You might also like
- Pmed 1002595 s003Document2 pagesPmed 1002595 s003Oneng IfayaniNo ratings yet
- Biostatistics: Descriptive Analysis and Differences Between GroupsDocument17 pagesBiostatistics: Descriptive Analysis and Differences Between GroupsOneng IfayaniNo ratings yet
- Intervention Type Quality AssessmentDocument5 pagesIntervention Type Quality AssessmentOneng IfayaniNo ratings yet
- PRISMA 2009 Checklist: Section/topic # Checklist Item Reported On Page #Document3 pagesPRISMA 2009 Checklist: Section/topic # Checklist Item Reported On Page #Oneng IfayaniNo ratings yet
- Biostatistics 1Document20 pagesBiostatistics 1Oneng IfayaniNo ratings yet
- Sample Size Required Per Group When Using The T Test To Compare Means of Continuous VariablesDocument11 pagesSample Size Required Per Group When Using The T Test To Compare Means of Continuous VariablesOneng IfayaniNo ratings yet
- Chapter 14Document15 pagesChapter 14Oneng IfayaniNo ratings yet
- Adverse Drug Reactions: Type C - Continuous Reactions Due To Long-Term Drug UseDocument9 pagesAdverse Drug Reactions: Type C - Continuous Reactions Due To Long-Term Drug UseOneng IfayaniNo ratings yet
- Chapter 8Document30 pagesChapter 8Oneng IfayaniNo ratings yet
- Chapter 9Document23 pagesChapter 9Oneng IfayaniNo ratings yet
- Chapter 4Document11 pagesChapter 4Oneng IfayaniNo ratings yet
- Conceiving The Research Question and Developing The Study PlanDocument9 pagesConceiving The Research Question and Developing The Study PlanOneng IfayaniNo ratings yet
- Chapter 1Document12 pagesChapter 1Oneng IfayaniNo ratings yet
- Quality of Antimikrobial - En.idDocument4 pagesQuality of Antimikrobial - En.idOneng IfayaniNo ratings yet
- Vandergarde Thorax2006Document5 pagesVandergarde Thorax2006Oneng IfayaniNo ratings yet
- Applied Statistics Survival AnalysisDocument23 pagesApplied Statistics Survival AnalysisOneng IfayaniNo ratings yet
- Statistik Deskriptif - SDA 2Document30 pagesStatistik Deskriptif - SDA 2Oneng IfayaniNo ratings yet
- Biochemistry and Cell Biology of Dopaminergic NeurotransmissionDocument18 pagesBiochemistry and Cell Biology of Dopaminergic NeurotransmissionOneng IfayaniNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- SERENACE Injection: What Is in This LeafletDocument5 pagesSERENACE Injection: What Is in This LeafletningrumNo ratings yet
- Electroconvulsive Therapy: Aban, Katherine Maebelle G. Esguerra, Dianne Carmela RDocument46 pagesElectroconvulsive Therapy: Aban, Katherine Maebelle G. Esguerra, Dianne Carmela REdgar ManoodNo ratings yet
- Biology 2 JournalDocument5 pagesBiology 2 JournalKadymars JaboneroNo ratings yet
- Cabaran Membesarkan Anak-Anak Autisme Daripada Perspektif Ibu (The Challenges of Nurturing Autistic Children From The Mother's Perspective) PDFDocument15 pagesCabaran Membesarkan Anak-Anak Autisme Daripada Perspektif Ibu (The Challenges of Nurturing Autistic Children From The Mother's Perspective) PDFsalwani salmizanNo ratings yet
- Soal Ujian PsikiatriDocument22 pagesSoal Ujian PsikiatriArya Ganesha100% (1)
- W6L28Document16 pagesW6L28N SinghNo ratings yet
- Klinefelter SyndromeDocument15 pagesKlinefelter SyndromeصادقNo ratings yet
- What Is Dissociative Identity DisorderDocument3 pagesWhat Is Dissociative Identity DisorderShifaDhinaNo ratings yet
- Manajemen Nyeri Neuropati Pada Pasien Diabetes Melitus Tipe 2: Studi LiteraturDocument7 pagesManajemen Nyeri Neuropati Pada Pasien Diabetes Melitus Tipe 2: Studi LiteraturEka NursafitriNo ratings yet
- 96-Article Text-328-1-10-20211022Document7 pages96-Article Text-328-1-10-20211022Asaad AlnhayerNo ratings yet
- GBS MCQDocument6 pagesGBS MCQMoonNo ratings yet
- Brief Psychotic Disorder Case PresDocument43 pagesBrief Psychotic Disorder Case PresTheressa TironaNo ratings yet
- DSM 5 Vs DSM 4 Case StudiesDocument18 pagesDSM 5 Vs DSM 4 Case Studiesapi-261267976100% (1)
- H.6 Internet Addiction PowerPoint 2015Document23 pagesH.6 Internet Addiction PowerPoint 2015Khoi NguyenNo ratings yet
- Psychiatry Summaries PDFDocument30 pagesPsychiatry Summaries PDFBEATRICE SOPHIA PARMANo ratings yet
- 14 OT Pediatrics AOTA Exam Prep.130Document51 pages14 OT Pediatrics AOTA Exam Prep.130Jarred Adams100% (1)
- Neuro Dr. RehabDocument142 pagesNeuro Dr. RehabMohammed Saad NabhanNo ratings yet
- Adhd BrochureDocument2 pagesAdhd BrochureJohanna MaraNo ratings yet
- Powerpoint On HemophiliaDocument26 pagesPowerpoint On HemophiliaTheo Sanson100% (1)
- Dissociation and Trauma: in Young PeopleDocument4 pagesDissociation and Trauma: in Young Peopleyeney armenterosNo ratings yet
- Emergency Care Emt 13th Edition Ebook PDFDocument61 pagesEmergency Care Emt 13th Edition Ebook PDFadolfo.milliken17896% (49)
- Solwezi General Mental Health TeamDocument35 pagesSolwezi General Mental Health TeamHumphreyNo ratings yet
- Cognitive Therapy: Past, Present, and Future: Aaron T. BeckDocument5 pagesCognitive Therapy: Past, Present, and Future: Aaron T. BeckLuisa LageNo ratings yet
- Scid2 BPDDocument4 pagesScid2 BPDRamonaStereaNo ratings yet
- A Beautiful MIND"": Movie AnalysisDocument8 pagesA Beautiful MIND"": Movie AnalysisRonita Nuqui0% (1)
- Phtls 9th Edition Prep Packets 2019aDocument19 pagesPhtls 9th Edition Prep Packets 2019ajuan4401100% (2)
- Management of Cerebral Palsy: A Literature Review From A Physiatric PerspectiveDocument4 pagesManagement of Cerebral Palsy: A Literature Review From A Physiatric Perspectivefebry firmansyahNo ratings yet
- Abnormally High Heart RateDocument2 pagesAbnormally High Heart RateEinah EinahNo ratings yet
- The Dangers of Binge EatingDocument2 pagesThe Dangers of Binge EatingJulio AlvesNo ratings yet
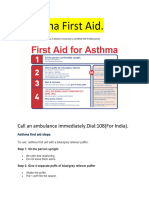
- Asthama First Aid.Document3 pagesAsthama First Aid.Manoj KumarNo ratings yet