You might also like
- Relative Biocompatibility of Micro-Hybrid and Nano-Hybrid Light-Activated Composite ResinsDocument6 pagesRelative Biocompatibility of Micro-Hybrid and Nano-Hybrid Light-Activated Composite ResinsAhmed Febri Hertama 'Sinosuke'No ratings yet
- In Vitro and in Vivo Stuides On The Toxicity of Dental Resin ComponentsDocument9 pagesIn Vitro and in Vivo Stuides On The Toxicity of Dental Resin Componentssoho1303No ratings yet
- 11 CoDocument8 pages11 CoSaad LiaqatNo ratings yet
- The Effect of Extrusion and Injection Molding On Physical, Chemical, and Biological Properties of PLLAHAp Whiskers CompositesDocument14 pagesThe Effect of Extrusion and Injection Molding On Physical, Chemical, and Biological Properties of PLLAHAp Whiskers CompositesFellipe LavaquiNo ratings yet
- Materials: Cytotoxicity of Light-Cured Dental Materials According To Different Sample Preparation MethodsDocument12 pagesMaterials: Cytotoxicity of Light-Cured Dental Materials According To Different Sample Preparation MethodsSai KarthikNo ratings yet
- The Repair Bond Strength To Resin Matrix in Cured Resin Composites After Water AgingDocument8 pagesThe Repair Bond Strength To Resin Matrix in Cured Resin Composites After Water AgingJuan K. J. ShinNo ratings yet
- J Biomedical Materials Res - 2011 - GhasabanDocument9 pagesJ Biomedical Materials Res - 2011 - Ghasaban발라드님No ratings yet
- Heliyon: Md. Ruhul Amin, Mohammad Asaduzzaman Chowdhury, Md. Are Fin KowserDocument12 pagesHeliyon: Md. Ruhul Amin, Mohammad Asaduzzaman Chowdhury, Md. Are Fin KowserhmossNo ratings yet
- Green Synthesis of Stretchable Ethyl Cellulose Film Plasticized With Transertified Sunflower OilDocument12 pagesGreen Synthesis of Stretchable Ethyl Cellulose Film Plasticized With Transertified Sunflower Oililan chertokNo ratings yet
- Effect of Coconut Fiber Reinforcement On Mechanical Properties of Corn Starch BioplasticsDocument5 pagesEffect of Coconut Fiber Reinforcement On Mechanical Properties of Corn Starch BioplasticsMark Junnel PascuaNo ratings yet
- GO Nanocomposite Fibers Inhibit Bacterial GrowthDocument14 pagesGO Nanocomposite Fibers Inhibit Bacterial GrowthHiran ChathurangaNo ratings yet
- Hydroxyapatite Whiskers Based Resin Composite VersDocument9 pagesHydroxyapatite Whiskers Based Resin Composite VersUauahaNo ratings yet
- Microestructura 1Document8 pagesMicroestructura 1Luis FelixNo ratings yet
- HHS Public Access: Gelatin/Carboxymethyl Cellulose Mucoadhesive Films With Lysozyme: Development and CharacterizationDocument22 pagesHHS Public Access: Gelatin/Carboxymethyl Cellulose Mucoadhesive Films With Lysozyme: Development and CharacterizationGiffariNo ratings yet
- Nanofilled Resin Composite Properties and Clinical Performance - A ReviewDocument18 pagesNanofilled Resin Composite Properties and Clinical Performance - A ReviewInside Dentistry educationNo ratings yet
- Experimental Investigation of Mechanical & Thermal Properties of PCL Blended Graphene BiocompositesDocument19 pagesExperimental Investigation of Mechanical & Thermal Properties of PCL Blended Graphene BiocompositesCody LeeNo ratings yet
- 2013 Chitosan PEO Silica HybridsDocument10 pages2013 Chitosan PEO Silica HybridsEliton Medeiros Candido de MacêdoNo ratings yet
- 1-s2.0-S2212982024000325-mainDocument12 pages1-s2.0-S2212982024000325-mainmikeairdNo ratings yet
- Recent Advancement in Composites - A ReviewDocument4 pagesRecent Advancement in Composites - A ReviewMueed SazidNo ratings yet
- Mang BiopolymerDocument15 pagesMang BiopolymerLU LAM THIENNo ratings yet
- 10 1016@j Porgcoat 2019 02 007Document8 pages10 1016@j Porgcoat 2019 02 007hayet debbichNo ratings yet
- Biopolymer Films Synthesis and CharacterisationDocument5 pagesBiopolymer Films Synthesis and Characterisationrajmohanty5100No ratings yet
- Biomaterials With Potential Use in Bone Tissue RegDocument21 pagesBiomaterials With Potential Use in Bone Tissue RegIsworo RukmiNo ratings yet
- Polymer Testing: Material PropertiesDocument7 pagesPolymer Testing: Material PropertiesSoffi SyarofahNo ratings yet
- Highly Toughened and Transparent Biobased Epoxy Composites Reinforced with Cellulose NanofibrilsDocument13 pagesHighly Toughened and Transparent Biobased Epoxy Composites Reinforced with Cellulose Nanofibrilsmartina.cirronis96No ratings yet
- Biodegradable Polymer Matrix Nanocomposites For Tissue Engineering PDFDocument21 pagesBiodegradable Polymer Matrix Nanocomposites For Tissue Engineering PDFJuan Pablo BulaciosNo ratings yet
- Effect of Ramie Fabric Chemical Treatments On The Physical Properties of Thermoset Polylactic Acid (PLA) CompositesDocument13 pagesEffect of Ramie Fabric Chemical Treatments On The Physical Properties of Thermoset Polylactic Acid (PLA) Compositesadnan alfarisiNo ratings yet
- A Comparative Study of Bulk-Fill Composites - Degree of Conversion, Post-Gel Shrinkage and CytotoxicityDocument9 pagesA Comparative Study of Bulk-Fill Composites - Degree of Conversion, Post-Gel Shrinkage and CytotoxicityDiogo SimõesNo ratings yet
- Ramie Fibers PDFDocument7 pagesRamie Fibers PDFDian RestiNo ratings yet
- 10 1111@etp 12068Document15 pages10 1111@etp 12068AKSNo ratings yet
- Comparison of The Sealing Ability of Bioceramic Sealer Against Epoxy ResinDocument8 pagesComparison of The Sealing Ability of Bioceramic Sealer Against Epoxy ResinViC JasonNo ratings yet
- 28 Polymers 14 01818Document12 pages28 Polymers 14 01818sylwka.inoNo ratings yet
- Materials Science and Engineering C: Amir Nemati Hayati, S.M. Hosseinalipour, H.R. Rezaie, M.A. ShokrgozarDocument7 pagesMaterials Science and Engineering C: Amir Nemati Hayati, S.M. Hosseinalipour, H.R. Rezaie, M.A. ShokrgozarEmon BaruaNo ratings yet
- Microcapsule Effects on Mortar Properties and Self-HealingDocument17 pagesMicrocapsule Effects on Mortar Properties and Self-HealingDhruv ThakkarNo ratings yet
- Journal of Hazardous Materials: A A A BDocument9 pagesJournal of Hazardous Materials: A A A BAna-Marya RadionNo ratings yet
- Angew Chem Int Ed - 2005 - Klemm - Cellulose Fascinating Biopolymer and Sustainable Raw MaterialDocument36 pagesAngew Chem Int Ed - 2005 - Klemm - Cellulose Fascinating Biopolymer and Sustainable Raw MaterialJULIAEANENo ratings yet
- Polymer: Jun-Yong Park, Kyu-Hong Kyung, Kosuke Tsukada, Sae-Hoon Kim, Seimei ShiratoriDocument9 pagesPolymer: Jun-Yong Park, Kyu-Hong Kyung, Kosuke Tsukada, Sae-Hoon Kim, Seimei ShiratoriMovila IrinaNo ratings yet
- Article 1 TDMDocument10 pagesArticle 1 TDMSorgiusNo ratings yet
- Nanofilled Resin Composite Properties and Clinical Performance: A ReviewDocument18 pagesNanofilled Resin Composite Properties and Clinical Performance: A ReviewFransisca FeliciaNo ratings yet
- ChemosphereDocument13 pagesChemosphereyunpu jiaNo ratings yet
- Biomimetic Materials in Dentistry 2321 6212 1000188Document9 pagesBiomimetic Materials in Dentistry 2321 6212 1000188Bhoomika SikriNo ratings yet
- البحث السادسDocument10 pagesالبحث السادسMostafa Shaker El AasserNo ratings yet
- Characterization of Properties of Epoxy Sisal / Glass Fiber Reinforced Hybrid CompositeDocument7 pagesCharacterization of Properties of Epoxy Sisal / Glass Fiber Reinforced Hybrid CompositeMr. K.S. Raghul Asst Prof MECH100% (1)
- 2005 - CS PEO Cellular CompatibilityDocument9 pages2005 - CS PEO Cellular CompatibilityTiNo ratings yet
- 1 (In Vitro Evaluation of The Biological Effects of ACTIVA Kids BioACTIVE Restorative, Ionolux, and Riva Light Cure On Human Dental Pulp Stem Cells)Document11 pages1 (In Vitro Evaluation of The Biological Effects of ACTIVA Kids BioACTIVE Restorative, Ionolux, and Riva Light Cure On Human Dental Pulp Stem Cells)Cahyani CahyaniNo ratings yet
- Properties of A Dental Resin Composite With A Spherical Inorganic FillerDocument8 pagesProperties of A Dental Resin Composite With A Spherical Inorganic Fillermuchlis fauziNo ratings yet
- Fabrication and Characterization of Alginate-Based Films Functionalized With Nanostructured Lipid CarriersDocument12 pagesFabrication and Characterization of Alginate-Based Films Functionalized With Nanostructured Lipid CarriersMohammad Hamayoon NorriNo ratings yet
- N.S.N.H. Nizan, F.H. Zulkifli, H.A. Hamid and M.H. MazwirDocument6 pagesN.S.N.H. Nizan, F.H. Zulkifli, H.A. Hamid and M.H. MazwirFarah Hanani ZulkifliNo ratings yet
- Binary Grafted Chitosan Film Synthesis Characterization Antibacterial Activity and Prospects For Food PackagingDocument21 pagesBinary Grafted Chitosan Film Synthesis Characterization Antibacterial Activity and Prospects For Food PackagingRicardo Fajardo DíazNo ratings yet
- 1 s2.0 S0142941820301045 MainDocument9 pages1 s2.0 S0142941820301045 MainTHE MASTER SIDENo ratings yet
- Progress in Organic Coatings: Aparna Kadam, Manisha Pawar, Viresh Thamke, Omprakash YemulDocument5 pagesProgress in Organic Coatings: Aparna Kadam, Manisha Pawar, Viresh Thamke, Omprakash YemulRobi MaulanaNo ratings yet
- 1 s2.0 S2666893921001419 Main1Document9 pages1 s2.0 S2666893921001419 Main1jadeshades12No ratings yet
- Materials: Interface Bond Improvement of Sisal Fibre Reinforced Polylactide Composites With Added Epoxy OligomerDocument22 pagesMaterials: Interface Bond Improvement of Sisal Fibre Reinforced Polylactide Composites With Added Epoxy Oligomerali aliNo ratings yet
- Root End Filling MaterialsDocument9 pagesRoot End Filling MaterialsRuchi ShahNo ratings yet
- Deshmukh 2021Document10 pagesDeshmukh 2021isukim0626No ratings yet
- Preparation of Laminated Poly - Caprolactone - Gelatin-Hydroxyapatite Nanocomposite Scaffold Bioengineered Via Compound Techniques For Bone SubstitutioDocument12 pagesPreparation of Laminated Poly - Caprolactone - Gelatin-Hydroxyapatite Nanocomposite Scaffold Bioengineered Via Compound Techniques For Bone Substitutioahmed titoNo ratings yet
- 1 Muhammad Husaini Amir Bin HusseinDocument31 pages1 Muhammad Husaini Amir Bin HusseinGreen ManNo ratings yet
- 10 1016@j Carbpol 2017 02 092Document23 pages10 1016@j Carbpol 2017 02 092agus priyantoNo ratings yet
- Chitosan Nanocomposites Based On Distinct Inorganic Fillers For Biomedical ApplicationsDocument18 pagesChitosan Nanocomposites Based On Distinct Inorganic Fillers For Biomedical ApplicationsYusliana SidaurukNo ratings yet
- Studiu 2-Eveline PutzeysDocument9 pagesStudiu 2-Eveline PutzeysLavinia GheorghitaNo ratings yet
- TetricEvoCeram-The Influence of Water Sorption of Dental Light-Cured Composites On Shrinkage StressDocument14 pagesTetricEvoCeram-The Influence of Water Sorption of Dental Light-Cured Composites On Shrinkage StressLavinia GheorghitaNo ratings yet
- Preventie Curs 8 PDFDocument109 pagesPreventie Curs 8 PDFLavinia GheorghitaNo ratings yet
- Preventie Curs 8 PDFDocument109 pagesPreventie Curs 8 PDFLavinia GheorghitaNo ratings yet
- Fuente As-IDocument4 pagesFuente As-IadalaviNo ratings yet
- Strengthening HIV Care in Africa CertificateDocument7 pagesStrengthening HIV Care in Africa CertificateMaiga Ayub HusseinNo ratings yet
- PCS-9656 Arc ProtectionDocument3 pagesPCS-9656 Arc ProtectionganeshNo ratings yet
- RESOLUTION 2022-08 Denial of Setback VarianceDocument5 pagesRESOLUTION 2022-08 Denial of Setback VarianceMatt McKinneyNo ratings yet
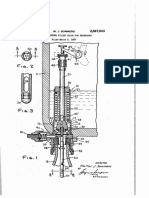
- Counter-pressure filler valve for beveragesDocument3 pagesCounter-pressure filler valve for beveragesbimalishaNo ratings yet
- Yıldız Technical University - Program Information Form - Page 1/9Document9 pagesYıldız Technical University - Program Information Form - Page 1/9Elsaadawi MohamedNo ratings yet
- General Biology 1 - Power Point Presentation (Group 8)Document14 pagesGeneral Biology 1 - Power Point Presentation (Group 8)Archan Dom ReyesNo ratings yet
- E 242 - 95 R00 - Rti0mi1sruq - PDFDocument5 pagesE 242 - 95 R00 - Rti0mi1sruq - PDFLeón SuárezNo ratings yet
- EWC661 TITLE: Dietary Habits During Term Time Among University Students. Background of StudyDocument4 pagesEWC661 TITLE: Dietary Habits During Term Time Among University Students. Background of StudyfarinaazmiNo ratings yet
- NBME 22 OfflineDocument200 pagesNBME 22 OfflineGautham Kanagala86% (14)
- Apcosil 605Document1 pageApcosil 605rihtak123No ratings yet
- Roof Construction Dr. Fixit Newcoat PDFDocument1 pageRoof Construction Dr. Fixit Newcoat PDFRishabh VijayNo ratings yet
- Conveying Water Distribution SEODocument90 pagesConveying Water Distribution SEOmichelghanemNo ratings yet
- Edwards Auto 306 CharacteristicsDocument4 pagesEdwards Auto 306 CharacteristicsJuan Antonio Rubio-LaraNo ratings yet
- Earth First! Climbers Guild Vol. 2Document16 pagesEarth First! Climbers Guild Vol. 2CascadiaDefenders100% (2)
- Uber ComplaintDocument17 pagesUber ComplaintMichael TobinNo ratings yet
- Ufara QasrinDocument14 pagesUfara Qasrinroni setiawanNo ratings yet
- Chemistry Units 8 12Document29 pagesChemistry Units 8 12reg speckNo ratings yet
- Water For Injections BP: What Is in This Leaflet?Document2 pagesWater For Injections BP: What Is in This Leaflet?Mohamed OmerNo ratings yet
- GMP TD Ar FPL 11033Document1 pageGMP TD Ar FPL 11033Sammy NguyenNo ratings yet
- Herbal MedicineDocument38 pagesHerbal MedicineBurei KouNo ratings yet
- Notes Form 2 Chapter 4Document4 pagesNotes Form 2 Chapter 4lembu_sihat7783% (6)
- Pre-Final Exam in Audit 2-3Document5 pagesPre-Final Exam in Audit 2-3Shr BnNo ratings yet
- Cerberus PRO Product Catalog: Fire Safety Products and AccessoriesDocument253 pagesCerberus PRO Product Catalog: Fire Safety Products and AccessoriesleonardoleitealertaNo ratings yet
- General Conditions of Contracts For NLNG 2018Document28 pagesGeneral Conditions of Contracts For NLNG 2018AF Dowell MirinNo ratings yet
- F.E. Campbell - Sweet Slavery - HIT 139Document115 pagesF.E. Campbell - Sweet Slavery - HIT 139HokusLocus67% (3)
- Preparation of Starch Nanoparticles in A New Ionic Liquid-in-Oil MicroemulsionDocument12 pagesPreparation of Starch Nanoparticles in A New Ionic Liquid-in-Oil MicroemulsionPaula NancyNo ratings yet
- Sakshijain75.Final ProDocument46 pagesSakshijain75.Final ProOm AherNo ratings yet
- 1978 - 90 Day Study or Rhesus Monkey ToxicityDocument4 pages1978 - 90 Day Study or Rhesus Monkey Toxicitygrace poudrierNo ratings yet
- Early Years and Childcare Safeguarding AuditDocument4 pagesEarly Years and Childcare Safeguarding AuditEarly Years Careers100% (1)