You might also like
- COVID-19 LEGACY: SARS-CoV-2 clinical trials, vaccines trials and bioethicsFrom EverandCOVID-19 LEGACY: SARS-CoV-2 clinical trials, vaccines trials and bioethicsNo ratings yet
- Lung Explant With Sars Cov 2Document10 pagesLung Explant With Sars Cov 2Ping LiuNo ratings yet
- SARS-CoV-2 Host Diversity - An Update of Natural Infections and Experimental EvidenceDocument11 pagesSARS-CoV-2 Host Diversity - An Update of Natural Infections and Experimental EvidenceruiNo ratings yet
- Kinetics of Specific IgM and IgG Responses PatientsDocument9 pagesKinetics of Specific IgM and IgG Responses Patientsluohucy163.comNo ratings yet
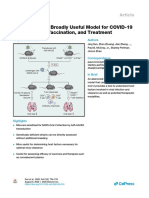
- Generation of A Broadly Useful Model For COVID19 Pathogenesis Vaccination and TreatmentDocument16 pagesGeneration of A Broadly Useful Model For COVID19 Pathogenesis Vaccination and Treatmentgaurav sharmaNo ratings yet
- Pathogenesis and Transmission of SARS-CoV-2 in Golden Syrian HamstersDocument18 pagesPathogenesis and Transmission of SARS-CoV-2 in Golden Syrian HamstersDakota1955aaNo ratings yet
- Ajplung 00223 2021Document8 pagesAjplung 00223 2021wn6ejrNo ratings yet
- Ad26.Cov2.S Prevents Sars-Cov-2 Induced Pathways of Inflammation and Thrombosis in HamstersDocument46 pagesAd26.Cov2.S Prevents Sars-Cov-2 Induced Pathways of Inflammation and Thrombosis in Hamsterscristianismo sem MáscaraNo ratings yet
- Attenuated Interferon and Proinflammatory Response in SARS-CoV-2-Infected Human Dendritic Cells Is Associated With Viral Antagonism of STAT1 PhosphorylationDocument12 pagesAttenuated Interferon and Proinflammatory Response in SARS-CoV-2-Infected Human Dendritic Cells Is Associated With Viral Antagonism of STAT1 PhosphorylationGeovane MarquesNo ratings yet
- Covid y Sistema EndocrinoDocument22 pagesCovid y Sistema EndocrinocristinaNo ratings yet
- Sambiloto Sarscov2Document10 pagesSambiloto Sarscov2Salman FaridziNo ratings yet
- COVID-19 Fact Sheet ENG PDFDocument27 pagesCOVID-19 Fact Sheet ENG PDFLuis Ricardo Soto JimenezNo ratings yet
- Article-2020-Genomic Diversity of SARS-CoV-2 in Coronavirus Disease 2019 PatientsDocument27 pagesArticle-2020-Genomic Diversity of SARS-CoV-2 in Coronavirus Disease 2019 Patientscarlos ArozamenaNo ratings yet
- Sars Cov2 Antigen Presentation Process by Immune Cells: Immunology Assignment - 2Document17 pagesSars Cov2 Antigen Presentation Process by Immune Cells: Immunology Assignment - 2azeema fatimaNo ratings yet
- Viruses 12 00404 PDFDocument14 pagesViruses 12 00404 PDFShriya MehtaNo ratings yet
- Knowing When and How To Fight: COVID-19 Between Viral Clearance and Immune ToleranceDocument11 pagesKnowing When and How To Fight: COVID-19 Between Viral Clearance and Immune ToleranceAri Trianto WibowoNo ratings yet
- Factors Affecting SARS CoV 2 (COVID-19) PandemicDocument32 pagesFactors Affecting SARS CoV 2 (COVID-19) PandemicTahir AliNo ratings yet
- Diarrhea During COVID-19 InfectionDocument11 pagesDiarrhea During COVID-19 InfectionMan'SzAr'diAnSyAhNo ratings yet
- New ChallengeDocument3 pagesNew ChallengeEliana TorresNo ratings yet
- Clinical Immunology: Susanna Felsenstein, Jenny A. Herbert, Paul S. Mcnamara, Christian M. Hedrich TDocument13 pagesClinical Immunology: Susanna Felsenstein, Jenny A. Herbert, Paul S. Mcnamara, Christian M. Hedrich TIrma NeyraNo ratings yet
- Potential Antigenic Cross-Reactivity Between SARS-CoV-2 and Dengue VirusesDocument19 pagesPotential Antigenic Cross-Reactivity Between SARS-CoV-2 and Dengue ViruseseveNo ratings yet
- Potential Role of Oral Rinses Targeting The Viral Lipid Zqaa002 COMPLETODocument12 pagesPotential Role of Oral Rinses Targeting The Viral Lipid Zqaa002 COMPLETODallas Juan Tarco SumireNo ratings yet
- Immune Responses in COVID-19 and Potential Vaccines: Lessons Learned From SARS and MERS EpidemicDocument9 pagesImmune Responses in COVID-19 and Potential Vaccines: Lessons Learned From SARS and MERS EpidemicJC XDNo ratings yet
- Narrative Reviews: Diarrhea During COVID-19 Infection: Pathogenesis, Epidemiology, Prevention, and ManagementDocument10 pagesNarrative Reviews: Diarrhea During COVID-19 Infection: Pathogenesis, Epidemiology, Prevention, and ManagementWaqasKhanNo ratings yet
- COVID-19 Fact Sheet ENGDocument38 pagesCOVID-19 Fact Sheet ENGIl Principio CarinoNo ratings yet
- Characterization of Anti-Viral Immunity in Recovered Individuals Infected by Sars-Cov-2Document14 pagesCharacterization of Anti-Viral Immunity in Recovered Individuals Infected by Sars-Cov-2ArtNo ratings yet
- Deciphering COVID-19 A ReviewDocument12 pagesDeciphering COVID-19 A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cei 202 162Document31 pagesCei 202 162chaterinaNo ratings yet
- Caractere VirologiaueDocument29 pagesCaractere Virologiauehind el hamriNo ratings yet
- COVID-19 Re-Infection by A Phylogenetically Distinct SARS-coronavirus-2 Strain Confirmed by Whole Genome SequencingDocument25 pagesCOVID-19 Re-Infection by A Phylogenetically Distinct SARS-coronavirus-2 Strain Confirmed by Whole Genome SequencingNano NoratoNo ratings yet
- 2020 Distinct Infection Process of SARS CoV 2 in Human Bronchial Epithelial Cell LinesDocument9 pages2020 Distinct Infection Process of SARS CoV 2 in Human Bronchial Epithelial Cell LinesMartin JYNo ratings yet
- Coronavirus3 PDFDocument28 pagesCoronavirus3 PDFWilmar David Medina MadridNo ratings yet
- COVID-19, Immune System Response, Hyperinflammation and Repurposing Antirheumatic DrugsDocument13 pagesCOVID-19, Immune System Response, Hyperinflammation and Repurposing Antirheumatic DrugsMarcelitaTaliaDuwiriNo ratings yet
- Réponse Immun Covid19Document8 pagesRéponse Immun Covid19Tidiane SibyNo ratings yet
- 1 Baldoni Zarycz MolSimulation 2022Document12 pages1 Baldoni Zarycz MolSimulation 2022Natalia ZaryczNo ratings yet
- COVID-19 Diagnosis  A Review of Current MethodsDocument16 pagesCOVID-19 Diagnosis  A Review of Current MethodsMariana BalderramaNo ratings yet
- Epid Pubmed 1 (Bab2) .En - IdDocument11 pagesEpid Pubmed 1 (Bab2) .En - IdSHAFIYA ADELINANo ratings yet
- Evaluation of An Antigen Detection Rapid Diagnostic Test For Detection of Sars-Cov-2 in Clinical SamplesDocument9 pagesEvaluation of An Antigen Detection Rapid Diagnostic Test For Detection of Sars-Cov-2 in Clinical Samplesjytj tjrj64fdNo ratings yet
- ACE2 Covid 2Document6 pagesACE2 Covid 2Laura Kristel Sánchez HernandezNo ratings yet
- The Modelling of COVID19 Pathways Sheds Light On Mechanisms, Opportunities and On Controversial Interpretations of Medical Treatments. v2Document15 pagesThe Modelling of COVID19 Pathways Sheds Light On Mechanisms, Opportunities and On Controversial Interpretations of Medical Treatments. v2ballechaseNo ratings yet
- The Yan ReportDocument27 pagesThe Yan ReportAndrea MartinezNo ratings yet
- Drug Sars-CovDocument20 pagesDrug Sars-CovSilvi Zakiyatul IlmiyahNo ratings yet
- PIIS0168827820336758Document17 pagesPIIS0168827820336758Yusup AhmadiNo ratings yet
- Articulo Cientifico Derrame Pleural en Covid 19Document10 pagesArticulo Cientifico Derrame Pleural en Covid 19Leyla Barnard LagunaNo ratings yet
- COVID-19 Fact Sheet ENGDocument32 pagesCOVID-19 Fact Sheet ENGjuancvlNo ratings yet
- BiomedPap - Bio 202003 0001Document9 pagesBiomedPap - Bio 202003 0001Edison Chiriboga OrtegaNo ratings yet
- 13 ACE2 Receptor For Covid19Document11 pages13 ACE2 Receptor For Covid19mmaNo ratings yet
- Journal Pre-Proof: Life SciencesDocument20 pagesJournal Pre-Proof: Life Sciences3323No ratings yet
- 5400-Article Text-31589-2-10-20210820Document12 pages5400-Article Text-31589-2-10-20210820Voltaire Méndez RodríguezNo ratings yet
- COVID-19 Compared To Other Pandemic DiseasesDocument17 pagesCOVID-19 Compared To Other Pandemic DiseasesDavid TorresNo ratings yet
- Immune Responses in COVID-19 and Potential Vaccines: Lessons Learned From SARS and MERS EpidemicDocument9 pagesImmune Responses in COVID-19 and Potential Vaccines: Lessons Learned From SARS and MERS EpidemicCucumber IsHealthy96No ratings yet
- Overview JournalDocument8 pagesOverview JournalDea Inthay WulanNo ratings yet
- Male Fertility and COVID 19 Pandemic 1606862102Document15 pagesMale Fertility and COVID 19 Pandemic 1606862102lauravellezNo ratings yet
- COVID - RNA Work PDFDocument5 pagesCOVID - RNA Work PDFomkarNo ratings yet
- The COVID TerjemahanDocument3 pagesThe COVID TerjemahanSusilawaty LestariNo ratings yet
- 001 Profiling Early Humoral Response To COVID-19 (IDSA 20) READDocument8 pages001 Profiling Early Humoral Response To COVID-19 (IDSA 20) READagboxNo ratings yet
- COVID-19 Immune System Response Hyperinflammation and RepurposiDocument14 pagesCOVID-19 Immune System Response Hyperinflammation and RepurposiLizbethNo ratings yet
- Sarscov2 Promote InflammationDocument13 pagesSarscov2 Promote InflammationAgnese ValentiniNo ratings yet
- s41423 021 00813 6Document12 pagess41423 021 00813 6Josué Cristhian Del Valle HornaNo ratings yet
- ExosomesinfectiousdiseaseDocument10 pagesExosomesinfectiousdiseaseTaniaNo ratings yet
- Exosomes in Viral Disease: ReviewDocument12 pagesExosomes in Viral Disease: ReviewTaniaNo ratings yet
- Viral Nucleic Acids in Live-Attenuated Vaccines: Detection of Minority Variants and An Adventitious VirusDocument8 pagesViral Nucleic Acids in Live-Attenuated Vaccines: Detection of Minority Variants and An Adventitious VirusTaniaNo ratings yet
- Exosomes RNADocument8 pagesExosomes RNATaniaNo ratings yet
- Perspective: Memory Engram Cells Have Come of AgeDocument14 pagesPerspective: Memory Engram Cells Have Come of AgeTaniaNo ratings yet
- Magnetic Sensing Through The Abdomen of The Honey BeeDocument7 pagesMagnetic Sensing Through The Abdomen of The Honey BeeTaniaNo ratings yet
- Apoptotic Cell-Derived Exosomes: Messages From Dying Cells: Reviewarticle OpenaccessDocument6 pagesApoptotic Cell-Derived Exosomes: Messages From Dying Cells: Reviewarticle OpenaccessTaniaNo ratings yet
- That Circumstances Exist Justifying Authorizations Pursuant To Section 564 (B) of The Federal Food, Drug, andDocument8 pagesThat Circumstances Exist Justifying Authorizations Pursuant To Section 564 (B) of The Federal Food, Drug, andTaniaNo ratings yet
- DR Will Cole Tips PDFDocument12 pagesDR Will Cole Tips PDFTania100% (4)
- Sentinel Visualizer 6 User GuideDocument227 pagesSentinel Visualizer 6 User GuideTaniaNo ratings yet
- Visual Diagnosis and Traditional Chinese Medicine: Face Reading - What Your Face SaysDocument8 pagesVisual Diagnosis and Traditional Chinese Medicine: Face Reading - What Your Face SaysTaniaNo ratings yet
- Anatomy and Physiology: Bone Histology Lecture OutlineDocument42 pagesAnatomy and Physiology: Bone Histology Lecture OutlineFokeerbux ZyadNo ratings yet
- Sickle Cell Case StudyDocument3 pagesSickle Cell Case StudyIsaac KipkemoiNo ratings yet
- G7 Science Q2 - Week 3-Levels of Biological OrganizationDocument48 pagesG7 Science Q2 - Week 3-Levels of Biological OrganizationJessa-Bhel AlmueteNo ratings yet
- Identify The Choice That Best Completes The Statement or Answers The QuestionDocument14 pagesIdentify The Choice That Best Completes The Statement or Answers The QuestionCamille BaybayNo ratings yet
- Human Circulatory SystemDocument3 pagesHuman Circulatory SystemMir Rehan Mushtaq100% (1)
- Birth Class 11Document5 pagesBirth Class 11anushkaparashar85No ratings yet
- Bones of The HindlimbDocument164 pagesBones of The HindlimbAdriana Anghel100% (1)
- Blood Pressure RegulationDocument35 pagesBlood Pressure Regulationبراءة أحمد السلاماتNo ratings yet
- GlossaryDocument63 pagesGlossaryavagavaNo ratings yet
- Lecture 1 HISTOLOGY OF THE RESPIRATORY SYSTEMDocument53 pagesLecture 1 HISTOLOGY OF THE RESPIRATORY SYSTEMlilimanao86% (7)
- 新New Metatron 4025 Hunter FeaturesDocument12 pages新New Metatron 4025 Hunter FeaturesTotal Acess100% (1)
- Module 9Document3 pagesModule 9Gia Joy B. PardeNo ratings yet
- Test Bank For Human Anatomy 6th Edition MartiniDocument24 pagesTest Bank For Human Anatomy 6th Edition MartiniBettyann Williams100% (40)
- Clear My Choice: Not Yet Answered Marked Out of 1.00Document7 pagesClear My Choice: Not Yet Answered Marked Out of 1.00medodiabNo ratings yet
- 11th STD - Class-4 (ZMP Sir) - Chemical Coordination and Integration - NotesDocument16 pages11th STD - Class-4 (ZMP Sir) - Chemical Coordination and Integration - Notesdisha shuklaNo ratings yet
- Developmental Biology Lecture Notes 4Document6 pagesDevelopmental Biology Lecture Notes 4Oguh AugustineNo ratings yet
- Nervous SystemDocument94 pagesNervous Systemmr pcNo ratings yet
- Techniques in Neuroanatomical ResearchDocument404 pagesTechniques in Neuroanatomical ResearchVlad TomaNo ratings yet
- Basosquamous Carcinoma: Treatment With Mohs Micrographic SurgeryDocument6 pagesBasosquamous Carcinoma: Treatment With Mohs Micrographic SurgeryMindaugas TNo ratings yet
- Nursing Care of The Child With A Hematologic Disorder TermsDocument8 pagesNursing Care of The Child With A Hematologic Disorder TermsJœnríčk AzueloNo ratings yet
- Correlacion Clinica Tej MuscularDocument5 pagesCorrelacion Clinica Tej MuscularEduardo SalazarNo ratings yet
- HistologyDocument65 pagesHistologyAlliana FlorenzaNo ratings yet
- ERBEJETDocument8 pagesERBEJETHossain TanjilaaNo ratings yet
- The Human Heart: Learner's Book Pg. # 8-9Document17 pagesThe Human Heart: Learner's Book Pg. # 8-9hareem FatimaNo ratings yet
- Prostate GlandsDocument3 pagesProstate GlandsDragan PetrovicNo ratings yet
- The Digestive System Notes - Grade 9Document3 pagesThe Digestive System Notes - Grade 9bd6cpynwmpNo ratings yet
- 04.06.2018 - 6 - V. Kushakovsky - Pediatric AnaesthesiaDocument46 pages04.06.2018 - 6 - V. Kushakovsky - Pediatric AnaesthesiaPhilippe KinnaerNo ratings yet
- Pricelist GD Metro PDFDocument45 pagesPricelist GD Metro PDFNovie NursantyNo ratings yet
- Sedimen UrinDocument73 pagesSedimen UrinHerbanu PramonoNo ratings yet
- 4 MyologyDocument57 pages4 MyologyAbhijith S. PNo ratings yet