You might also like
- Physiological Changes in Aging Affecting Various SystemsDocument30 pagesPhysiological Changes in Aging Affecting Various SystemsErven AranasNo ratings yet
- Week FiveDocument10 pagesWeek Fiveعـَــٻاس مَـــشتاقNo ratings yet
- Cooper C, Campion G, Melton LJ, 3rd. Hip Fractures in The Elderly: A World-Wide Projection. Osteoporosis Int. 1992 2 (6) :285-289Document5 pagesCooper C, Campion G, Melton LJ, 3rd. Hip Fractures in The Elderly: A World-Wide Projection. Osteoporosis Int. 1992 2 (6) :285-289Noor-E-Khadiza ShamaNo ratings yet
- Bone Remodeling and Osteoporosis ExplainedDocument11 pagesBone Remodeling and Osteoporosis ExplainedMesum JuttNo ratings yet
- Extract Sukhvendra Singh PDFDocument9 pagesExtract Sukhvendra Singh PDFMORDHWAJTOMARNo ratings yet
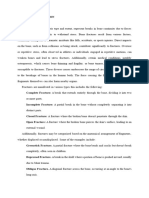
- Diseases and Disorders of The Skeletal SystemDocument11 pagesDiseases and Disorders of The Skeletal SystemJames Roy100% (1)
- Osteoporosis For BonesDocument24 pagesOsteoporosis For BonesRoking KumarNo ratings yet
- Musculoskeletal Management 1: School of Health & Social Care Division of PhysiotherapyDocument6 pagesMusculoskeletal Management 1: School of Health & Social Care Division of PhysiotherapyGeorge LuptonNo ratings yet
- FRACTURESDocument35 pagesFRACTURESMichelle DuNo ratings yet
- Essentials of Bone Densitometru For The Medical PhysicistDocument10 pagesEssentials of Bone Densitometru For The Medical PhysicistAmanda Farias FranciscoNo ratings yet
- Changes in the Musculoskeletal System during AgeingDocument19 pagesChanges in the Musculoskeletal System during Ageingsonali tushamerNo ratings yet
- ASKEP OsteoporosisDocument41 pagesASKEP OsteoporosisMaya PinteNo ratings yet
- Local Media6301021453740553391Document8 pagesLocal Media6301021453740553391ARAGON GEMMA LYNNo ratings yet
- The Normal Aging Process ExplainedDocument7 pagesThe Normal Aging Process ExplainedMonika JosephNo ratings yet
- MT16 QSU60104 M221 | MUSCLE AND BONE PROBLEMSDocument6 pagesMT16 QSU60104 M221 | MUSCLE AND BONE PROBLEMSFOONG YI KUAN MoeNo ratings yet
- Osteoporosis: How To Treat Osteoporosis: How To Prevent Osteoporosis: Along With Nutrition, Diet And Exercise For OsteoporosisFrom EverandOsteoporosis: How To Treat Osteoporosis: How To Prevent Osteoporosis: Along With Nutrition, Diet And Exercise For OsteoporosisNo ratings yet
- How Time Takes Its Toll: The Biological Effects of AgingDocument2 pagesHow Time Takes Its Toll: The Biological Effects of AgingYuri GagarinNo ratings yet
- Bone DiseaseDocument4 pagesBone DiseaseHuzaifa CHNo ratings yet
- Health and Wellness for SeniorsDocument43 pagesHealth and Wellness for Seniorsmelodyg40No ratings yet
- Biological and Cognitive Aspects of AgingDocument16 pagesBiological and Cognitive Aspects of AgingAmanda ScarletNo ratings yet
- Human CavitiesDocument14 pagesHuman CavitiesDrexel DalaygonNo ratings yet
- Osteoarthritis: Natural Drugless Treatments That Really Work!From EverandOsteoarthritis: Natural Drugless Treatments That Really Work!No ratings yet
- What Is Osteoarthritis?: ArthritisDocument4 pagesWhat Is Osteoarthritis?: ArthritisJohn Mark Alvin TorresNo ratings yet
- Apley OA 2Document11 pagesApley OA 2Koko AgungNo ratings yet
- Osteoarthritis: A Guide to the Common Joint DiseaseDocument34 pagesOsteoarthritis: A Guide to the Common Joint Diseasesamiul bashirNo ratings yet
- Musculoskeletal System - 14pDocument14 pagesMusculoskeletal System - 14pLinh LeNo ratings yet
- Westjmed00101 0065Document15 pagesWestjmed00101 0065zarrougonesNo ratings yet
- Physiology of AgingDocument45 pagesPhysiology of AgingLetyPerezTovarNo ratings yet
- Chapter 23: Osteoporosis of The SpineDocument15 pagesChapter 23: Osteoporosis of The SpineTraian UrsuNo ratings yet
- Muscular system-WPS OfficeDocument27 pagesMuscular system-WPS OfficeNiño Rey LavadorNo ratings yet
- Gerontology Reporting Group 1Document41 pagesGerontology Reporting Group 1Caryl Anne Dumdum CagaraNo ratings yet
- Osteoarthritis: An OverviewDocument24 pagesOsteoarthritis: An OverviewSulung Ade PratamaNo ratings yet
- Skeletal System: Univ. Ovidius Facultatea de Medicina Iosub Elena Iordache Cristina Sursa:WikipediaDocument26 pagesSkeletal System: Univ. Ovidius Facultatea de Medicina Iosub Elena Iordache Cristina Sursa:WikipediaCristian LuncasuNo ratings yet
- Skeletal system diseases and disordersDocument3 pagesSkeletal system diseases and disordersMbagwuMartinEzeugoNo ratings yet
- GUIA1255b1255d 1Document28 pagesGUIA1255b1255d 1CarlosRodríguezNo ratings yet
- Aging Changes in The BonesDocument5 pagesAging Changes in The Bonesrofana123No ratings yet
- Physiologicchangesofthe Musculoskeletalsystem Withaging:: A Brief ReviewDocument7 pagesPhysiologicchangesofthe Musculoskeletalsystem Withaging:: A Brief ReviewRizqan Fahlevvi AkbarNo ratings yet
- Osteoporosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandOsteoporosis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Mayo Clinic Guide to Preventing & Treating Osteoporosis: Keeping Your Bones Healthy and Strong to Reduce Your Risk of FractureFrom EverandMayo Clinic Guide to Preventing & Treating Osteoporosis: Keeping Your Bones Healthy and Strong to Reduce Your Risk of FractureRating: 2 out of 5 stars2/5 (1)
- Osteoporosis: Signs and SymptomsDocument9 pagesOsteoporosis: Signs and SymptomschelseachoirNo ratings yet
- Physical Changes Elderly Over 65Document2 pagesPhysical Changes Elderly Over 65Innocent-j CartagenaNo ratings yet
- Jawaban Perrtanyaan Tutor - Aging ProcessDocument7 pagesJawaban Perrtanyaan Tutor - Aging ProcessWinda PermatasariNo ratings yet
- Definisi OsteoporosisDocument3 pagesDefinisi OsteoporosisimissgnaNo ratings yet
- Older Adult Blueprint-Exam 1 SupplementDocument5 pagesOlder Adult Blueprint-Exam 1 SupplementNick BishopNo ratings yet
- OSTEOARTHRITISDocument61 pagesOSTEOARTHRITISARYAN THAPANo ratings yet
- Osteoarthritis Facts: ArthritisDocument2 pagesOsteoarthritis Facts: ArthritisparciNo ratings yet
- Final EbookDocument22 pagesFinal Ebookjinalgpatel11998No ratings yet
- Arthritis of the Wrist, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandArthritis of the Wrist, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- What Are Osteoporosis Symptoms and Signs?Document5 pagesWhat Are Osteoporosis Symptoms and Signs?Belle Mae SNo ratings yet
- Osteoporosis: Causes, Risks and PreventionDocument6 pagesOsteoporosis: Causes, Risks and PreventionKarla Mariana Gallegos P�rezNo ratings yet
- PPrevention Practice For Musculo Skeletal ConditionsDocument28 pagesPPrevention Practice For Musculo Skeletal ConditionsArham ShamsiNo ratings yet
- Osteoarthritis (Oa)Document19 pagesOsteoarthritis (Oa)Aj JaNo ratings yet
- Osteoarthiti1 in EngDocument3 pagesOsteoarthiti1 in EngVhyanVhyanNo ratings yet
- Ageing PhysiologyDocument37 pagesAgeing Physiologyeyob kaseyeNo ratings yet
- 2021 Sample Quantitative Chapters 1 and 2Document45 pages2021 Sample Quantitative Chapters 1 and 2Mark Jhuziel NacesNo ratings yet
- FNCP For Case Presentation COPARDocument3 pagesFNCP For Case Presentation COPARJann ericka JaoNo ratings yet
- Types of PCRDocument26 pagesTypes of PCRLydia EniithNo ratings yet
- FundamentalsExam W RatioDocument13 pagesFundamentalsExam W RatioJann ericka JaoNo ratings yet
- RESPI QuestionDocument14 pagesRESPI QuestionPrince Charles AbalosNo ratings yet
- Cultivating Excellence in Nursing Care for Pediatric AsthmaDocument5 pagesCultivating Excellence in Nursing Care for Pediatric AsthmaJann ericka JaoNo ratings yet
- Racial Disparities in Heart Disease Deaths and Risk FactorsDocument2 pagesRacial Disparities in Heart Disease Deaths and Risk FactorsJann ericka JaoNo ratings yet
- Mid-Term Aging Perspective DemographyDocument15 pagesMid-Term Aging Perspective DemographyJann ericka JaoNo ratings yet
- NCM 113 CHN 2 Lec SyllabusDocument24 pagesNCM 113 CHN 2 Lec SyllabusJann ericka Jao100% (3)
- Easy ECG GuideDocument17 pagesEasy ECG GuideDr.Chinmay Kulkarni83% (12)
- 2021 Sample Quantitative Chapters 1 and 2Document45 pages2021 Sample Quantitative Chapters 1 and 2Mark Jhuziel NacesNo ratings yet
- NCM 113 CHN 2 Lec SyllabusDocument24 pagesNCM 113 CHN 2 Lec SyllabusJann ericka Jao100% (3)
- EKG ExamplesDocument9 pagesEKG ExamplesMayer Rosenberg99% (235)
- ECG Study GuideDocument70 pagesECG Study GuideFatima Chrystelle NuñalNo ratings yet
- Four Principles of Moral DiscernmentDocument3 pagesFour Principles of Moral DiscernmentJann ericka JaoNo ratings yet
- ECG Study GuideDocument70 pagesECG Study GuideFatima Chrystelle NuñalNo ratings yet
- Hematology Handouts PDFDocument11 pagesHematology Handouts PDFJann ericka JaoNo ratings yet
- ThesisDocument2 pagesThesisJann ericka JaoNo ratings yet
- Moral Discernment, Evidence Based Medicine and Professional EthicsDocument11 pagesMoral Discernment, Evidence Based Medicine and Professional EthicsJann ericka JaoNo ratings yet
- s12888 021 03425 6Document15 pagess12888 021 03425 6Jann ericka JaoNo ratings yet
- ECG ReadingDocument11 pagesECG ReadingSuresh Shrestha100% (1)
- EKG Interpretation GuideDocument2 pagesEKG Interpretation GuideFabian Ramirez HincapiéNo ratings yet
- Final Written Proposal Template For Nursing Research1Document14 pagesFinal Written Proposal Template For Nursing Research1Mart Juaresa Yambao100% (8)
- Survey Questionnaire On Covid19Document8 pagesSurvey Questionnaire On Covid19TinNo ratings yet
- Nursing Thesis Proposal on Human Papilloma Vaccine AwarenessDocument24 pagesNursing Thesis Proposal on Human Papilloma Vaccine AwarenessCharlie Cotoner Falguera100% (1)
- Copar Book!Final DraftDocument98 pagesCopar Book!Final DraftVohn Andrae SarmientoNo ratings yet
- President Ramon Magsaysay State University: The Twelve Striking TechniquesDocument8 pagesPresident Ramon Magsaysay State University: The Twelve Striking TechniquesJann ericka JaoNo ratings yet
- Pathophysiology of Hellp Syndrome: Precipitating Risk Factors Predisposing Risk FactorsDocument2 pagesPathophysiology of Hellp Syndrome: Precipitating Risk Factors Predisposing Risk FactorsJann ericka JaoNo ratings yet
- Aggravating Factors Precipitating Factors Predisposing FactorsDocument4 pagesAggravating Factors Precipitating Factors Predisposing FactorsJann ericka JaoNo ratings yet
- Georgios Tsivgoulis Ultrasound in Neurology 2016Document23 pagesGeorgios Tsivgoulis Ultrasound in Neurology 2016JuliaNo ratings yet
- Pharmaceutical Care 5: Clinical Pharmacy Coronary Artery DiseaseDocument80 pagesPharmaceutical Care 5: Clinical Pharmacy Coronary Artery DiseaseJerson Aizpuro SuplementoNo ratings yet
- Systemic Blood Flow Is A CircuitDocument75 pagesSystemic Blood Flow Is A Circuitapi-76740522No ratings yet
- Cardiovascular Test Questions: "I Will Observe The Color of My Urine and Stool"Document36 pagesCardiovascular Test Questions: "I Will Observe The Color of My Urine and Stool"Melodia Turqueza GandezaNo ratings yet
- Lecture 30 - Pathology of AtherosclerosisDocument43 pagesLecture 30 - Pathology of Atherosclerosisapi-3703352100% (6)
- Final Case Study - CADDocument109 pagesFinal Case Study - CADPatricia Marie Buenafe100% (1)
- Seminar on Myocardial InfarctionDocument17 pagesSeminar on Myocardial InfarctionSuhas IngaleNo ratings yet
- GRE Verbal Reasoning Questions and AnswersDocument24 pagesGRE Verbal Reasoning Questions and AnswersTamunotonye Minaye-IlomboNo ratings yet
- Why Cholesterol Is Not The Cause of Heart DiseaseDocument2 pagesWhy Cholesterol Is Not The Cause of Heart Diseasejacksparrow2No ratings yet
- Esc Cardiomed (3 Edn) : Epidemiology and Risk FactorsDocument12 pagesEsc Cardiomed (3 Edn) : Epidemiology and Risk FactorsNadhila IchwanNo ratings yet
- Catatan Kuliah KardiologiDocument99 pagesCatatan Kuliah KardiologiAdhe Marlin SanyotoNo ratings yet
- Sample Cardiac Calcium Scoring ReportDocument3 pagesSample Cardiac Calcium Scoring ReportZyad DoskiNo ratings yet
- Therapy Final Questions on Rheumatic Fever and TreatmentDocument102 pagesTherapy Final Questions on Rheumatic Fever and TreatmentManushi HenadeeraNo ratings yet
- Special Pathology Solved KMU SEQs by RMC StudentsDocument145 pagesSpecial Pathology Solved KMU SEQs by RMC StudentsAamir Khan0% (1)
- Abdominal Aortic Aneurysm and Atherosclerosis FINALDocument23 pagesAbdominal Aortic Aneurysm and Atherosclerosis FINALErica P. ManlunasNo ratings yet
- Cardiovascular MedicineDocument2,877 pagesCardiovascular Medicinediyah100% (1)
- Cardiovascular Disorders: Coronary AtherosclerosisDocument6 pagesCardiovascular Disorders: Coronary AtherosclerosisHazel BandayNo ratings yet
- SCAI Interventional Cardiology ReviewDocument1,369 pagesSCAI Interventional Cardiology ReviewSajjad HussainNo ratings yet
- Physical Fitness Short Note (SPSC 1011) Unit One 1. 1. Concepts of Physical Fitness1 1.1. 1. Meanings and Definitions of Physical FitnessDocument62 pagesPhysical Fitness Short Note (SPSC 1011) Unit One 1. 1. Concepts of Physical Fitness1 1.1. 1. Meanings and Definitions of Physical Fitnesseyob astatkeNo ratings yet
- Emory Cardiology Newsletter June 2009Document9 pagesEmory Cardiology Newsletter June 2009hnaguNo ratings yet
- Evolocumab 2Document13 pagesEvolocumab 2Rania El-DesokyNo ratings yet
- Cardiac Rehab BookletDocument32 pagesCardiac Rehab BookletAbu Bakr Siddique100% (1)
- Color Atlas of Forensic Pathology by Dinesh Fernando and Sulochana Wijetunge. Vol IDocument199 pagesColor Atlas of Forensic Pathology by Dinesh Fernando and Sulochana Wijetunge. Vol IGorka AguirreNo ratings yet
- Achim 2022Document8 pagesAchim 2022BözskeNo ratings yet
- Diet and Health: Whitney & Rolfes - Understanding Nutrition, 12 EditionDocument59 pagesDiet and Health: Whitney & Rolfes - Understanding Nutrition, 12 EditionconsultationemailNo ratings yet
- Causes of Ischemic Stroke: October 2010Document19 pagesCauses of Ischemic Stroke: October 2010Pajokka 10No ratings yet
- Case Study Acute Myocardial InfarctionDocument11 pagesCase Study Acute Myocardial InfarctionChristine Elaine Batusin Ilagan91% (23)
- Management of Stroke PDFDocument6 pagesManagement of Stroke PDFtarmo angsanaNo ratings yet
- Coronary Artery DiseaseDocument22 pagesCoronary Artery DiseaseMark MahumotNo ratings yet
- Case Study NstemiDocument24 pagesCase Study NstemiNana Yunus100% (2)