You might also like
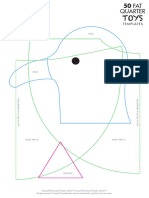
- 50 Fat Quarter Toys - TemplatesDocument42 pages50 Fat Quarter Toys - TemplateskatiaNo ratings yet
- Tilda Hot Chocolate Sewing TemplatesDocument18 pagesTilda Hot Chocolate Sewing TemplateskatiaNo ratings yet
- Sew ActivewearDocument96 pagesSew ActivewearkatiaNo ratings yet
- Create A Permaculture Fruit Tree GuildDocument3 pagesCreate A Permaculture Fruit Tree GuildkatiaNo ratings yet
- Accessing Your 'Strawman' Account - Filing A UCC1 Financing Statement - Stillness in The StormDocument4 pagesAccessing Your 'Strawman' Account - Filing A UCC1 Financing Statement - Stillness in The StormkatiaNo ratings yet
- Lemon Tree GuildDocument1 pageLemon Tree GuildkatiaNo ratings yet
- A Method To Obtain An Allodial Title To Your PropertyDocument2 pagesA Method To Obtain An Allodial Title To Your Propertykatia100% (1)
- Land Patent FAQ, Part 2 - How To File A Land PatentDocument11 pagesLand Patent FAQ, Part 2 - How To File A Land PatentkatiaNo ratings yet
- Sustainable Urban Composting: Determining Best Practices For Organic Waste Management in Burlington, VermontDocument160 pagesSustainable Urban Composting: Determining Best Practices For Organic Waste Management in Burlington, VermontkatiaNo ratings yet
- Application - Pineal FoundationDocument4 pagesApplication - Pineal FoundationkatiaNo ratings yet
- Biodynamic AgricultureDocument5 pagesBiodynamic AgriculturekatiaNo ratings yet
- BDW AffidavitDocument82 pagesBDW AffidavitkatiaNo ratings yet
- Big Bang Diagram DebunkedDocument11 pagesBig Bang Diagram DebunkedkatiaNo ratings yet
- Vaccine Protect 6-30Document4 pagesVaccine Protect 6-30katiaNo ratings yet
- The Nine Supplements Everyone Should TakeDocument4 pagesThe Nine Supplements Everyone Should TakekatiaNo ratings yet
- Summary of The Spike Protein ProtocolDocument4 pagesSummary of The Spike Protein ProtocolkatiaNo ratings yet
- PINE TEA - Possible Antidote For Spike Protein Transmission - Rights and FreedomsDocument4 pagesPINE TEA - Possible Antidote For Spike Protein Transmission - Rights and FreedomskatiaNo ratings yet
- Is Pine Needle Tea The Answer To Covid Vaccine Shedding - Transmission - Learn About Suramin, Shikimic Acid and How To Make Your Own ExtractsDocument7 pagesIs Pine Needle Tea The Answer To Covid Vaccine Shedding - Transmission - Learn About Suramin, Shikimic Acid and How To Make Your Own Extractskatia100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Basic Guide To Proposal Writing: Step 1: Developing Your Proposal IdeaDocument11 pagesBasic Guide To Proposal Writing: Step 1: Developing Your Proposal Ideanisaralamjan8616100% (2)
- Daftar PustakaDocument5 pagesDaftar PustakaR Handi BramantoNo ratings yet
- Communication and Nutrional EducationDocument11 pagesCommunication and Nutrional EducationSabrina PanjaitanNo ratings yet
- Jibachha's Handook of Animal HusbandryDocument40 pagesJibachha's Handook of Animal HusbandryJibachha ShahNo ratings yet
- Gouty GCPDocument48 pagesGouty GCPKylie GolindangNo ratings yet
- Department of Pharmaceutical ChemistryDocument13 pagesDepartment of Pharmaceutical ChemistrySuvarna KiniNo ratings yet
- Contractor Safety Rules PDFDocument10 pagesContractor Safety Rules PDFKEERTHI INDUSTRIESNo ratings yet
- Pbs Register of SponsorsDocument1,727 pagesPbs Register of SponsorsZaili KastamNo ratings yet
- 675 MSDSDocument4 pages675 MSDSAhmed Emad AhmedNo ratings yet
- TDS Shell Gadus S2 V220 2Document2 pagesTDS Shell Gadus S2 V220 2regisNo ratings yet
- MD 07Document109 pagesMD 07Lakshmi SethNo ratings yet
- Formal Special Areas: Border Management Red Corridor PncpcaDocument29 pagesFormal Special Areas: Border Management Red Corridor PncpcaAnirban MandalNo ratings yet
- Understanding The Psycho-Social and Health Problems Faced by Homeless Population in Visakhapatnam CityDocument8 pagesUnderstanding The Psycho-Social and Health Problems Faced by Homeless Population in Visakhapatnam CityMutluri AbrahamNo ratings yet
- Arntz 1999 Childhood Imagery Rescripting Paper PDFDocument26 pagesArntz 1999 Childhood Imagery Rescripting Paper PDFelliotNo ratings yet
- 1P1 - Anna Kusumawati 323-329Document7 pages1P1 - Anna Kusumawati 323-329imam habibiNo ratings yet
- Apa Research Paper On Eating DisordersDocument7 pagesApa Research Paper On Eating Disordersuifjzvrif100% (1)
- Notification No.19151 - Revised Guidelines MUKTADocument22 pagesNotification No.19151 - Revised Guidelines MUKTADeepak PeraNo ratings yet
- Purpose of Travel - SampleDocument3 pagesPurpose of Travel - SampleVirat GadhviNo ratings yet
- Vet Obst Lecture 2 Placenta Formation and GrowthDocument46 pagesVet Obst Lecture 2 Placenta Formation and GrowthgnpobsNo ratings yet
- Reflection Paper MULANAYDocument2 pagesReflection Paper MULANAYRob40% (5)
- Vha Class III ListingDocument2,575 pagesVha Class III ListingpvenkyNo ratings yet
- Water Intoxication - Is It Possible To Drink Too Much Water???Document11 pagesWater Intoxication - Is It Possible To Drink Too Much Water???NoraNo ratings yet
- Akapulko (Cassia Alata) Indication/s: Duration: Nursing ResponsibilitiesDocument16 pagesAkapulko (Cassia Alata) Indication/s: Duration: Nursing ResponsibilitiesEljay Lustria ReyesNo ratings yet
- Environmental Controls in Operating Theatres: S. Dharan and D. PittetDocument6 pagesEnvironmental Controls in Operating Theatres: S. Dharan and D. PittetDinda FSNo ratings yet
- Doctors List Bhopal PDFDocument4 pagesDoctors List Bhopal PDFMukesh NangiaNo ratings yet
- TGI0221 FinalDocument81 pagesTGI0221 FinalInes NarcisoNo ratings yet
- Ralph E. Strobel: Professional SummaryDocument3 pagesRalph E. Strobel: Professional Summaryapi-354918865No ratings yet
- Externalities & Public GoodsDocument13 pagesExternalities & Public GoodsAkshay ModakNo ratings yet
- Simple Magazine #17Document5 pagesSimple Magazine #17tôn thất minh khangNo ratings yet
- Traffic Signs ManualDocument334 pagesTraffic Signs Manualiwansalma100% (1)