas Simply Explained - Nigel Benson PDFDuck98% (96)
- 03 - Biosignal CharacteristicsDocument46 pages03 - Biosignal CharacteristicsdarNo ratings yet
- Biomedical Signals & SystemsDocument16 pagesBiomedical Signals & SystemsMuhammad IrfanNo ratings yet
- Ralph Mcinerny A History of Western PhilosophyDocument846 pagesRalph Mcinerny A History of Western PhilosophyamgoforthNo ratings yet
- (Lisa - Wyatt - Knowlton - Cynthia - C. - Phillips) - The Logic Model GuidebookDocument191 pages(Lisa - Wyatt - Knowlton - Cynthia - C. - Phillips) - The Logic Model GuidebookdarNo ratings yet
- Flash Memories: Detlev RichterDocument287 pagesFlash Memories: Detlev RichterdarNo ratings yet
- A Course of Pure MathematicsDocument587 pagesA Course of Pure MathematicsdarNo ratings yet
- 20200120KU SNU Joint ProgramDocument2 pages20200120KU SNU Joint ProgramdarNo ratings yet
- SNU-Kyushu Joint Symposium on Materials ChemistryDocument2 pagesSNU-Kyushu Joint Symposium on Materials ChemistrydarNo ratings yet
- An Integrated Machine Learning Approach To Stroke PredictionDocument9 pagesAn Integrated Machine Learning Approach To Stroke PredictiondarNo ratings yet
- Scholarship at Uwindsor Scholarship at UwindsorDocument85 pagesScholarship at Uwindsor Scholarship at UwindsordarNo ratings yet
- ML Approach to Stroke Risk Prediction Achieves 0.72 AUCDocument7 pagesML Approach to Stroke Risk Prediction Achieves 0.72 AUCdarNo ratings yet
- Limit Scaling of MosfetDocument32 pagesLimit Scaling of MosfetdarNo ratings yet
- Classification of Ischemic Stroke Using Machine Learning AlgorithmsDocument6 pagesClassification of Ischemic Stroke Using Machine Learning AlgorithmsdarNo ratings yet
- 1 - STM32Cube Overview - HAL Package and STM32CubeMXDocument50 pages1 - STM32Cube Overview - HAL Package and STM32CubeMXdarNo ratings yet
- Hands OnPythonTutorialDocument191 pagesHands OnPythonTutorialtdysarz100% (1)
- Prediction of Stroke Using Deep Learning Model: October 2017Document10 pagesPrediction of Stroke Using Deep Learning Model: October 2017darNo ratings yet
- 0 - STM32 ASEAN Workshop Installation InstructionsDocument10 pages0 - STM32 ASEAN Workshop Installation InstructionsdarNo ratings yet
- STM32CubeMX DocumentationDocument319 pagesSTM32CubeMX DocumentationRefik Zaimovic100% (1)
- 2 - Demo - STM32CubeMX Initialization Code Generation PDFDocument43 pages2 - Demo - STM32CubeMX Initialization Code Generation PDFdarNo ratings yet
- Karayilan 2017Document5 pagesKarayilan 2017darNo ratings yet
- WM8731 PDFDocument64 pagesWM8731 PDFRAMON JARAMILLO MARTINEZNo ratings yet
- Jetson Nano Developer Kit: User GuideDocument24 pagesJetson Nano Developer Kit: User GuideDARSHAN GNo ratings yet
- Rani ThesisDocument101 pagesRani ThesisRatan KotipalliNo ratings yet
- Data Retention Behavior of A Sonos Type Twobit Storage Flash MemDocument4 pagesData Retention Behavior of A Sonos Type Twobit Storage Flash MemdarNo ratings yet
- UM2237 STM32CubeProgrammer Software DescriptionDocument39 pagesUM2237 STM32CubeProgrammer Software DescriptiondarNo ratings yet
- JJAP2006Feb SangsuDocument5 pagesJJAP2006Feb SangsudarNo ratings yet
- Ijet 15714Document4 pagesIjet 15714darNo ratings yet
- Programming P89V51 Microcontroller to Control Seven Segment DisplayDocument5 pagesProgramming P89V51 Microcontroller to Control Seven Segment DisplaysrgperumalNo ratings yet
- Oracle Fusion Applications: An OverviewDocument32 pagesOracle Fusion Applications: An Overviewt prasanth reddyNo ratings yet
- Face Recognition Using Eigenfaces Seminar ReportDocument30 pagesFace Recognition Using Eigenfaces Seminar ReportVihang PattiwarNo ratings yet
- Perception 1.22.0 Release Notes Support of Transport XDocument17 pagesPerception 1.22.0 Release Notes Support of Transport Xamerinoa31No ratings yet
- Nokia Smartphone Security Maintenance Release SummaryDocument4 pagesNokia Smartphone Security Maintenance Release SummaryDel ReyNo ratings yet
- BSNL Offers 3G Mobile Internet - How To Activate BSNL 3G or 2G Data Plan in Mobile Phone - Telecom News Plans and Customer CareDocument26 pagesBSNL Offers 3G Mobile Internet - How To Activate BSNL 3G or 2G Data Plan in Mobile Phone - Telecom News Plans and Customer CarePemmasaniSrinivasNo ratings yet
- Sony HR ProblemsDocument20 pagesSony HR ProblemskingjanuariusNo ratings yet
- 18hp5a0106 PPT 1Document37 pages18hp5a0106 PPT 1Chelluri Lokesh100% (1)
- Met Gazette 1 - CorrectedDocument28 pagesMet Gazette 1 - CorrectedMariana BobadillaNo ratings yet
- Aptio ™ Text Setup Environment (TSE) User ManualDocument42 pagesAptio ™ Text Setup Environment (TSE) User ManualArthur BarbosaNo ratings yet
- Apple's History, Products, Brand Value and Marketing Strategies in 40 CharactersDocument33 pagesApple's History, Products, Brand Value and Marketing Strategies in 40 CharactersYogendra ShuklaNo ratings yet
- OCAJP Oracle Certified Associate Java SE 8 Programmer Practice Exams (Mitchell Glenn) (Z-Library)Document3,004 pagesOCAJP Oracle Certified Associate Java SE 8 Programmer Practice Exams (Mitchell Glenn) (Z-Library)lenin12No ratings yet
- Huawei BBPDocument8 pagesHuawei BBPEmreNo ratings yet
- Connect Your PC/Laptop to the Router in 3 Easy StepsDocument6 pagesConnect Your PC/Laptop to the Router in 3 Easy StepsPradyot H AdaviNo ratings yet
- REN R01us0165ej0120-Rh850g3kh MAN 20161222Document384 pagesREN R01us0165ej0120-Rh850g3kh MAN 20161222Jimmy ChenNo ratings yet
- Assessment BSBPMG532 Manage Project Quality Task 2 PDFDocument19 pagesAssessment BSBPMG532 Manage Project Quality Task 2 PDFtarun SharmaNo ratings yet
- CoolMastePro Submittal Data-Sheet For The US MarketDocument2 pagesCoolMastePro Submittal Data-Sheet For The US Marketalejandro pimientaNo ratings yet
- Bahasa Inggris "Soal Pada Unit 14 Hal 100 Unit A Dan B"Document5 pagesBahasa Inggris "Soal Pada Unit 14 Hal 100 Unit A Dan B"anedoNo ratings yet
- Manual enDocument88 pagesManual enyenorig120No ratings yet
- Ricoh 4055 PDFDocument1,280 pagesRicoh 4055 PDFPham Nguyen Hoang Minh100% (1)
- Bana Bir Soygun Yaz 2 (2018) - IMDbDocument3 pagesBana Bir Soygun Yaz 2 (2018) - IMDbTrojaikeNo ratings yet
- NoodleTools MLA FAQDocument8 pagesNoodleTools MLA FAQpamelalibrarianNo ratings yet
- GENGDocument7 pagesGENGAizat RomainoNo ratings yet
- Update IP Particulars Through IP Portal ESICDocument55 pagesUpdate IP Particulars Through IP Portal ESICamittradaNo ratings yet
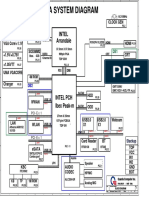
- UM8 UMA system diagram overviewDocument46 pagesUM8 UMA system diagram overviewReballing BogotaNo ratings yet
- 1 Microscopy CanvasDocument11 pages1 Microscopy CanvasRokia BenzergaNo ratings yet
- Comp3301 OutlineDocument5 pagesComp3301 OutlinenenesNo ratings yet
- Octal and Hexadecimal Number Systems: © 2014 Project Lead The Way, Inc. Digital ElectronicsDocument25 pagesOctal and Hexadecimal Number Systems: © 2014 Project Lead The Way, Inc. Digital ElectronicsAJNo ratings yet
- Examen TP Cisco Final Device Names TableDocument5 pagesExamen TP Cisco Final Device Names TableHamma RezzagNo ratings yet
- Java Script QuestionsDocument4 pagesJava Script QuestionsFazal-E- MalikNo ratings yet