You might also like
- Occupational Diseases and Health Awareness Through Multimedia: A Case Study Among Women at Risk Employed in Coir Retting in Kerala, IndiaFrom EverandOccupational Diseases and Health Awareness Through Multimedia: A Case Study Among Women at Risk Employed in Coir Retting in Kerala, IndiaNo ratings yet
- Community DiagnosisDocument28 pagesCommunity DiagnosisKarLo Tabuzo100% (2)
- Tugas Individu Kep KomunitasDocument10 pagesTugas Individu Kep KomunitasMeilissaNo ratings yet
- Used CHN Week 1Document37 pagesUsed CHN Week 1John paolo TiglaoNo ratings yet
- National Rural Health Mission analyzedDocument4 pagesNational Rural Health Mission analyzedANIRUDHNo ratings yet
- The Problem I. Background of The StudyDocument5 pagesThe Problem I. Background of The StudyWayne LambinoNo ratings yet
- Final Community Diagnosis of Tigbi Tiwi AlbayDocument50 pagesFinal Community Diagnosis of Tigbi Tiwi AlbayEduard Espeso Chiong-Gandul Jr.100% (4)
- Exploring Strategies To Improve The Performance of Community Health Volunteers For Tuberculosis Care and Prevention: A Qualitative StudyDocument8 pagesExploring Strategies To Improve The Performance of Community Health Volunteers For Tuberculosis Care and Prevention: A Qualitative StudyTIENDUONGNo ratings yet
- Socail Mobilzation Plan Final New 2Document15 pagesSocail Mobilzation Plan Final New 2Sajad Ahmed MemonNo ratings yet
- Capstone Proposal Tanauan GroupDocument9 pagesCapstone Proposal Tanauan GroupburdeosmaelnoraNo ratings yet
- Bottom Up' Approach: A Community-Based Intervention inDocument9 pagesBottom Up' Approach: A Community-Based Intervention inondikijames88No ratings yet
- Level of Awareness Towards Dengue Among The Residents of Barangay KauswaganDocument5 pagesLevel of Awareness Towards Dengue Among The Residents of Barangay KauswaganMercia Quinsayas Trabuco100% (1)
- The Unavailibility of Sufficient Public Healthcare in Our SocietyDocument5 pagesThe Unavailibility of Sufficient Public Healthcare in Our Societysoham chatterjeeNo ratings yet
- Study of Health Seeking Behavior and Its Determinants Among Attendees of Urban Health Center, Dharavi, Mumbai, IndiaDocument6 pagesStudy of Health Seeking Behavior and Its Determinants Among Attendees of Urban Health Center, Dharavi, Mumbai, IndiaIshwarya RaghuNo ratings yet
- Chapter I (A Case Study in Community and Public Health Area: Barangay Kayquit Iii, Purok 3 & 4)Document3 pagesChapter I (A Case Study in Community and Public Health Area: Barangay Kayquit Iii, Purok 3 & 4)sophiasaphire100% (1)
- Improving Public Health in a Cavite CommunityDocument3 pagesImproving Public Health in a Cavite CommunitysophiasaphireNo ratings yet
- Community Health Analysis of Brgy. 628Document79 pagesCommunity Health Analysis of Brgy. 628YongNo ratings yet
- Reflections of A Public Health AdvocateDocument9 pagesReflections of A Public Health AdvocateMichele YiNo ratings yet
- Pie GraphsDocument26 pagesPie GraphsDENNROSE DECLARONo ratings yet
- Case Study Community Problem and Solution AbilayDocument8 pagesCase Study Community Problem and Solution AbilayMark Laurence C. AbilayNo ratings yet
- Rural-Urban Comparison On Mothers' Media Access and Information Needs On Dengue Prevention and ControlDocument83 pagesRural-Urban Comparison On Mothers' Media Access and Information Needs On Dengue Prevention and ControlBuen Josef Cainila AndradeNo ratings yet
- Research in Community Health NursingDocument4 pagesResearch in Community Health NursingToday ViralNo ratings yet
- The Interrelations Between Community Development and Availability of Health Services in Barangay DalahicanDocument14 pagesThe Interrelations Between Community Development and Availability of Health Services in Barangay DalahicanPaul Julius M. Regio100% (1)
- Perceived Helping Skills of Community Health Workers in Selected Barangays of San Pascual Batangas Towards Enhancement of Community Health ServicesDocument68 pagesPerceived Helping Skills of Community Health Workers in Selected Barangays of San Pascual Batangas Towards Enhancement of Community Health ServicesChristian PerryNo ratings yet
- CHN MergedDocument261 pagesCHN MergedRej h100% (1)
- NP2 RationaleDocument19 pagesNP2 RationaleElizabella Henrietta TanaquilNo ratings yet
- A Study of Educational Status of Rural ChildrenDocument39 pagesA Study of Educational Status of Rural ChildrenAttaur RahamanNo ratings yet
- Community Health Nursing Ii NUR204: Population Groups and Community As Clients)Document31 pagesCommunity Health Nursing Ii NUR204: Population Groups and Community As Clients)ZairaNo ratings yet
- Jurnal BupiiiDocument7 pagesJurnal BupiiiIrma FatimahNo ratings yet
- CDC 7598 DS1Document72 pagesCDC 7598 DS1Umm e ArbabNo ratings yet
- ComMed-Logbook TcsDocument143 pagesComMed-Logbook TcsTeEbhan ChAnthira SeEkaranNo ratings yet
- Community Health NursingDocument10 pagesCommunity Health NursingBunzay GelineNo ratings yet
- Community Diagnosis FinalDocument116 pagesCommunity Diagnosis FinalAriane Ballaret75% (8)
- RNpedia WPS OfficeDocument12 pagesRNpedia WPS Officeguinomtadmarcos0No ratings yet
- Community Diagnosis FPT - Chapter 1Document19 pagesCommunity Diagnosis FPT - Chapter 1Katherine 'Chingboo' Leonico Laud100% (1)
- LugobaDocument8 pagesLugobagabrielNo ratings yet
- Community DiagnosisDocument38 pagesCommunity Diagnosisraquel93% (60)
- Ijerph 18 09661Document15 pagesIjerph 18 09661emmanuel emekaNo ratings yet
- COMMUNITY HEALTH ASSESSMENT AND DIAGNOSISDocument6 pagesCOMMUNITY HEALTH ASSESSMENT AND DIAGNOSISCAÑADA, JOHANNELYN M.No ratings yet
- Oleh: Riswan Hamid Siregar (20030038) Sri Indah Komala POHAN (20030004) Vinny Padilla Indriyani Siregar (20030016)Document10 pagesOleh: Riswan Hamid Siregar (20030038) Sri Indah Komala POHAN (20030004) Vinny Padilla Indriyani Siregar (20030016)Vinny PadillahNo ratings yet
- Healthy Spaces and Places.Document11 pagesHealthy Spaces and Places.Marvin CJNo ratings yet
- Lecture 42: New Issues Before The Sociologists Slide 1Document18 pagesLecture 42: New Issues Before The Sociologists Slide 1Jaf ShahNo ratings yet
- Sociology ResearchDocument19 pagesSociology Researchbbddbbd2003No ratings yet
- ConceptOfCommunity&PhilHealthSituation Module CHN2 Jan2021Document18 pagesConceptOfCommunity&PhilHealthSituation Module CHN2 Jan2021Denise CastroNo ratings yet
- The Role of Social MediaDocument11 pagesThe Role of Social MediaJosé MartínezNo ratings yet
- Chapters 1 To 2. Incomplete. Please Double CheckDocument19 pagesChapters 1 To 2. Incomplete. Please Double CheckajdgafjsdgaNo ratings yet
- The Public/Community Health Nursing ProcessDocument79 pagesThe Public/Community Health Nursing ProcessRitaNo ratings yet
- Primary Health Care As An Approach To HealthDocument31 pagesPrimary Health Care As An Approach To HealthRea Andrea CuaresmaNo ratings yet
- Community DiagnosisDocument30 pagesCommunity DiagnosisPaulo Galang83% (6)
- Cmmty DXDocument125 pagesCmmty DXReine Chiara B. ConchaNo ratings yet
- CHN2 Lecture Number 2 PDFDocument31 pagesCHN2 Lecture Number 2 PDFJulian SantosNo ratings yet
- Community perceptions of solid waste management in DhakaDocument1 pageCommunity perceptions of solid waste management in DhakaUjjwal anandNo ratings yet
- Foundations - 1 (Part 1)Document54 pagesFoundations - 1 (Part 1)Minatulahamida Al-fitra KadayunanNo ratings yet
- Community Health Nursing 1: (Individual and Family As Clients)Document63 pagesCommunity Health Nursing 1: (Individual and Family As Clients)Wilma Nierva Beralde100% (4)
- Acquaintance With The Actuality: Community Diagnosis Programme of Kathmandu Medical College at Gundu Village, Bhaktapur, NepalDocument7 pagesAcquaintance With The Actuality: Community Diagnosis Programme of Kathmandu Medical College at Gundu Village, Bhaktapur, Nepalputriaisyahn ainiNo ratings yet
- Sample Community DiagnosisDocument37 pagesSample Community DiagnosisKarLo Tabuzo50% (2)
- CHN 30 ItemsDocument4 pagesCHN 30 Itemsdhma.gacutan.uiNo ratings yet
- Assignment: QuestionsDocument5 pagesAssignment: QuestionsDanna Mae CachoNo ratings yet
- Primary Health CareDocument41 pagesPrimary Health CareKailash NagarNo ratings yet
- TQM Study of University Libraries in Tamil NaduDocument131 pagesTQM Study of University Libraries in Tamil NaduPalak ChughNo ratings yet
- MS - 100 Synopsis HRDocument15 pagesMS - 100 Synopsis HRPalak ChughNo ratings yet
- Old NCERT Books PDF Political Science Class XII Democracy in India Issues and Challenges - WWW - Dhyeyaias.com - PDFDocument285 pagesOld NCERT Books PDF Political Science Class XII Democracy in India Issues and Challenges - WWW - Dhyeyaias.com - PDFHimanshu JaiswalNo ratings yet
- Mani SynopsDocument27 pagesMani SynopsPalak ChughNo ratings yet
- Mesp 85 SynopsisDocument27 pagesMesp 85 SynopsisPalak ChughNo ratings yet
- 570-ULSP status index instrument cablesDocument184 pages570-ULSP status index instrument cableskumarnpccNo ratings yet
- Filter Integrity Test MachineDocument4 pagesFilter Integrity Test MachineAtul SharmaNo ratings yet
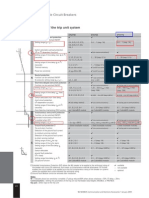
- ETU 776 TripDocument1 pageETU 776 TripbhaskarinvuNo ratings yet
- TL102 0 2024 Che3701 0Document12 pagesTL102 0 2024 Che3701 0sollomontlou06No ratings yet
- PDFDocument478 pagesPDFPriyaranjan PradhanNo ratings yet
- English Task "Analytical Exposition": Smoking BansDocument7 pagesEnglish Task "Analytical Exposition": Smoking BansFirda RazaqNo ratings yet
- Self-Confidence and Satisfaction Among Nursing Students With The Use of High Fidelity Simulation at Arab American University, PalestineDocument10 pagesSelf-Confidence and Satisfaction Among Nursing Students With The Use of High Fidelity Simulation at Arab American University, PalestineArianna Jasmine MabungaNo ratings yet
- Harman/kardon: Onyx Studio 3Document36 pagesHarman/kardon: Onyx Studio 3Thai Lam100% (1)
- SX SeriesDocument6 pagesSX SeriesmattuttezNo ratings yet
- WaterDocument2 pagesWaterLogan Marquez AguayoNo ratings yet
- Articol Final Rev MG-MK LB Engleza - Clinica Virtuala OnlineDocument14 pagesArticol Final Rev MG-MK LB Engleza - Clinica Virtuala Onlineadina1971No ratings yet
- Quality Operating Process: Manual of Operations Care of PatientsDocument4 pagesQuality Operating Process: Manual of Operations Care of PatientsPrabhat KumarNo ratings yet
- Banking Question PapersDocument12 pagesBanking Question Papersmohak khinNo ratings yet
- Divine Intervention Episode 5 Cardio A Physiology1Document18 pagesDivine Intervention Episode 5 Cardio A Physiology1Swisskelly1No ratings yet
- TBT Accident Prevention 1Document2 pagesTBT Accident Prevention 1zaimNo ratings yet
- KR1100 2Document1 pageKR1100 2Byron Xavier Lima CedilloNo ratings yet
- Klee N Rite 50100Document24 pagesKlee N Rite 50100Nestor Marquez-DiazNo ratings yet
- "Channel Sampling": Forms & ChecklistDocument1 page"Channel Sampling": Forms & ChecklistevonNo ratings yet
- SGS-GIS-RFC - Combined Version-A4 - v8 - Mar 16 2018Document3 pagesSGS-GIS-RFC - Combined Version-A4 - v8 - Mar 16 2018Refresh CornerNo ratings yet
- Wisdom Chi KungDocument0 pagesWisdom Chi KungDevlinPyxNo ratings yet
- Common Admission Test (CAT) 2020 Admit Card: BarcodeDocument2 pagesCommon Admission Test (CAT) 2020 Admit Card: BarcodeViraaj ThakurNo ratings yet
- Axell Wireless Cellular Coverage Solutions BrochureDocument8 pagesAxell Wireless Cellular Coverage Solutions BrochureBikash ShakyaNo ratings yet
- CHAP2 Bioavailability of Metals David Jhon LeventhalDocument9 pagesCHAP2 Bioavailability of Metals David Jhon LeventhalCrisThian PaucaNo ratings yet
- FHJJDocument8 pagesFHJJCristina MocanuNo ratings yet
- Drugs MnemonicsDocument6 pagesDrugs MnemonicsDarrylJavier100% (1)
- Neisseria and HaemophilusDocument15 pagesNeisseria and HaemophilusEdwin CvNo ratings yet
- SITHPAT006 Student LogbookDocument46 pagesSITHPAT006 Student LogbookÇrox Rmg PunkNo ratings yet
- The "Break-Even" Ang Bao Rates For Wedding in 2019 Wedding Ang Bao Rates in SingaporeDocument1 pageThe "Break-Even" Ang Bao Rates For Wedding in 2019 Wedding Ang Bao Rates in SingaporeNicholas TanNo ratings yet
- Pedest Tbox Toolbox - 4 Sidewalks and Walkways PDFDocument44 pagesPedest Tbox Toolbox - 4 Sidewalks and Walkways PDFbagibagifileNo ratings yet
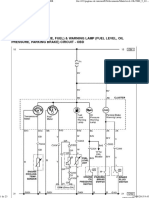
- Dokumen - Tips Daewoo Service Manual Instrument Cluster Matiz-2023Document23 pagesDokumen - Tips Daewoo Service Manual Instrument Cluster Matiz-2023urexalg AlgériaNo ratings yet