Professional Documents
Culture Documents
Georgios Tsivgoulis Ultrasound in Neurology 2016
Uploaded by
JuliaOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Georgios Tsivgoulis Ultrasound in Neurology 2016
Uploaded by
JuliaCopyright:
Available Formats
Review Article
Ultrasound in
Address correspondence to
Dr Georgios Tsivgoulis,
Second Department of
Neurology, University of
Neurology Athens School of Medicine,
Iras 39, Gerakas Attikis,
Athens, Greece 15344,
tsivgoulisgiorg@yahoo.gr.
Georgios Tsivgoulis, MD, PhD, MSc, RVT;
Relationship Disclosure:
Andrei V. Alexandrov, MD, RVT Dr Tsivgoulis serves on the
editorial boards of Stroke and
the Journal of Neuroimaging
and has received research/
ABSTRACT grant support from the European
Purpose of Review: Low cost, avoidance of irradiation, and high temporal resolution Regional Development Fund.
Dr Alexandrov serves on the
are inherent advantages of ultrasound imaging that translate into multiple clinical uses in editorial board of the Journal
many domains of neurology. This article presents clinical uses of ultrasound examination of Neuroimaging.
in cerebrovascular, neurodegenerative, and peripheral nervous system diseases. Unlabeled Use of
Recent Findings: Modern treatment and prevention of ischemic stroke rely on prompt Products/Investigational
Use Disclosure:
diagnosis. Ultrasonography has found a place as a noninvasive screening test and Drs Tsivgoulis and
bedside technique that provides estimates of the degree of stenosis as well as Alexandrov report
hemodynamic and structural information about intracranial and extracranial vessels no disclosures.
in real time. Other standard applications of neurosonology include detection of * 2016 American Academy
of Neurology.
vasospasm in patients with subarachnoid hemorrhage, selection of appropriate
candidates for blood transfusion among patients with sickle cell anemia (primary
stroke prevention), right-to-left shunt testing, emboli detection, vasomotor reactivity
assessment, and noninvasive confirmation of cerebral circulatory arrest. Improvement
in image quality permits novel uses of ultrasonography in neurodegenerative and
peripheral nervous system disorders, providing clinically important information that
is complementary to the clinical examination and electrophysiology. Transcranial
parenchymal sonography may assist in the differential diagnosis of movement dis-
orders, while peripheral nerve ultrasound using high-frequency probes may provide
structural information regarding the underlying etiology of entrapment neuropathies.
Summary: The indications for neurosonology are rapidly expanding, increasing its
applicability outside the field of cerebrovascular diseases. Ultrasound testing is a
noninvasive easily repeatable bedside investigation providing clinically relevant
information on a wide spectrum of neurologic disorders.
Continuum (Minneap Minn) 2016;22(5):1655–1677.
INTRODUCTION Vascular ultrasound was the first
Excellent safety, very high temporal modality adopted in clinical neurology
and high spatial resolution, real-time for the evaluation of extracranial
evaluation, low cost, and the ability to (1970s) and intracranial (1980s) vascu-
perform examinations at the bedside lature before the widespread availability
are some of the key advantages of of multimodal CT and MRI. Brightness-
medical ultrasound. These advantages mode display (B-mode) consists of a
explain why diagnostic ultrasound has two-dimensional grayscale image de-
revolutionized many medical special- rived from scanning a plane through
ties, including neurology. Several med- the body by an array of transducers.
ical schools in the United States already B-mode has been in clinical use for many
include ultrasound in their curriculum years for the evaluation of the vessel
for all medical students, using it to teach wall and plaques in the extracranial
anatomy and instructing them in how arteries (Figure 13-1). Doppler mode
to scan with portable equipment. makes use of the Doppler effect in
Continuum (Minneap Minn) 2016;22(5):1655–1677 www.ContinuumJournal.com 1655
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Ultrasound
sonology to describe a variety of non-
invasive imaging and nonimaging
ultrasound techniques that have
established clinical value in evaluating
patients with stroke or those at risk for
stroke. The extracranial internal carotid,
common carotid, external carotid, and
vertebral arteries can be assessed by
cervical duplex (simultaneous presen-
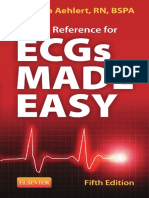
Cervical duplex ultrasound (brightness
tation of B-mode image and Doppler
FIGURE 13-1 waveform) ultrasonography, while the
mode, horizontal plane). The common
carotid artery (CCA) is bifurcating into the middle cerebral, anterior cerebral, pos-
internal carotid artery (ICA) and external carotid artery
(ECA). Note an arterial branch originating from the ECA (red terior cerebral, ophthalmic, intracranial
asterisk). The presence of arterial branch is essential for the vertebral, and basilar arteries can be
ultrasound differentiation between cervical ECA (several
arterial branches) and cervical ICA (no arterial branch). investigated by transcranial Doppler
(TCD) or transcranial color-coded du-
plex sonography. Other specialized
KEY POINT measuring blood flow. Information tests that can be used to ascertain the
h The extracranial internal about blood direction and velocity is pathogenic mechanism of stroke or risk
carotid, common projected on the B-mode image, of stroke recurrence include emboli
carotid, external carotid,
encoded in colors. Spectral Doppler detection with or without contrast
and vertebral arteries
depicts a waveform containing infor- injection, vasomotor reactivity testing,
can be assessed by
mation about velocity, resistance, and and real-time spectral Doppler moni-
cervical duplex
(simultaneous
flow direction. Imaging improvement in toring during treatment or specific
presentation of B-mode has permitted the evaluation maneuvers (eg, head turn, blood pres-
brightness-mode image of the adult brain parenchyma and sure manipulation).
and Doppler waveform) opened new horizons in the imaging
ultrasonography, while of neurodegenerative disorders. Novel Ultrasound Assessment of
the middle cerebral, high-frequency probes have permitted Extracranial Arteries
anterior cerebral, high-quality imaging of peripheral Cervical duplex ultrasonography is a
posterior cerebral, nerves, providing morphologic infor- noninvasive neuroimaging modality
ophthalmic, intracranial mation that is complementary to the for the evaluation of both vessel wall
vertebral, and basilar neurophysiologic findings. However, features and blood flow parameters in
arteries can be it should be noted that despite recent cervical arteries. Cervical duplex ultra-
investigated by technologic advances, neurosonology
transcranial Doppler or
sonography provides real-time infor-
continues to remain highly operator mation about the presence of an
transcranial color-coded
dependent and requires extensive train- atherosclerotic plaque, including its
duplex sonography.
ing to acquire both the required theo- length, composition, protrusion and
retical knowledge and the necessary surface, range of resulting vascular
scanning skills. This article presents a stenosis or occlusion, presence of a
brief and practical overview of the dissection, and other significant imag-
main current applications of ultra-
ing findings in patients with acute
sound in neurology.
ischemic stroke (Table 13-1). Cervical
duplex ultrasonography can directly
CEREBROVASCULAR DISEASES visualize atherosclerotic plaque com-
A major cause of disability and death, position that can be classified based on
ischemic stroke ensues after occlusion its echogenicity. Uniformly hyperechoic
of extracranial or intracranial arteries. carotid plaques are mainly composed
This article uses the term neuro- of fibrotic tissue needed for plaque
1656 www.ContinuumJournal.com October 2016
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINTS
h Cervical duplex
TABLE 13-1 Applications of Cervical Duplex Ultrasonography in
Patients With Acute Ischemic Stroke ultrasonography can
directly visualize
b Information about plaque composition and surface (eg, lipid, hemorrhage, atherosclerotic plaque
fibrous content, ulceration, superimposed thrombus) composition that can be
classified based on its
b Diagnosis of the degree of carotid artery stenosis (normal, 0Y49%,
echogenicity. Cervical
50Y69%, 70Y99%, near occlusion, occlusion)
duplex ultrasonography
b Diagnosis of the degree of vertebral artery stenosis (G50%, 950%, occlusion) also allows rapid
b Detection of intraluminal thrombus in cervical vessels detection of internal
carotid artery thrombosis
b Diagnosis of subclavian steal syndrome and differentiation
b Diagnosis/suspicion of uncommon causes of stroke (eg, cervical artery between chronic internal
dissection, fibromuscular dysplasia, aortic arch dissection) carotid artery occlusion
with or without preexisting
b Complementary information in the diagnosis of temporal arteritis
atheromatous stenosis.
b Indirect information for distal intracranial vessel occlusion
h Peak systolic velocity,
b Indirect information for heart rate and heart valves end-diastolic velocity,
and the systolic internal
b Diagnosis of other conditions not related to acute stroke (eg, carotid
body tumor) carotid artery/common
carotid artery velocity
ratio are essential
ultrasound parameters
stability. In contrast, heterogeneous be conducted with grayscale (B-mode), for North American
(and predominantly hypoechoic) power-mode, or color Doppler and Symptomatic Carotid
plaques consisting of matrix deposi- spectral Doppler ultrasound, and Endarterectomy Trial
tion, cholesterol accumulation, ne- reported using NASCET ranges of ICA grading ranges of
extracranial internal
crosis, calcification, and intraplaque stenosis (normal, 0% to 49%, 50% to
carotid artery disease.
hemorrhage are considered unstable, 69%, 70% to 99%, near occlusion,
being the source of artery-to-artery occlusion). A characteristic example of h Peak systolic velocity and
embolic strokes.1 severe (70% to 99%) ICA stenosis is end-diastolic velocity
must be assessed in the
Peak systolic velocity, end-diastolic presented in Case 13-1.
prestenotic, stenotic, and
velocity, and the systolic internal ca- Cervical duplex ultrasonography al-
poststenotic segments of
rotid artery (ICA)/common carotid ar- lows rapid detection of ICA thrombosis the vessel, and ultrasound
tery (CCA) velocity ratio are essential and differentiation from chronic ICA interpretation must refer
ultrasound parameters for grading the occlusion with or without preexisting to the North American
percentage of stenosis in extracranial atheromatous stenosis. These acute Symptomatic Carotid
carotid artery steno-occlusive disease. findings may prompt consideration of Endarterectomy Trial
Peak systolic velocity and end-diastolic carotid endarterectomy (Case 13-2). strata of internal carotid
velocity must be assessed in the Ultrasound diagnosis and classifica- artery stenosis.
prestenotic, stenotic, and poststenotic tion of vertebral artery stenosis is more
segments of the vessel. The Society of demanding. Vertebral artery asymme-
Radiologists in Ultrasound Consensus try is common, and a hypoplastic
Conference reached multidisciplinary vertebral artery may terminate in the
agreement on criteria to predict clini- posterior inferior cerebellar artery. An-
cally relevant strata of ICA stenosis atomic variants and abnormalities (eg,
corresponding to the North American stenosis, occlusion) of the contralateral
Symptomatic Carotid Endarterectomy vertebral artery influence vertebral
Trial (NASCET) criteria (Table 13-2).2 artery flow. Severe stenosis in the
All carotid artery examinations should carotid arteries may also affect blood
Continuum (Minneap Minn) 2016;22(5):1655–1677 www.ContinuumJournal.com 1657
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Ultrasound
TABLE 13-2 Peak Systolic Velocities, End-Diastolic Velocities, and Doppler Spectra With
Varying Degrees of Extracranial Internal Carotid Artery Stenosisa
Peak Systolic
ICA Stenosis Peak Systolic End-Diastolic Velocity ICA/
Range Velocity (cm/s) Velocity (cm/s) CCA Ratio Plaque
Normal G125 G40 G2 None
0Y49% G125 G40 G2 G50% diameter reduction
50Y69% 125Y230 40Y100 2Y4 Q50% diameter reduction
70Y99% 9230 9100 94 Q50% diameter reduction
Near occlusion High/low or Variable Variable Significant, detectable
undetectable lumen
Occlusion Undetectable NA NA Significant, no detectable
lumen
CCA = common carotid artery; ICA = internal carotid artery; NA = not applicable.
a
Modified with permission from Grant EG, et al, Radiology.2 B 2003 Radiological Society of North America. pubs.rsna.org/doi/full/10.1148/
radiol.2292030516.
KEY POINT flow in the vertebral artery due to minimal diastolic blood flow that con-
h Ultrasonography recruitment of collaterals. Vertebral curs with high-resistance bidirectional
may assist in the artery stenoses are most commonly Doppler signal. In B-mode imaging, a
diagnosis of carotid or located in the origin from the subcla- tapered lumen with a characteristic
vertebral artery vian artery (V0 segment) followed by string sign appearance may be shown,
dissection. Cervical
the atlas loop/intracranial segments, as well as a floating intimal flap. The
duplex ultrasonography
while intertransverse segments are less true lumen can be compressed by the
may detect reversed
systolic blood flow commonly affected. Criteria for verte- false lumen thrombus, and subse-
at the origin of the bral artery stenoses are not based on a quently a low-velocity Doppler wave-
vessel and absent or peak systolic velocity cutoff but on form can be recorded. The flow
minimal diastolic focal and significant peak systolic ve- direction in a patent false lumen may
blood flow that locity increase, since tortuosity of the fluctuate from forward to reverse or
concurs with proximal vertebral artery segment, ICA may be bidirectional. If a dissection is
high-resistance lesions, and vertebral artery asymmetry found ascending from the proximal
bidirectional may result in relatively high velocities. CCA, it indicates aortic dissection. In
Doppler signal. The velocity increase should be found patients with a distal cervical ICA
over a relatively short segment of the dissection (that has not descended to
vertebral artery with normal or de- the proximal ICA), a retromandibular
creased prestenotic and poststenotic high-velocity signal may be the only
velocities.7 Elongated and multiple ste- sign of dissection.8
noses in the vertebral artery may not Ultrasound detection of vertebral
produce focal velocity elevations, which artery dissection in the V2 through V4
could be a source of false-negative cer- segments (Figure 13-4) is challenging
vical duplex ultrasonography studies. since no well-defined and predictable
Ultrasonography may assist in the imaging findings have been identified.
diagnosis of carotid artery dissection. Absent blood flow, low bidirectional
Cervical duplex ultrasonography may flow, or low poststenotic velocities can
detect reversed systolic blood flow at be detected at the level of the atlas
the origin of the ICA and absent or loop, a frequent site of dissection. A
1658 www.ContinuumJournal.com October 2016
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Case 13-1
A 58-year-old man with a history of hypertension, hypercholesterolemia, and smoking presented with
recurrent episodes of transient hemiparesis lasting between 20 and 40 minutes over the previous 2 days.
His blood pressure was 178/94 mm Hg, and his ABCD2 score (age, blood pressure, clinical features,
duration, presence of diabetes mellitus) was 4. He reported that he developed symptoms after standing
up or walking for a period longer than 30 minutes. Emergent neurosonology evaluation disclosed the
presence of hypoechoic material in the distal right internal carotid bulb coupled by the absence of flow
in color-mode display on cervical duplex ultrasound (Figure 13-2). Transcranial duplex sonography showed
the presence of collateral flow via ipsilateral ophthalmic artery flow reversal (Figure 13-2), while the
flow in the ipsilateral proximal middle cerebral artery was severely blunted (mean flow velocity of
60 cm/s, pulsatility index of 0.42; normal values being less than 100 cm/s and 0.6 to 1.1, respectively).
The diagnosis of acute internal carotid artery occlusion causing orthostatic hypoperfusion syndrome was
made.3 Digital subtraction angiography confirmed the presence of an acute right internal carotid artery
occlusion. Brain MRI with diffusion-weighted imaging excluded the presence of an acute infarction.
The patient was put in the head-down position and treated with IV isotonic fluids and the combination of
oral aspirin (100 mg) and clopidogrel (75 mg) while his systolic blood pressure was maintained at the
levels of 160 mm Hg to 180 mm Hg for the first 5 days of acute cerebral ischemia. The patient did not
develop any recurrent symptoms during his hospitalization.
FIGURE 13-2 Imaging of the patient in Case 13-1. Acute internal carotid artery occlusion originally
diagnosed by cervical duplex ultrasound (A) and subsequently confirmed by digital
substraction angiography (C). Note the presence of hypoechoic material in the
distal internal carotid artery bulb coupled by absence of flow in color-mode display. Transcranial
color-coded duplex sonography displays the presence of collateral flow via ipsilateral ophthalmic
artery flow reversal (B, detection of retrograde low-resistance flow in ipsilateral ophthalmic artery).
Comment. This case highlights the importance of neurosonology in identifying patients with acute cerebral
ischemia due to hypoperfusion caused by steno-occlusive intracranial or extracranial arterial disease. Acute
blood pressure lowering in this subgroup of patients may be harmful and cause further neurologic
deterioration. Putting the patient in the head-down position and maintaining a moderately elevated blood
pressure level appears to be the preferable therapeutic approach in patients with orthostatic transient ischemic
attacks or strokes caused by cerebral hypoperfusion distal to an extracranial or intracranial large vessel occlusion.4
Continuum (Minneap Minn) 2016;22(5):1655–1677 www.ContinuumJournal.com 1659
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Ultrasound
Case 13-2
A 64-year-old man with a history of hypertension, diabetes mellitus, coronary artery disease, and
smoking presented with a mild right hemiparesis 12 hours following symptom onset. His National Institute
of Health Stroke Scale (NIHSS) score was 3. Emergent neurovascular ultrasound disclosed the presence of
a heterogeneous plaque with an overlying thrombus in his left internal carotid artery (Figure 13-3)
causing severe stenosis (70% to 99% North American Symptomatic Carotid Endarterectomy Trial
range). Transcranial Doppler monitoring of the ipsilateral proximal middle cerebral artery recorded the
FIGURE 13-3 Imaging of the patient in Case 13-2. Cervical duplex ultrasound (A, B) depicts a
heterogeneous plaque (A, green arrowheads) with an overlying thrombus
(A, white arrowheads) causing a hemodynamically (70% or greater) significant
carotid artery stenosis. Note the presence of aliasing on color-mode display (A) and the
elevated peak systolic velocity (236 cm/s) and end-diastolic velocity (112 cm/s) on spectral
display (B). CT angiography (C, D) confirms ultrasound findings and depicts the presence of an
overlying thrombus protruding in the vessel lumen (C, red circle; D, white arrowhead). The
patient underwent emergent carotid endarterectomy, removing both atherosclerotic plaque
and overlying thrombus (E).
Continued on page 1661
1660 www.ContinuumJournal.com October 2016
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Continued from page 1660
presence of high-intensity transient signals indicative of microembolism in real time. CT angiography
confirmed the ultrasound findings and depicted the presence of a large atherosclerotic plaque with an
overlying thrombus protruding in the left internal carotid artery lumen (Figure 13-3). Brain MRI with
diffusion-weighted imaging showed numerous small foci of restricted diffusion in the territory of
the left middle cerebral artery. Artery-to-artery embolism distal to a symptomatic carotid artery
stenosis was considered as the underlying mechanism of acute cerebral ischemia. The patient underwent
emergent carotid endarterectomy at 29 hours following symptom onset (Figure 13-3). He was discharged
on the fifth day of hospitalization with an NIHSS score of 1.
Comment. This case highlights the importance of neurosonology in identifying patients with
symptomatic carotid artery stenosis causing distal microembolization. These patients carry an
excessively high risk (nearly tenfold) of recurrent stroke5 and should undergo carotid endarterectomy
during the first 14 days after transient ischemic attack or nondisabling stroke.6 Neurosonology is a
noninvasive and inexpensive neuroimaging modality that can be rapidly applied at the bedside of
patients with acute cerebral ischemia; it may provide real-time diagnostic and prognostic information
to help make patient management decisions.
dissection causing stenosis at the V1 or cerebral arteriogram) should be
segment may be detected by ultra- performed even if ultrasound results
sound; absent blood flow may be are inconclusive.
found in the intertransverse segments, Takayasu arteritis presents with
and a localized broadening of a vessel smooth homogenous concentric thick-
diameter at V1 may be seen with se- ening of the arterial wall on B-mode
vere stenosis or occlusion. Direct visu- imaging in proximal cervical vessels
alization of intramural hematoma by (common carotid artery, innominate
ultrasound is rare; it can be easily missed artery, and subclavian artery), which
if no significant stenosis is evident or can be easily identified by cervical
if it is located outside an accessible duplex ultrasonography by the typi-
intratransverse arterial segment.9 When cal macaroni sign (Figure 13-5). In
a clinical suspicion of vertebral artery contrast to atherosclerotic disease,
dissection exists, further imaging work- patients with Takayasu arteritis have an
up (MRI with fat-saturation sequences affected CCA with sparing of the ICA
FIGURE 13-4 Extracranial vertebral artery (VA) segments on cervical duplex ultrasound. VA
origin (V0) from the subclavian artery is displayed on the right panel, the
pretransverse VA segment (V1) located proximally to the C6 transverse process
is displayed in the middle panel, and the transverse VA segment (V2) is displayed in the
left panel.
RVA = right vertebral artery.
Continuum (Minneap Minn) 2016;22(5):1655–1677 www.ContinuumJournal.com 1661
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Ultrasound
FIGURE 13-5 Cervical duplex ultrasound showing typical macaroni sign in the right common carotid artery (CCA)
of a 32-year old woman with Takayasu arteritis (A, B-mode). The macaroni sign represents smooth,
homogeneous, and moderately echogenic circumferential thickening of the arterial wall (red
arrowheads) that occurs in Takayasu arteritis. Note the elevation of velocities (peak-systolic velocity: 257 cm/s,
end-diastolic velocity: 76 cm/s) due to constriction of CCA lumen in color-mode display (B).
KEY POINT and external carotid artery. More- coded duplex sonography to provide
h Intracranial cerebral over, contrast-enhanced cervical du- real-time flow findings (Figure 13-7)
vasculature can be plex ultrasonography can reliably that are complementary to information
assessed by transcranial
identify vulnerable plaques at the provided by CT angiography (CTA) or
Doppler or transcranial
vessel wall lumen, by providing direct multimodal MRI. TCD is a diagnostic
color-coded duplex
sonography to provide
visualization of intraplaque neovas- method increasingly used for the
real-time flow findings cularization and improving delinea- diagnosis of cerebrovascular diseases
that are complementary tion of plaque ulcers. 10 Takayasu (Table 13-3). TCD identifies intracra-
to information provided arteritis may also present with subcla- nial stenoses, distal emboli, and col-
by CT angiography or vian steal syndrome caused by subcla- lateral flow and helps determine
multimodal MRI. vian artery stenosis. hemodynamic significance of extra-
Giant cell arteritis can present cranial or intracranial steno-occlusive
with stroke symptoms, typically of the lesions, monitor recanalization during
vertebrobasilar territory. In these cases, thrombolytic therapy in real time, deter-
the vertebral artery may rarely show mine the stroke pathogenic mechanism,
hypoechoic wall thickening on cervical and select the next and most appro-
duplex ultrasonography. An examina- priate step in patient management.13
tion of the superficial temporal artery A fast-track insonation protocol
with high-frequency 12-MHz to 15-MHz has been developed for rapid extra-
B - m o de transducers can detect cranial and intracranial artery eval-
hypoechoic circumferential thickening uation in the emergency setting of
(the halo sign) (Figure 13-6).11 The acute ischemic stroke to diagnose large
halo sign is moderately sensitive (68%) artery intracranial steno-occlusive le-
but highly specific (91%) when present sions, recanalization, and reocclusion.14
at the superficial temporal artery and The choice of fast-track insonation
can also be used to guide biopsy as steps is determined by clinical localiza-
well as monitor treatment.12
tion of the ischemic arterial territory.
Ultrasound Assessment of Most studies can be accomplished
Intracranial Arteries within minutes by experienced sonog-
Intracranial cerebral vasculature can be raphers at the bedside in parallel with
assessed by TCD or transcranial color- the neurologic examination in the
1662 www.ContinuumJournal.com October 2016
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
FIGURE 13-6 Ultrasound findings in giant cell arteritis. Extracranial duplex ultrasound of the left superficial temporal artery
(STA) shows reduced color filling and vessel-wall thickening in the form of a dark halo (hypoechoic
circumferential thickening) in axial (A, red arrows) and longitudinal (B, blue arrow) planes. Note the normal
color filling in the right STA in axial (C) and longitudinal (D) planes. The ultrasound findings in the left STA wall (unilateral
halo sign) are indicative of giant cell arteritis. The diagnosis is confirmed by magnetic resonance angiography (MRA) (E)
depicting unilateral severe left STA stenosis/obstruction (red arrow) and temporal artery biopsy showed inflammatory
infiltrates (including giant cells) involving the entire vessel wall with marked intimal thickening. Note the normal appearance
of the right STA (E, blue arrow).
emergency department without evaluating patients with acute ischemic
delaying treatment. Overall, bedside stroke with acute proximal arterial oc-
TCD examination in the emergency clusion or stenosis of an intracranial
department had a satisfactory agree- artery (Figure 13-8). Its efficacy de-
ment to brain CTA in the evaluation of pends on symptomatic artery localiza-
patients with acute ischemic stroke. tion, onset-to-insonation time, and
TCD is a highly accurate and reliable acute ischemic stroke severity. TCD
bedside diagnostic examination for can reveal artery occlusion in more
FIGURE 13-7 Depiction of proximal intracranial arteries of the circle of Willis in a healthy individual using
transcranial color-coded duplex sonography (A). The intensity mode, or power mode,
allows better visualization of the arterial flow (B).
ACA = anterior cerebral artery; MCA = middle cerebral artery; PCA = posterior cerebral artery.
Continuum (Minneap Minn) 2016;22(5):1655–1677 www.ContinuumJournal.com 1663
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Ultrasound
TABLE 13-3 Applications of Transcranial Doppler or Transcranial
Color-Coded Duplex Sonography in Patients With Acute
Ischemic Stroke
b Bedside confirmation of vascular origin of the presenting symptoms and
determination of underlying stroke mechanism
b Fast detection and localization of occlusion/stenosis
b Mapping of the collateral circulation
b Detection of cerebral embolism in real time and quantification of
right-to-left shunt
b Real-time monitoring of recanalization in patients treated with systemic
thrombolysis
b Selection of patients for intraarterial reperfusion procedures
b Monitoring of rescue intraarterial procedures (eg, detection of
reocclusion, air embolism, hyperperfusion syndrome)
b Detection of supratentorial intracerebral hemorrhage at the bedside
following acute reperfusion therapies (application of transcranial
color-coded duplex sonography)
b Potential augmentation of clot lysis and clinical recovery
(sonothrombolysis)
than 90% of patients with acute ische- Ultrasound may also assist in map-
mic stroke treated with recombinant ping of collateral cerebral circulation.
tissue-type plasminogen activator Efficient collateral circulation helps
within 3 hours from symptom onset maintain cerebral perfusion in the set-
when NIHSS score is 10 or more.14 ting of acute ischemic stroke and is
FIGURE 13-8 Transcranial Doppler findings in intracranial stenosis. A, Power-motion-mode transcranial Doppler
depicts the presence of a hemodynamically (70% or greater) significant right proximal middle
cerebral artery stenosis. Note the presence of elevated mean (141 cm/s) and peak (209 cm/s)
systolic flow velocities and the presence of systolic bruit on power-motion-mode (depicted as systolic flow gaps) and
spectral (circles) displays. B, Digital substraction angiography confirmed the diagnosis of severe (79%) proximal
middle cerebral artery stenosis (arrow).
1664 www.ContinuumJournal.com October 2016
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
KEY POINTS
associated with reduced infarct volume TIBI flow grades were found to corre- h Transcranial Doppler
and better functional outcome. The late strongly with stroke severity, assesses recanalization
main collateral pathways are the ante- mortality, and clinical improvement. and potential reocclusion
rior and posterior communicating ar- Rapid arterial recanalization is associ- in real time in patients
teries, reversed ophthalmic artery, and ated with better short-term improve- with acute ischemic
reversed basilar artery. These channels ment. On the contrary, slow flow stroke treated with
come into play only if a change occurs improvement and dampened TIBI systemic or intraarterial
in pressure gradients between two flow signals are less favorable prog- reperfusion therapies.
anastomosing arterial systems. TCD nostic signs that indicate the need for h A novel application of
can provide real-time information on further reperfusion therapies, such as neurosonology is the
the blood flow direction and velocity mechanical thrombectomy. TIBI flow assessment of an
intracranial arterial steal
of the collateral pathways. Activation grading can be used in follow-up after
syndrome and evaluation
of a collateral flow pathway implies initial CTA assessment to determine if of vasomotor reactivity
the presence of a flow-limiting lesion the patient still has a persisting occlu- of intracranial arteries.
proximal to the origin of the collateral sion or reocclusion or had full recanali-
channel.15 zation without clinical improvement to
TCD and transcranial color-coded avoid the need for repeat CTA in acute
duplex sonography may assess recan- ischemic stroke within the time frame
alization and potential reocclusion in for mechanical thrombectomy.
real time in patients with acute ische- A novel application of neurosonology
mic stroke treated with systemic or is the assessment of intracranial arterial
intraarterial reperfusion therapies. steal syndrome and evaluation of vaso-
Spontaneous recanalization of a mid- motor reactivity of intracranial arteries.
dle cerebral artery (MCA) occlusion Once a feeding vessel is blocked,
occurs at a rate of approximately 6% compensatory distal vasodilation de-
per hour after symptom onset, and IV creases resistance to attract blood flow
tissue plasminogen activator doubles through collateral channels. Counter-
the chance of complete recanalization intuitively, this hemodynamic phenom-
to almost 13% during the first hour enon may, in turn, lead to further
of treatment, with a median time of perfusion decrease of ischemic brain
35 minutes after the bolus infusion.16 tissues (in which arteries cannot dilate
TCD provides a noninvasive bedside any further). This lack of further dilation
tool for real-time monitoring of arterial may not counteract the steal of blood
recanalization. The thrombolysis in by normally perfused areas that main-
brain ischemia (TIBI) flow-grading tain the capability for vasodilation with
system was developed to evaluate additional stimuli. This hemodynamic
residual flow noninvasively and in real steal phenomenon can be detected on
time in analogy to the thrombolysis in TCD in patients with acute ischemic
myocardial infarction (TIMI) flow stroke and has been termed reversed
grades.17 TIBI grade 5 corresponds Robin Hood syndrome in analogy with
to normal blood flow, grade 4 to stenotic ‘‘rob the poor to feed the rich.’’18
blood flow (accelerated), grade 3 to A TCD vasomotor study is a simple
dampened blood flow (decreased ve- method to assess vasomotor reactivity
locities compared to the contralateral in acute ischemic stroke and can iden-
intracranial artery), grade 2 to blunted tify patients at high risk for stroke in
blood flow (flattened waveform), the setting of symptomatic or asymp-
grade 1 to minimal blood flow (absent tomatic extracranial internal carotid
diastolic flow), and grade 0 to no flow. artery stenosis or occlusion. During this
Continuum (Minneap Minn) 2016;22(5):1655–1677 www.ContinuumJournal.com 1665
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Ultrasound
KEY POINTS
h The transcranial noninvasive test, TCD is used to mea- benefit from prophylactic transfusion
Doppler bubble sure velocity response to voluntary (Table 13-4).13 Ischemic strokes in
test is more sensitive breath-holding for 30 seconds, which children with sickle cell anemia primar-
than transthoracic induces hypercapnia and serves as a ily result after stenosis of the MCA or
echocardiography (with natural vasodilatory stimulus.19 distal intracranial ICA, and some chil-
or without contrast Another indication for TCD is the dren may develop moyamoya syn-
injection) in detection of noninvasive detection of cerebral em- drome. The Stroke Prevention in
a right-to-left shunt bolization and presence of right-to-left Sickle Cell Anemia (STOP) trial showed
through a patent shunts, such as patent foramen ovale, that time-averaged maximum mean
foramen ovale. as a conduit of paradoxical embolism. velocity greater than 200 cm/s in the
h Transcranial Doppler Microembolic signals can be detected terminal ICA or MCA is associated with
stratifies the risk of during TCD monitoring in patients with a 10% annual risk for stroke.13 Trans-
patients with sickle cell acute ischemic stroke or transient is- fusion to lower hemoglobin S concen-
anemia and those in chemic attacks as signals of high inten- trations to less than 30% of total
need of blood
sity and short duration within the hemoglobin in these children decreases
transfusions for primary
Doppler spectrum; they represent solid time-averaged maximum mean for
stroke prevention. Those
who meet transcranial
or gaseous particles within the blood several weeks, reduces blood coagu-
Doppler criteria for blood flow. Although not causing immediate lation biomarkers,22 and, most impor-
transfusions should stay symptoms, these embolic signals are tant, reduces the relative risk of stroke
on transfusions since clinically important, as they can identify by 92%. Children at risk continue to
these children remain an embolic mechanism and point to the benefit from transfusions and should
at high risk of stroke source of embolism in patients with continue to receive treatment to sustain
if transfusions stroke or transient ischemic attack. the primary stroke prevention benefit,
are discontinued. TCD is the gold standard of detection, as shown in the STOP 2 trial.23 It should
h One of the first quantification, and localization of cere- be noted that not all pediatric strokes
applications of bral embolization in real time. Patients in sickle cell anemia are predicted by
transcranial Doppler in with symptomatic carotid artery steno- TCD as other mechanisms come into
clinical use has been sis and microembolic signals on TCD play, such as artery dissection, embo-
the identification of were found to benefit from early ca- lism, small artery infarction, and
cerebral vasospasm rotid endarterectomy.20 hypercoagulable states.
after subarachnoid
Paradoxical embolism is a possible One of the first applications of TCD
hemorrhage.
mechanism of acute ischemic stroke in in clinical use has been the identifica-
patients with right-to-left shunts. The tion of cerebral vasospasm after sub-
TCD bubble test is equivalent or even arachnoid hemorrhage (SAH). Blood
superior to both transthoracic and extravasation has a toxic effect on
transesophageal echocardiography in brain arteries and leads to lumen
detection of right-to-left shunt through narrowing that, when severe enough,
a patent foramen ovale. 13 Power- can lead to ischemic lesions. TCD can
motion-mode Doppler may further estimate the severity of vasospasm by
increase the yield. TCD criteria for detecting increased blood velocities
grading right-to-left shunts have been in areas of vasospasm (Table 13-4).13
proposed to distinguish incidental Baseline TCD measurements are
from pathogenic right-to-left shunts in obtained, and the patient is monitored
patients with acute ischemic stroke.21 every day or every other day through-
TCD is a validated diagnostic tool for out Day 7 (all grades) and Day 10 (Hunt-
children with sickle cell anemia be- Hess grades 2+) or until vasospasm
tween the ages of 2 and 16 years who resolution. It is recommended that
have not sustained a stroke to identify extracranial internal carotid artery ve-
those at high risk for stroke who could locities be recorded to adjust for
1666 www.ContinuumJournal.com October 2016
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TABLE 13-4 Established Clinical Indications and Expected Outcomes of Transcranial Doppler
Testing in Sickle Cell Anemia, Subarachnoid Hemorrhage, and Brain Deatha
Broad Indication Specific Indications Expected Outcomes
Sickle cell anemia Children Robust first-ever stroke risk reduction based on transcranial
Doppler (TCD) criteria for the need of blood transfusion
and continuing use of blood transfusions.
Subarachnoid Days 2Y5 TCD can detect development of vasospasm days before it
hemorrhage can become clinically apparent. This information can be
used by intensivists to step up hemodynamic management
of these patients.
Days 5Y12 TCD can detect progression to the severe phase of spasm
when development of the delayed ischemic deficit due to
perfusion failure through the residual lumen is the greatest.
This information can help in planning interventions (eg,
angioplasty, nicardipine infusions).
Day 12Yend of ICU stay TCD can document spasm resolution after treatment or
intervention, sustainability of vessel patency, and infrequent
cases of late or rebound vasospasm development at the end
of the second or into the third week after subarachnoid
hemorrhage. At all specific time intervals, TCD is able to detect
changes in resistance to flow that may indicate increase in
the intracranial pressure and necessitate ventriculostomy.
Suspected brain Increased intracranial TCD can rule out cerebral circulatory arrest if positive
death pressure, mass effect, diastolic flow is detected at any intracranial pressure values.
herniation TCD can confirm the clinical diagnosis of brain death by
demonstrating complete cerebral circulatory arrest in both
middle cerebral arteries and the basilar artery. TCD offers
serial noninvasive assessments and can minimize the
number of nuclear flow studies needed to confirm arrest
of cerebral circulation.
a
Modified with permission from Alexandrov AV, et al; American Society of Neuroimaging Practice Guidelines Committee, J Neuroimaging.13
B 2010 American Society of Neuroimaging. onlinelibrary.wiley.com/doi/10.1111/j.1552-6569.2010.00523.x/full.
increased velocities due to hyperdynamic hypertension-euvolemia or invasively
states. By recording velocity in the MCA with balloon angioplasty or intraar-
and the ipsilateral extracranial ICA, a terial vasodilators. Distal vasospasm
Lindegaard ratio between mean flow can be indirectly diagnosed when focal
velocities (MCA/ICA) can be calculated; pulsatile flow (pulsatility index greater
a ratio greater than 6 indicates severe than 1.2) is detected.24 Similar to a
spasm. Secondary findings, such as rapid Lindegaard ratio, a Soustiel ratio (mean
daily mean flow velocity rise (greater flow velocity of basilar artery/extracranial
than 20% or greater than 65 cm/s) and vertebral artery assessed at the first
early appearance of MCA mean flow cervical level) greater than 3 indi-
velocity of greater than 180 cm/s, are cates severe basilar artery vasospasm
associated with adverse outcomes in after SAH.25
patients with SAH. Early recognition Brain death is a clinical diagnosis
of severe vasospasm can lead to the that can be supported by TCD find-
prompt treatment of vasospasm with ings, given the ability of TCD to detect
Continuum (Minneap Minn) 2016;22(5):1655–1677 www.ContinuumJournal.com 1667
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Ultrasound
KEY POINTS
h Brain death is a clinical cerebral circulatory arrest (Table 13-4). evaluated in three predetermined exam-
diagnosis that can be Increased intracranial pressure causes ination planes: mesencephalic, thalamic,
supported by transcranial increased pulsatility, followed by re- and lateral ventricular (Table 13-5).
Doppler, given the ability duction, elimination, and reversal of The midbrain appears hypoechoic in
of transcranial Doppler to diastolic flow. Finally, a reverberating transcranial sonography and is readily
detect cerebral flow pattern emerges, and, at that point, recognized by its characteristic but-
circulatory arrest. TCD can confirm complete cerebral terfly pattern, surrounded by the hyper-
h The midbrain appears circulatory arrest (Figure 13-9), offering echoic basal cisterns. The substantia
hypoechoic in transcranial a pathophysiologic explanation of clin- nigra appears as a thin hyperechoic
sonography, surrounded ical progression to brain death. TCD has strip with total surface not exceeding
by the hyperechoic basal received a Class A, Level II evidence rat- 0.20 cm2 in normal subjects. In 87% of
cisterns, while the ing for determining cerebral circulatory
substantia nigra appears
patients with Parkinson disease (PD),
arrest/brain death by the American Aca-
as a thin hyperechoic strip the substantia nigra shows increased
demy of Neurology.26 False negatives
with total surface not echogenicity (Figure 13-10) as com-
exist, especially when time has elapsed
exceeding 0.20 cm2 in pared to 12% in controls.28 Hyperecho-
between brain death and TCD examina-
normal subjects. genicity is more pronounced in the side
tion, but specificity remains high (higher
h Increased substantia of the midbrain contralateral to the
than 95%). A recent meta-analysis in-
nigra hyperechogenicity
cluding 22 eligible studies (1671 pa- side of predominance of extrapyramidal
can be detected with symptoms. In a minority of patients
tients total) showed that TCD had a
transcranial parenchymal with PD, around 10%, normal echo-
sonography in
pooled sensitivity and specificity of
90% and 98%, respectively, for the genicity of the substantia nigra is pre-
approximately 90% of
diagnosis of brain death.27 served, a finding that could be because
patients with idiopathic
Parkinson disease.
of a different genetic background or
MOVEMENT DISORDERS secondary parkinsonism.29 Increased
Technologic advances in ultrasound iron deposition and reduction of fer-
have led to improved brain parenchy- ritin levels have been described in
mal imaging that has permitted novel autopsy studies of the substantia nigra
uses of transcranial sonography in neu- of patients with PD; iron is thus be-
rologic disorders. The echogenicity and lieved to bind to alternative proteins
surface of specific brain structures are and result in neurotoxicity locally.30
FIGURE 13-9 Power-motion-mode transcranial Doppler showing reverberating flow in middle cerebral arteries both
in power-motion-mode (red bands corresponding to antegrade flow, blue bands corresponding to
retrograde flow) and spectral displays in a patient with cerebral circulatory arrest.
1668 www.ContinuumJournal.com October 2016
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TABLE 13-5 Standardized Examination Planes and Cerebral Structures to Be Evaluated
in Patients Diagnosed With Movement Disorders
Examination Plane Structure Normal Findings Abnormal Findings
Mesencephalic plane Substantia nigra Echogenicity: weak Size of echoic area 90.2 cm2:
medium hyperechogenicity
Size of echoic area: Size of echoic area 90.25 cm2:
G0.2 cm2 significant hyperechogenicity
Red nucleus Echogenicity: medium Unknown
to significant
Midbrain raphe Echogenicity: medium Reduced echogenicity
to significant (hypoechoic to anechoic)
Thalamic plane Thalamus Echogenicity: hypoechoic Increased echogenicity
to isoechoic (hyperechoic)
Lentiform nucleus Echogenicity: isoechoic Increased echogenicity
(hyperechoic)
Caudate nucleus Echogenicity: isoechoic Increased echogenicity
(hyperechoic)
Third ventricular Age G60 years: G7 mm Age G60 years: 97 mm
diameter
Age 960 years: G10 mm Age 960 years: 910 mm
Lateral ventricular plane Lateral ventricular Age G60 years: G19 mm Age G60 years: 919 mm
diameter
Age 960 years: G22 mm Age 960 years: 922 mm
When extrapyramidal symptoms related with markedly increased risk KEY POINT
become apparent in PD, 60% to 70% for PD development.33 h Substantia nigra
of nigrostriatal neurons have been Neurosonology may provide nonin- hyperechogenicity may
serve as a preclinical
lost. As a consequence, a preclinical vasive information for the differential
marker of idiopathic
diagnosis of PD is critical for the diagnosis of extrapyramidal disorders. parkinsonism.
research and development of neu- Differentiating PD from other neuro-
roprotective therapies. Large-scale degenerative disorders presenting
population screening is not feasible, with parkinsonism, such as multiple
but in relatives of patients with PD, system atrophy, progressive supranu-
who are at higher risk for developing clear palsy, dementia with Lewy bod-
the disease, substantia nigra hyper- ies, and corticobasal degeneration,
echogenicity is present in 45%.31 An- can still be challenging despite re-
other subgroup at risk for PD is markable progress in brain imaging.34
patients with depression; in this group, Definite diagnosis of the aforemen-
an increased incidence of substantia tioned disorders necessitates autopsy,
nigra hyperechogenicity has been de- and, in many instances, clinical diag-
scribed.32 In a cohort of 1847 asymp- nosis is proved erroneous by post-
tomatic subjects over 50 years of age, mortem findings. Correct diagnosis is
substantia nigra hyperechogenicity cor- crucial not only for treatment, but
Continuum (Minneap Minn) 2016;22(5):1655–1677 www.ContinuumJournal.com 1669
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Ultrasound
KEY POINTS
h Peripheral nerve
ultrasound may offer
structural information
regarding the underlying
etiology of entrapment
neuropathies.
Ultrasound findings are
complementary to
information offered by
neurophysiologic studies.
h Ultrasonography of a
peripheral nerve
examines five parameters:
(1) cross-sectional area
at certain sites of clinical
interest, (2) variability
of the cross-sectional
area along its course,
(3) echogenicity,
(4) vascularity, and
(5) mobility.
FIGURE 13-10 Transcranial sonography in a patient
with idiopathic Parkinson disease at axial
midbrain plane. Note the butterfly
appearance of midbrain (A, red arrow) and the presence
of mild ipsilateral substantia nigra hyperechogenicity
(B, green asterisk; planimetric measurement of substantia
nigra echoic area: 0.227 cm2 [normal reference value
G0.20 cm2, moderate substantia nigra hyperechogenicity
0.20 cm2 to 0.25 cm2, severe substantia nigra
hyperechogenicity 90.25 cm2]).
also for creating homogenous cohorts PNS that is complementary to electro-
for clinical trials. As a consequence, a physiologic studies. Normal peripheral
great need exists for novel noninva- nerves have a tubular form, with alter-
sive diagnostic methods. Transcranial nating hypoechoic (nerve fibers) and
sonography, in conjunction with clin- hyperechoic (perineurium) zones that
ical characteristics, has demonstrated give the impression of a honeycomb
high sensitivity for the differential pattern (Figure 13-11). Five parame-
diagnosis of movement disorders.35 ters of a peripheral nerve are exam-
Transcranial sonography findings in ex- ined: (1) cross-sectional area (CSA) at
trapyramidal disorders are summarized certain sites of clinical interest, (2) va-
in Table 13-6. riability of the CSA along its course,
(3) echogenicity, (4) vascularity, and
PERIPHERAL NERVOUS SYSTEM (5) mobility.
Ultrasonography of the peripheral
nervous system (PNS) is a noninvasive Entrapment Neuropathies
diagnostic method that is increasingly Peripheral nerve ultrasound may be
being used in clinical practice. It pro- particularly useful in the diagnosis of en-
vides a morphologic evaluation of the trapment neuropathies (Table 13-7).36,37
1670 www.ContinuumJournal.com October 2016
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TABLE 13-6 Ultrasound Findings of Brain Parenchyma in Healthy Individuals and in Those With
Neurodegenerative Disease
Increase Increase of
Substantia Lentiform Caudate of Third Lateral
Nigra Nucleus Nucleus Ventricular Ventricular
Condition Hyperechogenicity Hyperechogenicity Hyperechogenicity Diameter Diameter
Healthy individuals Rare Rare Rare Very rare Rare
960 years old
Idiopathic Almost always Rare Often Never Very rare
Parkinson observed
disease
Multiple system Very rare Almost always Often Never Very rare
atrophy observed
Progressive Rare Almost always Almost always Almost Often
supranuclear palsy always
Corticobasal Almost always Almost always Almost always Never Rare
degeneration observed
Dementia with Almost always Rare Almost always Never Often
Lewy bodies observed
Carpal tunnel syndrome. Carpal within normal values.37 One of the KEY POINT
tunnel syndrome is the entrapment latest applications of neuromuscular h The most common
neuropathy that has been most exten- ultrasound is the preoperative detection ultrasound findings seen
sively studied with ultrasound. The in patients with
of persistent median artery or bifid
symptomatic carpal
most common ultrasound findings de- median nerve that have been reported tunnel syndrome include
tected in patients with symptomatic as causes of atypical carpal tunnel enlarged cross-sectional
carpal tunnel syndrome include: syndrome.38 area of the median nerve
& Enlarged CSA of the median nerve Radial neuropathy. The most com- proximal to the edge of
proximal to the edge of the mon causes of compressive neuropa- the flexor retinaculum,
flexor retinaculum thy of the deep motor branch of the increased wrist to forearm
& Increased wrist to forearm radial nerve are repetitive overuse of the swelling ratio,
swelling ratio forearm (repetitive pronation-supination hypoechogenicity and
disturbed fascicular echo
& Hypoechogenicity and disturbed or flexion-extension). The most com-
structure, reduced
fascicular echo structure mon ultrasound findings are CSA en- slippage of the nerve after
& Reduced slippage of the nerve largement of the posterior inferior finger flexion, and
after finger flexion nerve at the proximal portion of increased vascularity.
& Increased vascularity the compression site, hyperemia of
A diagnostic algorithm that takes the nerve, and echo difference of the
into consideration CSA of the median dorsal extensor muscles caused by
nerve at the wrist and the forearm denervation.37,39
presents similar sensitivity and speci- Fibular neuropathy. Entrapment
ficity to electrophysiologic studies.36 neuropathy of the common fibular
However, in some cases of severe and nerve is usually located at the fibular
advanced carpal tunnel syndrome re- head region. Although reduction of mo-
sulting in nerve atrophy, CSA could be tor conduction velocity and presence
Continuum (Minneap Minn) 2016;22(5):1655–1677 www.ContinuumJournal.com 1671
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Ultrasound
FIGURE 13-11 Median nerve ultrasound. A, Peripheral nerve ultrasound depicts a transverse view of a normal median nerve
(circled with dotted lines) at the wrist. The nerve appears with normal echotexture exhibiting a honeycomb pattern
and with a normal cross-sectional area (CSA) of 0.07 cm2. B, The same nerve is depicted in sagittal
view, exhibiting no signs of entrapment (dotted lines). C, Peripheral nerve ultrasound depicting a transverse view of the wrist of a
patient with carpal tunnel syndrome. The median nerve appears enlarged (circled with dotted lines) (CSA = 0.18 cm2, normal
value G0.11 cm2) and the echotexture has changed to hypoechoic with loss of the regular honeycomb pattern. D, Sagittal view
of the same nerve shows the structural entrapment and consecutive enlargement shortly before the constriction (dotted lines).
of conduction block are frequent elec- method for evaluating cervical root
trophysiologic findings, neuromus- lesions. CSA of the clinically affected
cular ultrasound may add useful cervical nerve roots are increased
diagnostic data concerning the etiology compared to the unaffected sides and
of entrapment: intraneural ganglia, correlate with symptom duration.41
ganglion cyst, neurofibroma, or hema-
toma. Common pathologic ultrasound Brachial Plexopathies
findings include increased CSA of the Ultrasound imaging of the brachial
nerve at the fibular head or proximally plexus is routinely used to perform
and increased fibular to popliteal fossa nerve block, but diagnostic applica-
swelling ratio.37,40 tions are growing fast. High specificity
Cervical radiculopathy. Although and fair sensitivity of ultrasound in
MRI remains the gold standard for brachial plexus pathology has been
diagnosing cervical radiculopathy, so- reported, especially for the detection
nography provides an alternative of mass lesions.42 Ultrasound may
1672 www.ContinuumJournal.com October 2016
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
TABLE 13-7 Overview of the Most Common Ultrasound Findings in
Entrapment Neuropathiesa
Entrapment Neuropathy Ultrasound Findings
Carpal tunnel syndrome Cross-sectional area (CSA) 90.11 cm2
Wrist to forearm ratio 91.4
Reduced echogenicity
Increased vascularity
Reduced mobility
Cubital tunnel syndrome CSA 90.09 cm2
Elbow to upper arm ratio 91.4
Reduced echogenicity
Increased echogenicity of epineurium
Luxation/subluxation
Radial nerve compression CSA 90.06 cm2
Reduced echogenicity
Fibular nerve compression CSA 90.12 cm2
Reduced echogenicity
Popliteal fossa to fibular head ratio 91.4
Cervical radiculopathy Side-to-side difference ratio 91.5
a
Modified with permission from Kerasnoudis A, Tsivgoulis G, J Neuroimaging.37 B 2015 American
Society of Neuroimaging. onlinelibrary.wiley.com/doi/10.1111/jon.12261/abstract.
reveal rupture, swelling, or loss of the nerve conduction studies of the phrenic
internal texture of the brachial plexus nerve.44
in traumatic lesions and may assist in
the diagnosis of radiation plexitis, Inflammatory Polyneuropathies
tumor invasion (Pancoast tumor), neu- PNS ultrasound may also offer diag-
rogenic tumors, and Parsonage-Turner nostic information in patients with in-
(also known as neuralgic amyotrophy flammatory polyneuropathies.37 The
or brachial neuritis) and thoracic out- main applications of neurosonology
let syndromes.43 in the diagnostic evaluation of inflam-
matory polyneuropathies are summa-
Phrenic Neuropathies rized below.
Besides enhancing the accuracy of Chronic inflammatory demyelinat-
needle positioning during EMG of ing polyradiculoneuropathy. Brachial
the diaphragm, ultrasound may reveal plexus hypertrophy and multifocal
atrophy (decrease of absolute thickness) peripheral nerve hypertrophy can be
or decreased contractility (decrease in seen on ultrasound images in patients
thickening ratio at maximal inspiration) with chronic inflammatory demyelin-
of the diaphragm, providing additional ating polyradiculoneuropathy (CIDP),
information to diaphragmatic EMG and probably due to recurrent episodes
Continuum (Minneap Minn) 2016;22(5):1655–1677 www.ContinuumJournal.com 1673
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Ultrasound
of demyelination and remyelination detecting focal nerve enlargement in
that lead to the classic onion-bulb his- MMN and differentiating this condition
tologic appearance of the nerves. In- from amyotrophic lateral sclerosis.48
creased intranerve CSA variability in Peripheral nerve involvement is a
several peripheral nerves has also been common complication of systemic
reported. The degree of correlation vasculitis and presents as a painful
between sonographic and electrophys- sensorimotor polyneuropathy affect-
iologic findings in CIDP still remains ing primarily the lower limbs or as a
unclear, and neither study correlates mononeuritis multiplex. Diffuse thick-
sufficiently with functional disability.45 ening of peripheral nerves, primarily
Nerve ultrasound scores have been de- of the lower limbs, and reduction of
veloped to distinguish CIDP of sub- nerve diameter after corticosteroid
acute or progressive onset from therapy have been described using
Guillain-Barré syndrome (GBS). A sum ultrasound.49 Abnormal ultrasound
score of 2 points or more on the findings have been reported in pa-
Bochum ultrasound score has sensi- tients with paraproteinemia, and path-
tivity of 80% and specificity of 100% ologic values of both of the nerve CSAs
for the distinction of subacute CIDP in various peripheral nerves have been
from GBS. The score is more sensitive found in patients with antiYmyelin-
than both classic electrophysiologic associated glycoprotein antibodies
and clinical parameters in diagnosing (MAG) polyneuropathy.50
the early onset of CIDP.46 In addition,
a distinction of CIDP from multifo- CONCLUSION
cal motor neuropathy (MMN) or TCD and cervical duplex ultrasonogra-
multifocal acquired demyelinating phy are two easily repeatable nonin-
sensory and motor neuropathy vasive diagnostic tests that can be
(MADSAM) can be made with the performed at the bedside and may
Bochum ultrasound score. provide hemodynamic information in
Guillain-Barré syndrome. Both pe- real time. Both tests broaden the
ripheral nerve and cervical root pa- abilities of stroke physicians to rapidly
thology during the early stage of GBS evaluate patients with stroke, deter-
have been described with ultrasonog- mine the likely mechanism of stroke,
raphy, but nerve ultrasound findings and decide on acute reperfusion and
seem to show no significant correla- secondary prevention therapies. Tran-
tion to electrophysiologic findings or scranial parenchymal sonography has
functional disability in patients with recently been developed as a valuable
GBS.47 However, increased CSF protein supplementary tool in the diagnosis
and reduced compound muscle action and differential diagnosis of move-
potential amplitudes in motor conduc- ment disorders by providing reliable
tion studies appear to predict both the structural information on the substantia
functional outcome and the develop- nigra, basal ganglia, and ventricular
ment of pathologic nerve ultrasound system. Peripheral nerve ultrasound is
changes in GBS.37 a noninvasive and readily available
Other neuropathies. Nerve ultra- modality that may offer structural in-
sound abnormalities in MMN appear as formation regarding the underlying
a multifocal pattern of nerve enlarge- etiology of entrapment neuropa-
ment at sites with or without clinical or thies that is complementary to the
electrophysiologic abnormalities. Nerve findings offered by neurophysio-
ultrasound is a useful method for logic studies.
1674 www.ContinuumJournal.com October 2016
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
REFERENCES 11. Tsivgoulis G, Heliopoulos I, Vadikolias K,
1. Rundek T. Beyond percent stenosis: carotid et al. Teaching NeuroImages: ultrasound
plaque surface irregularity and risk of stroke. findings in giant-cell arteritis. Neurology
Int J Stroke 2007;2(3):169Y171. doi:10.1111/ 2010;75(16):e67Ye68. doi:10.1212/
j.1747-4949.2007.00135.x. WNL.0b013e3181f881e9.
2. Grant EG, Benson CB, Moneta GL, et al. 12. Arida A, Kyprianou M, Kanakis M,
Carotid artery stenosis: gray-scale and Sfikakis PP. The diagnostic value of
Doppler US diagnosisVSociety of Radiologists ultrasonography-derived edema of the
in Ultrasound Consensus Conference. temporal artery wall in giant cell arteritis:
Radiology 2003;229(2):340Y346. doi:10.1148/ a second meta-analysis. BMC Musculoskelet
radiol.2292030516. Disord 2010;11:44. doi:10.1186/
3. Saqqur M, Sharma VK, Tsivgoulis G, et al. 1471-2474-11-44.
Real-time hemodynamic assessment of 13. Alexandrov AV, Sloan MA, Tegeler CH, et al;
downstream effects of intracranial stenoses American Society of Neuroimaging
in patients with orthostatic hypoperfusion Practice Guidelines Committee. Practice
syndrome. Cerebrovasc Dis 2010;30(4): standards for transcranial Doppler (TCD)
355Y361. doi:10.1159/000319567. ultrasound. Part II. Clinical indications and
4. Pascual-Leone A, Anderson DC, Larson DA. expected outcomes. J Neuroimaging
Volume therapy in orthostatic transient 2012;22(3):215Y224. doi:10.1111/
ischemic attacks. Stroke 1989;20(9):1267Y1270. j.1552-6569.2010.00523.x.
doi:10.1161/01.STR.20.9.1267.
14. Tsivgoulis G, Sharma VK, Lao AY, et al.
5. King A, Markus HS. Doppler embolic signals Validation of transcranial Doppler with
in cerebrovascular disease and prediction of computed tomography angiography in
stroke risk: a systematic review and meta-analysis. acute cerebral ischemia. Stroke
Stroke 2009;40(12):3711Y3717. doi:10.1161/ 2007;38(4):1245Y1249. doi:10.1161/
STROKEAHA.109.563056. 01.STR.0000259712.64772.85.
6. Brott TG, Halperin JL, Abbara S, et al. 2011 15. Molina CA, Alexandrov AV, Demchuk AM,
ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/ et al. Improving the predictive
SAIP/SCAI/SIR/SNIS/SVM/SVS guideline on the accuracy of recanalization on stroke
management of patients with extracranial outcome in patients treated with tissue
carotid and vertebral artery disease. Stroke plasminogen activator. Stroke
2011;42(8):e464Ye540. doi:10.1161/ 2004;35(1):151Y156. doi:10.1161/
STR.0b013e3182112cc2. 01.STR.0000106485.04500.
7. Bartels E, Fuchs HH, Flügel KA. Duplex 16. Alexandrov AV, Burgin WS, Demchuk AM,
ultrasonography of vertebral arteries: et al. Speed of intracranial clot lysis with
examination, technique, normal values, intravenous tissue plasminogen activator
and clinical applications. Angiology therapy: sonographic classification and
1992;43(3 pt 1):169Y180. doi:10.1177/ short-term improvement. Circulation
000331979204300301. 2001;103(24):2897Y2902. doi:10.1161/
01.CIR.103.24.2897.
8. Sturzenegger M, Mattle HP, Rivoir A,
Baumgartner RW. Ultrasound 17. Tsivgoulis G, Ribo M, Rubiera M, et al.
findings in carotid artery dissection: Real-time validation of transcranial Doppler
analysis of 43 patients. Neurology criteria in assessing recanalization during
1995;45(4):691Y698. doi:10.1212/ intra-arterial procedures for acute ischemic
WNL.45.4.691. stroke: an international, multicenter study.
Stroke 2013;44(2):394Y400. doi:10.1161/
9. Nebelsieck J, Sengelhoff C, Nassenstein I,
STROKEAHA.112.675074.
et al. Sensitivity of neurovascular
ultrasound for the detection of 18. Alexandrov AV, Nguyen HT, Rubiera M,
spontaneous cervical artery dissection. J Clin et al. Prevalence and risk factors associated
Neurosci 2009;16(1):79Y82. doi:10.1016/ with reversed Robin Hood syndrome in
j.jocn.2008.04.005. acute ischemic stroke. Stroke
2009;40(8):2738Y2742. doi:10.1161/
10. Schinkel AF, van den Oord SC, van der
STROKEAHA.109.547950.
Steen AF, et al. Utility of contrast-enhanced
ultrasound for the assessment of the 19. Silvestrini M, Vernieri F, Pasqualetti P, et al.
carotid artery wall in patients with Takayasu Impaired cerebral vasoreactivity and risk of
or giant cell arteritis. Eur Heart J stroke in patients with asymptomatic carotid
Cardiovasc Imaging 2014;15(5):541Y546. artery stenosis. JAMA 2000;283(16):2122Y2127.
doi:10.1093/ehjci/jet243. doi:10.1001/jama.283.16.2122.
Continuum (Minneap Minn) 2016;22(5):1655–1677 www.ContinuumJournal.com 1675
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
Ultrasound
20. Tsivgoulis G, Krogias C, Georgiadis GS, et al. parkinsonian syndromes. Neurology
Safety of early endarterectomy in patients 2003;60(1):74Y77. doi:10.1212/WNL.60.1.74.
with symptomatic carotid artery stenosis: an
30. Riederer P, Sofic E, Rausch WD, et al.
international multicenter study. Eur J Neurol
Transition metals, ferritin, glutathione, and
2014;21(10):1251Y1257, e75Ye76.
ascorbin acid in parkinsonian brains. J
doi:10.1111/ene.12461.
Neurochem 1989;52(2):515Y520.
21. Lao AY, Sharma VK, Tsivgoulis G, et al. doi:10.1111/j.1471-4159.1989.tb09150.x.
Detection of right-to-left shunts: comparison
31. Ruprecht-Dörfler P, Berg D, Tucha O, et al.
between the International Consensus and
Echogenicity of the substantia nigra in
Spencer Logarithmic Scale criteria.
relatives of patients with sporadic Parkinson’s
J Neuroimaging 2008;18(4):402Y406.
disease. Neuroimage 2003;18(2):416Y422.
doi:10.1111/j.1552-6569.2007.00218.x.
doi:10.1016/S1053-8119(02)00035-6.
22. Tsivgoulis G, Kerasnoudis A, Krogias C, et al.
Clopidogrel load for emboli reduction in 32. Schuurman AG, van den Akker M, Ensinck KT,
patients with symptomatic carotid stenosis et al. Increased risk of Parkinson’s disease
undergoing urgent carotid endarterectomy. after depression: a retrospective cohort study.
Stroke 2012;43(7):1957Y1960. doi:10.1161/ Neurology 2002;58(10):1501Y1504.
STROKEAHA.112.657916. doi:10.1212/WNL.58.10.1501.
23. Adams RJ, Brambilla D; Optimizing Primary 33. Berg D, Seppi K, Behnke S, et al. Enlarged
Stroke Prevention in Sickle Cell Anemia substantia nigra hyperechogenicity and risk
(STOP 2) Trial Investigators. Discontinuing for Parkinson disease: a 37-month 3-center
prophylactic transfusions used to prevent study of 1847 older persons. Arch Neurol
stroke in sickle cell disease. N Engl J Med 2011;68(7):932Y937. doi:10.1001/
2005;353(26):2769Y2778. doi:10.1056/ archneurol.2011.141.
NEJMoa050460. 34. Respondek G, Roeber S, Kretzschmar H, et al.
24. Mizuno M, Nakajima S, Sampei T, et al. Serial Accuracy of the National Institute for
transcranial Doppler flow velocity and cerebral Neurological Disorders and Stroke/Society
blood flow measurements for evaluation of for Progressive Supranuclear Palsy and
cerebral vasospasm after subarachnoid neuroprotection and natural history in
hemorrhage. Neurol Med Chir (Tokyo) Parkinson plus syndromes criteria for the
1994;34(3):164Y171. doi:10.2176/nmc.34.164. diagnosis of progressive supranuclear palsy.
Mov Disord 2013;28(4):504Y509. doi:10.1002/
25. Soustiel JF, Shik V, Shreiber R, et al. Basilar
mds.25327.
vasospasm diagnosis: investigation of a
modified ‘‘Lindegaard Index’’ based on imaging 35. Busse K, Heilmann R, Kleinschmidt S,
studies and blood velocity measurements of the et al. Value of combined midbrain
basilar artery. Stroke 2002;33(1):72Y77. sonography, olfactory and motor function
doi:10.1161/hs0102.100484. assessment in the differential diagnosis of
early Parkinson’s disease. J Neurol Neurosurg
26. Sloan MA, Alexandrov AV, Tegeler CH, et al.
Psychiatry 2012;83(4):441Y447. doi:10.1136/
Assessment: transcranial Doppler
jnnp-2011-301719.
ultrasonography: report of the Therapeutics
and Technology Assessment Subcommittee of 36. Deniz FE, Oksüz E, Sarikaya B, et al.
the American Academy of Neurology. Comparison of the diagnostic utility of
Neurology 2004;62(9):1468Y1481. doi:10.1212/ electromyography, ultrasonography,
WNL.62.9.1468. computed tomography, magnetic resonance
imaging in idiopathic carpal tunnel
27. Chang JJ, Tsivgoulis G, Katsanos AH, et al. syndrome determined by clinical findings.
Diagnostic accuracy of transcranial Doppler Neurosurgery 2012;70(3):610Y616.
for brain death confirmation: systematic doi:10.1227/NEU.0b013e318233868f.
review and meta-analysis. AJNR Am J
Neuroradiol 2016;37(3):408Y414. 37. Kerasnoudis A, Tsivgoulis G. Nerve
doi:10.3174/ajnr.A4548. ultrasound in peripheral neuropathies: a
review. J Neuroimaging 2015;25(4):528Y538.
28. Vlaar AM, Bouwmans A, Mess WH, et al. doi:10.1111/jon.12261.
Transcranial duplex in the differential diagnosis
of parkinsonian syndromes: a systematic 38. Walker FO, Cartwright MS, Blocker JN, et al.
review. J Neurol 2009;256(4):530Y538. Prevalence of bifid median nerves and
doi:10.1007/s00415-009-0143-8. persistent median arteries and their association
with carpal tunnel syndrome in a sample of
29. Walter U, Niehaus L, Probst T, et al. Brain Latino poultry processors and other manual
parenchyma sonography discriminates workers. Muscle Nerve 2013;48(4):539Y544.
Parkinson’s disease and atypical doi:10.1002/mus.23797.
1676 www.ContinuumJournal.com October 2016
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
39. Djurdjevic T, Loizides A, Löscher W, et al. electrophysiological and clinical findings
High resolution ultrasound in posterior in chronic inflammatory demyelinating
interosseous nerve syndrome. Muscle Nerve polyneuropathy. J Neuroimaging
2014;49(1):35Y39. doi:10.1002/mus.23867. 2015;25(2):207Y216. doi:10.1111/
jon.12079.
40. Visser LH, Hens V, Soethout M, et al.
Diagnostic value of high-resolution 46. Kerasnoudis A, Pitarokoili K, Behrendt V,
sonography in common fibular neuropathy et al. Bochum ultrasound score versus
at the fibular head. Muscle Nerve clinical and electrophysiological parameters
2013;48(2):171Y178. doi:10.1002/mus.23729. in distinguishing acute-onset chronic from
41. Kim E, Yoon JS, Kang HJ. Ultrasonographic acute inflammatory demyelinating
cross-sectional area of spinal nerve roots in polyneuropathy. Muscle Nerve 2015;
cervical radiculopathy: a pilot study. Am J 51(6):846Y852. doi:10.1002/mus.24484.
Phys Med Rehabil 2015;94(2):159Y164. 47. Grimm A, Décard BF, Axer H.
doi:10.1097/PHM.0000000000000212. Ultrasonography of the peripheral nervous
42. Tagliafico A, Succio G, Serafini G, Martinoli C. system in the early stage of Guillain-Barré
Diagnostic performance of ultrasound syndrome. J Peripher Nerv Syst 2014;
in patients with suspected brachial plexus 19(3):234Y241. doi:10.1111/jns.12091.
lesions in adults: a multicenter retrospective 48. Grimm A, Décard BF, Athanasopoulou I,
study with MRI, surgical findings and clinical et al. Nerve ultrasound for differentiation
follow-up as reference standard. Skeletal between amyotrophic lateral sclerosis and
Radiol 2013;42(3):371Y376. multifocal motor neuropathy. J Neurol
43. Lapegue F, Faruch-Bilfeld M, Demondion X, 2015;262(4):870Y880. doi:10.1007/
et al. Ultrasonography of the brachial s00415-015-7648-0.
plexus, normal appearance and practical
49. Grimm A, Décard BF, Bischof A, Axer H.
applications. Diagn Interv Imaging Ultrasound of the peripheral nerves in
2014;95(3):259Y275. systemic vasculitic neuropathies. J Neurol
44. Boon AJ, Sekiguchi H, Harper CJ, et al. Sci 2014;347(1Y2):44Y49. doi:10.1016/
Sensitivity and specificity of diagnostic j.jns.2014.09.017.
ultrasound in the diagnosis of phrenic
50. Lucchetta M, Padua L, Granata G, et al. Nerve
neuropathy. Neurology 2014;83(14):
ultrasound findings in neuropathy associated
1264Y1270.
with anti-myelin-associated glycoprotein
45. Kerasnoudis A, Pitarokoili K, Behrendt V, antibodies. Eur J Neurol 2015;22(1):193Y1202.
et al. Correlation of nerve ultrasound, doi:10.1111/ene.12554.
Continuum (Minneap Minn) 2016;22(5):1655–1677 www.ContinuumJournal.com 1677
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
You might also like
- Shock Cheat SheetDocument2 pagesShock Cheat SheetCindia LaiNo ratings yet
- Pocket Reference For ECGs Made Easy 5th EditionDocument133 pagesPocket Reference For ECGs Made Easy 5th EditionSylvia Loong100% (2)
- 2018 Book PrimaryAngioplastyDocument339 pages2018 Book PrimaryAngioplastyRami El-Mokdad100% (2)
- Heart Failure - 2022Document106 pagesHeart Failure - 2022Rana Khaled AwwadNo ratings yet
- Cardiac Cycle JVPDocument70 pagesCardiac Cycle JVPAstrid PramudyaaNo ratings yet
- Atlas Of: Human Body Ultrasound ScanningDocument575 pagesAtlas Of: Human Body Ultrasound ScanningGARY WILLIAMS CORTEZ PEREZNo ratings yet
- Fontan Operation: DR Hussain BuxDocument62 pagesFontan Operation: DR Hussain BuxMujeeb Ur RehmanNo ratings yet
- VExUS Ultrasound Score Protocol PDFDocument1 pageVExUS Ultrasound Score Protocol PDFKarla HernandezNo ratings yet
- HEARTS Hypertension Clinical Pathway Editable - ENGDocument1 pageHEARTS Hypertension Clinical Pathway Editable - ENGSIANY FIORELLA CHAVEZ MORANNo ratings yet
- Esophagus and StomachDocument33 pagesEsophagus and StomachIrfan Falah100% (1)
- Hemodynamic Monitoring and Support - CCM - 2021Document13 pagesHemodynamic Monitoring and Support - CCM - 2021AlexisBallén100% (3)
- Pulmonary EmbolismDocument23 pagesPulmonary EmbolismBianca Dizon0% (1)
- Diagnostic Ultrasonography in Neurology.15Document40 pagesDiagnostic Ultrasonography in Neurology.15BALEWNo ratings yet
- Role of High Resolution Ultrasound in Assessment oDocument16 pagesRole of High Resolution Ultrasound in Assessment oilham Maulana ArifNo ratings yet
- Point of Care NHJMDocument9 pagesPoint of Care NHJMFernanda Araújo AvendanhaNo ratings yet
- Koziarz 2019Document11 pagesKoziarz 2019Thiago DiasNo ratings yet
- Point-Of-care Ultrasonography N Engl J Med 3648749Document10 pagesPoint-Of-care Ultrasonography N Engl J Med 3648749Andreas Natan100% (1)
- Clinical Neurology and Neurosurgery: SciencedirectDocument15 pagesClinical Neurology and Neurosurgery: SciencedirectPedroNo ratings yet
- Medical Ultrasound - WikipediaDocument30 pagesMedical Ultrasound - WikipedianibNo ratings yet
- Fsurg 10 1277997Document3 pagesFsurg 10 1277997Abhilash VemulaNo ratings yet
- Role of Ultrasound Versus Magnetic Resonance Imaging in Evaluation of Non-Osseous Disorders Causing Wrist PainDocument7 pagesRole of Ultrasound Versus Magnetic Resonance Imaging in Evaluation of Non-Osseous Disorders Causing Wrist Painmariatul khiftiyahNo ratings yet
- 1 s2.0 S2214854X20300224 MainDocument10 pages1 s2.0 S2214854X20300224 MainPhan Tấn TàiNo ratings yet
- Forensic RadiologyDocument12 pagesForensic RadiologywendellNo ratings yet
- Basics of Point-Of-Care Lung UltrasonographyDocument6 pagesBasics of Point-Of-Care Lung UltrasonographyHilma BermudezNo ratings yet
- How To Interpret An Echocardiography Report (For The Non-Imager) ?Document13 pagesHow To Interpret An Echocardiography Report (For The Non-Imager) ?Brigitte Fani FlorenciaNo ratings yet
- Alexandrov2019 PDFDocument10 pagesAlexandrov2019 PDFSyed Shabbir HaiderNo ratings yet
- Ultrasonography Report PDFDocument3 pagesUltrasonography Report PDFKruthi M LNo ratings yet
- Stroke For DiscutionDocument4 pagesStroke For Discutionrebeca marityNo ratings yet
- Doppler Transcreaneal y Ecografía Del Nervio ÓpticoDocument15 pagesDoppler Transcreaneal y Ecografía Del Nervio ÓpticoBenjamínGalvanNo ratings yet
- Ultrasound in Emergency Medicine: Use of Ocular Ultrasound For The Evaluation of Retinal DetachmentDocument5 pagesUltrasound in Emergency Medicine: Use of Ocular Ultrasound For The Evaluation of Retinal DetachmentZarella Ramírez BorreroNo ratings yet
- Laura C Scholtz Ultrasonography in Neurology ADocument10 pagesLaura C Scholtz Ultrasonography in Neurology AJuliaNo ratings yet
- 1530 Jul 27Document6 pages1530 Jul 27kelvin amahNo ratings yet
- Application of Physics in MedicineDocument9 pagesApplication of Physics in MedicineShreyash PolNo ratings yet
- Comparative Overview of Brain Perfusion Imaging Techniques: 2005 36:e83-E99.) Key Words: Computed TomographyDocument17 pagesComparative Overview of Brain Perfusion Imaging Techniques: 2005 36:e83-E99.) Key Words: Computed TomographyAlaa Naser HunikelNo ratings yet
- Contrast Echocardiography: Current Applications and InnovationsDocument7 pagesContrast Echocardiography: Current Applications and InnovationsIJAR JOURNALNo ratings yet
- Kwon Et Al 2020 Deep Learning Based Algorithm For Detecting Aortic Stenosis Using ElectrocardiographyDocument16 pagesKwon Et Al 2020 Deep Learning Based Algorithm For Detecting Aortic Stenosis Using Electrocardiography施展No ratings yet
- Fneur 14 1138661Document2 pagesFneur 14 1138661ChadiIbrahimNo ratings yet
- Ultrasound of The Hand and Wrist in RheumatologyDocument8 pagesUltrasound of The Hand and Wrist in RheumatologyRaphael SiqueiraNo ratings yet
- Stroke 2002 Zunker 2600 3Document5 pagesStroke 2002 Zunker 2600 3MEDI MEDIKANo ratings yet
- Ultrasonography Diagnosis of Peripheral Nerves: Cases and IllustrationsFrom EverandUltrasonography Diagnosis of Peripheral Nerves: Cases and IllustrationsDingzhang ChenNo ratings yet
- Comparison of Pre Procedural and Real Time Ultrasound Guided Spinal Anesthesia For Traumatic Lower Limb InjuryDocument7 pagesComparison of Pre Procedural and Real Time Ultrasound Guided Spinal Anesthesia For Traumatic Lower Limb InjuryIJAR JOURNALNo ratings yet
- 10.1016@S0140 67361931721 0Document7 pages10.1016@S0140 67361931721 0Oana DrăganNo ratings yet
- 057ac46d06cf PDFDocument16 pages057ac46d06cf PDFDonnet AndresNo ratings yet
- Diagnostic Accuracy of Ultrasonography Verified WiDocument5 pagesDiagnostic Accuracy of Ultrasonography Verified WiIranna HittalamaniNo ratings yet
- Imaging For Neuro-Ophthalmic and Orbital Disease - A ReviewDocument24 pagesImaging For Neuro-Ophthalmic and Orbital Disease - A ReviewMashhoor AlfayezNo ratings yet
- Orthopedic Diagnostic Imaging in Exotic PetsDocument25 pagesOrthopedic Diagnostic Imaging in Exotic PetsHidaNo ratings yet
- Craniectomia 3Document8 pagesCraniectomia 3Vlady78No ratings yet
- Zaidat Et Al 2023 Tesla Trial Rationale Protocol and DesignDocument9 pagesZaidat Et Al 2023 Tesla Trial Rationale Protocol and Designdvkhvbbds7No ratings yet
- Tomasello ContourDocument11 pagesTomasello ContourangelNo ratings yet
- Hou, Et Al., 2021Document9 pagesHou, Et Al., 2021NyomantrianaNo ratings yet
- My Published Paper 6, AnesthesiaDocument5 pagesMy Published Paper 6, Anesthesiamir sahirNo ratings yet
- MRI Monitoring of Pathological Changes in The Spinal Cord in Patients With Multiple SclerosisDocument13 pagesMRI Monitoring of Pathological Changes in The Spinal Cord in Patients With Multiple SclerosisIreneNo ratings yet
- Annals of Medicine and Surgery: SciencedirectDocument7 pagesAnnals of Medicine and Surgery: SciencedirectBagoes AsNo ratings yet
- Current Diagnostic Techniques in Veterinary Surgery PDFDocument2 pagesCurrent Diagnostic Techniques in Veterinary Surgery PDFKirti JamwalNo ratings yet
- CT ScanDocument4 pagesCT ScanPoova RagavanNo ratings yet
- Renal Imaging: Core Curriculum 2019Document14 pagesRenal Imaging: Core Curriculum 2019luis arredondoNo ratings yet
- Echography and Doppler of the BrainFrom EverandEchography and Doppler of the BrainChiara RobbaNo ratings yet
- Non Invasive Tests Appreciation of Diagnostic Procedures For Cardiovascular ProblemsDocument9 pagesNon Invasive Tests Appreciation of Diagnostic Procedures For Cardiovascular ProblemsMark Nel NuñezNo ratings yet
- NIH Public Access: Author ManuscriptDocument26 pagesNIH Public Access: Author Manuscriptchrist_cruzerNo ratings yet
- Whole-Body Diffusion Kurtosis Imaging: Initial Experience On Non-Gaussian Diffusion in Various OrgansDocument7 pagesWhole-Body Diffusion Kurtosis Imaging: Initial Experience On Non-Gaussian Diffusion in Various OrgansAyush JainNo ratings yet
- Iranjradiol 10 140Document8 pagesIranjradiol 10 140Orange PeachNo ratings yet
- Musculoskeletal Ultrasonography in Physical and ReDocument10 pagesMusculoskeletal Ultrasonography in Physical and ReHoussem BejaouiNo ratings yet
- Annotated Bibliography FinalDocument15 pagesAnnotated Bibliography Finaledetrez94No ratings yet
- 4 IndianJAnaesth617581-2226112 - 061101Document6 pages4 IndianJAnaesth617581-2226112 - 061101Mythology KingdomNo ratings yet
- 227 Full PDFDocument3 pages227 Full PDFanon_629352389No ratings yet
- Automatic Measurements of Mitral Annular Plane Systolic Excursion and Velocities To Detect Left Ventricular DysfunctionDocument9 pagesAutomatic Measurements of Mitral Annular Plane Systolic Excursion and Velocities To Detect Left Ventricular DysfunctionMiguelNo ratings yet
- Yang 2014Document4 pagesYang 2014Akmal Niam FirdausiNo ratings yet
- Index PHPDocument14 pagesIndex PHPShreyash Yadav (Nova)No ratings yet
- Endoscopic and Open Release Similarly Safe For The Treatment of Carpal Tunnel Syndrome. A Systematic Review and Meta-AnalysisDocument16 pagesEndoscopic and Open Release Similarly Safe For The Treatment of Carpal Tunnel Syndrome. A Systematic Review and Meta-AnalysisMonika Diaz KristyanindaNo ratings yet
- Hodel, 2015 PDFDocument9 pagesHodel, 2015 PDFOliver BlandyNo ratings yet
- 2017 Results of Endoscopically-Assisted Cubital Tunnel Release Without Using Any Specific InstrumentDocument4 pages2017 Results of Endoscopically-Assisted Cubital Tunnel Release Without Using Any Specific InstrumentDimitris RodriguezNo ratings yet
- 304 FullDocument9 pages304 FullIcicNo ratings yet
- Correlation Seminar On Cardiovascular SystemDocument20 pagesCorrelation Seminar On Cardiovascular Systemnischal neupaneNo ratings yet
- Hypertension Topic DiscussionDocument13 pagesHypertension Topic Discussionapi-665372449No ratings yet
- Машщщл Broad: IndexDocument78 pagesМашщщл Broad: IndexWshineNo ratings yet
- (Clinical Cases Uncovered) - CARDIOLOGY - (2010) - Halaman-202-207Document6 pages(Clinical Cases Uncovered) - CARDIOLOGY - (2010) - Halaman-202-207zizaNo ratings yet
- Fetal Circulation: DR - Santosh ReddyDocument16 pagesFetal Circulation: DR - Santosh Reddydevireddy santoshreddyNo ratings yet
- Heart Failure - ReferatDocument10 pagesHeart Failure - ReferatAlbert ShantoNo ratings yet
- +1 Bio Zoo em Vol 2Document38 pages+1 Bio Zoo em Vol 2Ameena BegumNo ratings yet
- Admitting Conference: Abejo, Jerika D. Bona, Henry JR.Document38 pagesAdmitting Conference: Abejo, Jerika D. Bona, Henry JR.Henry BonaNo ratings yet
- Presentor: DR - Kumar Moderator: DR - VamsidharDocument71 pagesPresentor: DR - Kumar Moderator: DR - VamsidharJayaprakash KuppusamyNo ratings yet
- Original PDF Pathophysiology of Heart Disease A Collaborative 6th Edition PDFDocument41 pagesOriginal PDF Pathophysiology of Heart Disease A Collaborative 6th Edition PDFwilliams.allen717100% (40)
- Levine Sign - Google SearchDocument1 pageLevine Sign - Google SearchMathan KarthikNo ratings yet
- Extrinsic Regulation of The HeartDocument9 pagesExtrinsic Regulation of The Heartkawaiijanai gfNo ratings yet
- Erp 18 0068Document17 pagesErp 18 0068Jose Ignacio Tarton SisimitNo ratings yet
- MedCosmos Surgery - History TakingDocument18 pagesMedCosmos Surgery - History TakingEmmanuel DanielsNo ratings yet
- Cardiovascular Failure, Inotropes and Vasopressors: Oxygen DeliveryDocument4 pagesCardiovascular Failure, Inotropes and Vasopressors: Oxygen DeliveryMarlin Berliannanda TawayNo ratings yet
- Assessment of The Peripheral Vascular SystemDocument3 pagesAssessment of The Peripheral Vascular SystemTrisha Andrea DavaNo ratings yet
- Lymphatic SystemDocument7 pagesLymphatic SystemAsher Eby VargeeseNo ratings yet
- Procedure On Ventricular Septal Defect (VSD) Device ClosureDocument9 pagesProcedure On Ventricular Septal Defect (VSD) Device ClosurejaganjaggiNo ratings yet