You might also like
- Photosynthesis Interactive NotebookDocument26 pagesPhotosynthesis Interactive NotebookAshley Farnham67% (3)
- The Microbiology of Skin, Soft Tissue, Bone and Joint InfectionsFrom EverandThe Microbiology of Skin, Soft Tissue, Bone and Joint InfectionsNo ratings yet
- Isolation and Identification of Dermatophytes Causing DermatophytosisDocument15 pagesIsolation and Identification of Dermatophytes Causing Dermatophytosisabznaim420No ratings yet
- ClinDermatolRev133-5811533 160835Document9 pagesClinDermatolRev133-5811533 160835rehanaNo ratings yet
- 35429-Article Text-126139-2-10-20180206Document5 pages35429-Article Text-126139-2-10-20180206Robertus RonnyNo ratings yet
- Clinicomycological Profile of Superficial Fungal Infections Caused by Dermatophytes in A Tertiary Care Centre of North IndiaDocument8 pagesClinicomycological Profile of Superficial Fungal Infections Caused by Dermatophytes in A Tertiary Care Centre of North IndiaasfwegereNo ratings yet
- Microscopic Evaluation, Molecular Identification, Antifungal Dematiaceous KeratitisDocument11 pagesMicroscopic Evaluation, Molecular Identification, Antifungal Dematiaceous KeratitisAnonymous argZ1ZNo ratings yet
- Mycetoma Laboratory Diagnosis Review Article740Document17 pagesMycetoma Laboratory Diagnosis Review Article740hapipahNo ratings yet
- Mycetoma Laboratory Diagnosis Review Article740Document17 pagesMycetoma Laboratory Diagnosis Review Article740HapipahNo ratings yet
- Jof 03 00017Document10 pagesJof 03 00017Asterlita RyaneNo ratings yet
- Evaluation of A Commercial PCR Test For The Diagnosis of Dermatophyte Nail InfectionsDocument7 pagesEvaluation of A Commercial PCR Test For The Diagnosis of Dermatophyte Nail Infectionsckcy ahaiNo ratings yet
- Jof 07 00526Document14 pagesJof 07 00526Aishah FarihaNo ratings yet
- Kredics Et Al 2015Document18 pagesKredics Et Al 2015Palanisamy ManikandanNo ratings yet
- Jurnal TC KohDocument4 pagesJurnal TC KohariefNo ratings yet
- Dermatophytosis in Bhairahawa, Nepal: Prevalence and Resistance Pattern of Dermatophyte SpeciesDocument9 pagesDermatophytosis in Bhairahawa, Nepal: Prevalence and Resistance Pattern of Dermatophyte SpeciesSubhas KarnaNo ratings yet
- Tinea Infections: Changing Face or Neglected?: Laura Atzori, Laura Pizzatti and Monica PauDocument7 pagesTinea Infections: Changing Face or Neglected?: Laura Atzori, Laura Pizzatti and Monica PauRisma AnjelinaNo ratings yet
- The Susceptibility of Pathogens Associated With Acne Vulgaris To AntibioticsDocument7 pagesThe Susceptibility of Pathogens Associated With Acne Vulgaris To AntibioticsMuhammad AdiNo ratings yet
- Miyajima 2013Document7 pagesMiyajima 2013Siti Bellia Arafah XndNo ratings yet
- 1 s2.0 S1286457912001918 MainDocument8 pages1 s2.0 S1286457912001918 Mainabznaim420No ratings yet
- EJMCM - Volume 7 - Issue 11 - Pages 9184-9190Document7 pagesEJMCM - Volume 7 - Issue 11 - Pages 9184-9190Akshay BeradNo ratings yet
- Diagnosis of Dermatophytosis Using Molecular BiologyDocument10 pagesDiagnosis of Dermatophytosis Using Molecular BiologyJosias SagcheNo ratings yet
- Causative Fungi and Treatment Outcome of Dematiaceous Fungal Keratitis in North India. 2019Document7 pagesCausative Fungi and Treatment Outcome of Dematiaceous Fungal Keratitis in North India. 2019Anonymous argZ1ZNo ratings yet
- Combined Steroid and AntifungalDocument9 pagesCombined Steroid and AntifungalMega RafikaNo ratings yet
- Jurnal Eucast LainnyaDocument228 pagesJurnal Eucast Lainnyaonly taaNo ratings yet
- Identification !!!!Document6 pagesIdentification !!!!Hasnae HassaniNo ratings yet
- Management of Tinea Corporis, Tinea Cruris, and Tinea Pedis: A Comprehensive ReviewDocument19 pagesManagement of Tinea Corporis, Tinea Cruris, and Tinea Pedis: A Comprehensive ReviewYovitaNo ratings yet
- A Cross Sectional Study To Observe The Diversity of Fungal Species in Onychomycosis Isolated From A Tertiary Care Hospital in KarachiDocument4 pagesA Cross Sectional Study To Observe The Diversity of Fungal Species in Onychomycosis Isolated From A Tertiary Care Hospital in KarachiMini LaksmiNo ratings yet
- PCR Tugas Diagmol 2Document9 pagesPCR Tugas Diagmol 2Laboratorium RSUDKOTANGNo ratings yet
- Manikandan Et AlDocument10 pagesManikandan Et AlPalanisamy ManikandanNo ratings yet
- Moshirfar Et Al. - 2019 - Biological Staining and Culturing in Infectious KeDocument7 pagesMoshirfar Et Al. - 2019 - Biological Staining and Culturing in Infectious KesyramadhantiNo ratings yet
- Cshperspectmed HFP A019299Document14 pagesCshperspectmed HFP A019299windaNo ratings yet
- Epidemilogia de OnicomicosesDocument12 pagesEpidemilogia de OnicomicosesJoão Gabriel Giaretta AvesaniNo ratings yet
- Anuradha NDocument4 pagesAnuradha NIJAMNo ratings yet
- Epidemiological Characterization of Dermatomycosis in EthiopiaDocument7 pagesEpidemiological Characterization of Dermatomycosis in EthiopiaMini LaksmiNo ratings yet
- A Study of Dermatomycoses: Manuscript InfoDocument7 pagesA Study of Dermatomycoses: Manuscript InfoCorry ZalukhuNo ratings yet
- Diagnostic Techniques of Soil-Transmitted Helminths: Impact On Control MeasuresDocument17 pagesDiagnostic Techniques of Soil-Transmitted Helminths: Impact On Control MeasuresBrionelle DumelodNo ratings yet
- Jjurnal InternasionalDocument4 pagesJjurnal Internasionalckcy ahaiNo ratings yet
- Artigo ÉrickaDocument11 pagesArtigo Érickaiven87No ratings yet
- Dermatophytes and Bacterial Superinfections in Tinea Pedis Patients at Haji Adam Malik Central Hospital, Medan-IndonesiaDocument5 pagesDermatophytes and Bacterial Superinfections in Tinea Pedis Patients at Haji Adam Malik Central Hospital, Medan-IndonesiaKapindraNo ratings yet
- Dermatophytosis in Northern AfricaDocument8 pagesDermatophytosis in Northern Africaabznaim420No ratings yet
- 5 Goffar Deardo SaragihDocument5 pages5 Goffar Deardo SaragihJoe BitchNo ratings yet
- Tinea Pedis An Update 1Document6 pagesTinea Pedis An Update 1putrinurulapriliaNo ratings yet
- Art:10.1186/s12879 016 1593 0Document6 pagesArt:10.1186/s12879 016 1593 0Tasalina Yohana Parameswari GustamNo ratings yet
- The Foot: Original ArticleDocument5 pagesThe Foot: Original ArticleKarinaayu SerinNo ratings yet
- Tinea Pedis An UpdateDocument5 pagesTinea Pedis An UpdateRahmat MuliaNo ratings yet
- 1 PBDocument11 pages1 PBMega RebbekaNo ratings yet
- Antifungal Efficacy of Lasers Against Dermatophytes and Yeasts in VitroDocument7 pagesAntifungal Efficacy of Lasers Against Dermatophytes and Yeasts in VitroCyberNo ratings yet
- Muhilan Jegadeesan's Clinico-Etiological Study of Tinea Corporis: Emergence of Trichophyton MentagrophytesDocument5 pagesMuhilan Jegadeesan's Clinico-Etiological Study of Tinea Corporis: Emergence of Trichophyton MentagrophytesjmuhilanNo ratings yet
- Jof 06 00216 v2Document18 pagesJof 06 00216 v2Grace Yuni Soesanti MhNo ratings yet
- Evaluation of Culture Media For The Rapid Isolation of DermatophytesDocument4 pagesEvaluation of Culture Media For The Rapid Isolation of DermatophytesIOSRjournalNo ratings yet
- Antifungal Susceptibility Pattern Against Dermatophytic Strains Isolated From Humans in Anambra State, NigeriaDocument8 pagesAntifungal Susceptibility Pattern Against Dermatophytic Strains Isolated From Humans in Anambra State, NigeriaIJAERS JOURNALNo ratings yet
- PCR Application in Infectious Keratitis DiagnosisDocument4 pagesPCR Application in Infectious Keratitis DiagnosisFriska Amanda Nur LailiyahNo ratings yet
- Severe DermatoDocument13 pagesSevere DermatoadriantiariNo ratings yet
- Skin Immunity To Dermatophytes: From Experimental Infection Models To Human DiseaseDocument16 pagesSkin Immunity To Dermatophytes: From Experimental Infection Models To Human Diseaseirwan junNo ratings yet
- Mesotrerapia Protocolo Seguro y Manejo de ComplicacionesDocument5 pagesMesotrerapia Protocolo Seguro y Manejo de ComplicacionesOrlando GaduNo ratings yet
- Feline DermatophytosisDocument13 pagesFeline Dermatophytosisanisofea rosnizamNo ratings yet
- IndianDermatolOnlineJ115747-8523267 022203Document6 pagesIndianDermatolOnlineJ115747-8523267 022203Zefqy Wahyu MardianaNo ratings yet
- Research Center Diagnosis of Pulmonary Tuberculosis - How Rapid Can It Get?Document10 pagesResearch Center Diagnosis of Pulmonary Tuberculosis - How Rapid Can It Get?lenysfaridaNo ratings yet
- 25.antifungal NigamPKDocument10 pages25.antifungal NigamPKnurulunismuhNo ratings yet
- Topical Corticosteroids and Fungal Keratitis: A Review of The Literature and Case SeriesDocument11 pagesTopical Corticosteroids and Fungal Keratitis: A Review of The Literature and Case SeriesRiyan PratamaNo ratings yet
- Clinically Relevant Mycoses: A Practical ApproachFrom EverandClinically Relevant Mycoses: A Practical ApproachElisabeth PresterlNo ratings yet
- Priorities For Research and Control of Cestode Zoonoses in AsiaDocument11 pagesPriorities For Research and Control of Cestode Zoonoses in AsiahansmeetNo ratings yet
- Neurocysticercosis: A Review: January 2007Document6 pagesNeurocysticercosis: A Review: January 2007hansmeetNo ratings yet
- Neurocysticercosis: A Disease of Neglect: Abhishek Mewara, Kapil Goyal, Rakesh SehgalDocument9 pagesNeurocysticercosis: A Disease of Neglect: Abhishek Mewara, Kapil Goyal, Rakesh SehgalhansmeetNo ratings yet
- Malassezia Pachydermatis: Carriage in Dog OwnersDocument6 pagesMalassezia Pachydermatis: Carriage in Dog OwnershansmeetNo ratings yet
- Chapter 89: Part X Infectious DisordersDocument4 pagesChapter 89: Part X Infectious DisordershansmeetNo ratings yet
- Kuntsi Vaattovaara2002 PDFDocument6 pagesKuntsi Vaattovaara2002 PDFhansmeetNo ratings yet
- Shelter Hospital Mode: How Do We Prevent COVID-19 Hospital-Acquired Infection?Document2 pagesShelter Hospital Mode: How Do We Prevent COVID-19 Hospital-Acquired Infection?hansmeetNo ratings yet
- Old and New Vaccine Approaches: Ruth Arnon, Tamar Ben-YedidiaDocument10 pagesOld and New Vaccine Approaches: Ruth Arnon, Tamar Ben-YedidiahansmeetNo ratings yet
- Approaches To Improve Chemically Defined Synthetic Peptide VaccinesDocument8 pagesApproaches To Improve Chemically Defined Synthetic Peptide VaccineshansmeetNo ratings yet
- Design of A Recombinant Hepatitis B Vaccine Based On Stably Binding Hlai Peptides 2167 7956.1000120Document4 pagesDesign of A Recombinant Hepatitis B Vaccine Based On Stably Binding Hlai Peptides 2167 7956.1000120hansmeetNo ratings yet
- Review: A Decade of RiboswitchesDocument8 pagesReview: A Decade of RiboswitcheshansmeetNo ratings yet
- 1 Bacterial InvasionDocument13 pages1 Bacterial InvasionhansmeetNo ratings yet
- DiseaseDocument100 pagesDiseasehansmeetNo ratings yet
- Antibiotics in Veterinary UseDocument83 pagesAntibiotics in Veterinary Usehansmeet100% (1)
- Bottle JawDocument35 pagesBottle Jawhansmeet100% (1)
- Diseases of Neonates in AnimalsDocument35 pagesDiseases of Neonates in AnimalshansmeetNo ratings yet
- Grade-8 Lesson PlanDocument7 pagesGrade-8 Lesson PlanPristine Aila Robles100% (1)
- Seed Technology - Trad2 (1-5)Document5 pagesSeed Technology - Trad2 (1-5)Jaru Jacky100% (1)
- Sea-Shore Food Chains and WebDocument2 pagesSea-Shore Food Chains and WebJohn OsborneNo ratings yet
- Activity Worksheet: ExampleDocument6 pagesActivity Worksheet: ExampleNicole LagadoNo ratings yet
- IGCSE Biology Section 1 Lesson 1Document44 pagesIGCSE Biology Section 1 Lesson 1Zhuko Suko AdiNo ratings yet
- GR 11 Life Sciences IEB 3 in 1 ExtractsDocument16 pagesGR 11 Life Sciences IEB 3 in 1 ExtractsMfago MohosetjiNo ratings yet
- A Brief History of MicrobiologyDocument54 pagesA Brief History of MicrobiologyVia SongcalNo ratings yet
- Curriculum Vitae 1. Personal DetailsDocument8 pagesCurriculum Vitae 1. Personal DetailsRadha PriyadarshiniNo ratings yet
- Biology B: Pearson Edexcel Level 3 GCEDocument107 pagesBiology B: Pearson Edexcel Level 3 GCEaliceNo ratings yet
- Tala Zeer - Meisosi Revision Worksheet Copy 2Document2 pagesTala Zeer - Meisosi Revision Worksheet Copy 2Tala ZeerNo ratings yet
- VermiGrow TeaDocument3 pagesVermiGrow TeaCandace RobertsNo ratings yet
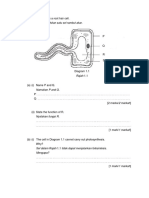
- Rajah 1.1 Menunjukkan Satu Sel Rambut AkarDocument29 pagesRajah 1.1 Menunjukkan Satu Sel Rambut AkarAzfar SyahmiNo ratings yet
- Animal Scientific NamesDocument4 pagesAnimal Scientific NamesAnjaliNo ratings yet
- Classification of MicroorganismsDocument37 pagesClassification of MicroorganismsKenix ChanNo ratings yet
- Chromosomes: © 2016 Paul BillietDocument25 pagesChromosomes: © 2016 Paul BillietClaude UbaNo ratings yet
- Grade: G9 Subject: Biology Topic: Cell DivisionDocument5 pagesGrade: G9 Subject: Biology Topic: Cell DivisionKhyra ScottNo ratings yet
- Theories of Shoot Apical Meristem OKOKOKDocument8 pagesTheories of Shoot Apical Meristem OKOKOKShameel PervezNo ratings yet
- Surirella - Diatoms of The United StatesDocument3 pagesSurirella - Diatoms of The United StatesAlexidosNo ratings yet
- AK-Homework-21.3 - 21.4 2Document3 pagesAK-Homework-21.3 - 21.4 2Remas NBNo ratings yet
- Homo SapiensDocument3 pagesHomo SapiensAlvin TorioNo ratings yet
- Lecture 1 FungiDocument23 pagesLecture 1 FungiDragon Gie30No ratings yet
- Postulat KochDocument11 pagesPostulat KochputriNo ratings yet
- Science 10 3rd TQDocument5 pagesScience 10 3rd TQWashima Bentulina SabtalNo ratings yet
- Microbial Taxonomy and Phylogeny PATINGA CHRISTIAN V.Document2 pagesMicrobial Taxonomy and Phylogeny PATINGA CHRISTIAN V.Christian PatingaNo ratings yet
- Cell DifferentiationDocument26 pagesCell DifferentiationQusai Haimone100% (1)
- Winter Wheat Production Manual CH 10: Growth Stages of WheatDocument15 pagesWinter Wheat Production Manual CH 10: Growth Stages of Wheatit helpdesk smarkNo ratings yet
- Reuse DNA Spin ColumnDocument6 pagesReuse DNA Spin ColumnashueinNo ratings yet
- Blue-White Colony ScreeningDocument1 pageBlue-White Colony ScreeningShalizma Khandaker OrniNo ratings yet
- Family: Solanaceae (Potato Family)Document2 pagesFamily: Solanaceae (Potato Family)Optimistic MindNo ratings yet