You might also like
- The Radiology Handbook: A Pocket Guide to Medical ImagingFrom EverandThe Radiology Handbook: A Pocket Guide to Medical ImagingRating: 3.5 out of 5 stars3.5/5 (8)
- Medcosmos Surgery: Spleen MCQDocument19 pagesMedcosmos Surgery: Spleen MCQSajag GuptaNo ratings yet
- Simposium Papdi 3-Hari 1-5. Ws 1 - Dr. Lita-Untuk Share-2. Dr. LitaDocument46 pagesSimposium Papdi 3-Hari 1-5. Ws 1 - Dr. Lita-Untuk Share-2. Dr. LitaRangga Alam VaneoNo ratings yet
- Chapter38 Assessment and Management of Patients With Rheumatic DisordersDocument38 pagesChapter38 Assessment and Management of Patients With Rheumatic Disordersjericho dinglasanNo ratings yet
- Medcosmos SurgeryDocument85 pagesMedcosmos SurgerySajag GuptaNo ratings yet
- (10920684 - Neurosurgical Focus) Surgical Treatment of Primary Sacral Tumors - Complications Associated With SacrectomyDocument8 pages(10920684 - Neurosurgical Focus) Surgical Treatment of Primary Sacral Tumors - Complications Associated With Sacrectomyfloroiu.ioana.valeriaNo ratings yet
- Abdominal Trauma Diagnosis and ClassificationDocument129 pagesAbdominal Trauma Diagnosis and ClassificationTan DanNo ratings yet
- MedCosmos Surgery - MCQ - General SurgeryDocument167 pagesMedCosmos Surgery - MCQ - General SurgeryEmmanuel DanielsNo ratings yet
- MRI Brain - Neurologist P Ed.VDocument58 pagesMRI Brain - Neurologist P Ed.Vnila choNo ratings yet
- Ksellybelly - MSK I Arthritis RheumDocument4 pagesKsellybelly - MSK I Arthritis RheumTricia Kaye IblanNo ratings yet
- CVS System: Bader Al-Mukhtar - RCSI - SCDocument8 pagesCVS System: Bader Al-Mukhtar - RCSI - SCmuhammadridhwanNo ratings yet
- Lecturer: Dr. Jess Belocura: L-NU - College of MedicineDocument7 pagesLecturer: Dr. Jess Belocura: L-NU - College of MedicineDan Fabros0% (1)
- Pengayaan Koass Ortho - Update 5 VersionDocument122 pagesPengayaan Koass Ortho - Update 5 Versionanon_967171484No ratings yet
- CT VS MriDocument1 pageCT VS MriJulianna ChanNo ratings yet
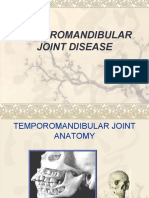
- Temporomandibular Joint DiseaseDocument84 pagesTemporomandibular Joint Diseaseapi-19916399No ratings yet
- Orthopaedics EmergenciesDocument63 pagesOrthopaedics EmergencieszzooooeeeeeeNo ratings yet
- Lecture 6.5 Fracture and Dislocation-dr. Yudha Mathan Sakti, Sp.ot (K) (2020)Document81 pagesLecture 6.5 Fracture and Dislocation-dr. Yudha Mathan Sakti, Sp.ot (K) (2020)stefany huangNo ratings yet
- C/C: One Main Complain (Symptom) +duration+site+cause of The Symptom (FromDocument5 pagesC/C: One Main Complain (Symptom) +duration+site+cause of The Symptom (FromarsohgahNo ratings yet
- Tendinitis Crónica Articulo en InglesDocument6 pagesTendinitis Crónica Articulo en IngleskarolndNo ratings yet
- Kelainan Muskuloskeletal akibat Autoimun & MetabolikDocument75 pagesKelainan Muskuloskeletal akibat Autoimun & MetabolikWita sarumpaetNo ratings yet
- Orthopedic Clerking TemplateDocument4 pagesOrthopedic Clerking TemplateNur Liyana Ahmad ZakiNo ratings yet
- Fractures and Dislocation: ArnadiDocument30 pagesFractures and Dislocation: ArnadiNizai Rama DeswiraNo ratings yet
- (Upgraded) Trauma Multitrauma Kuliah Ummu MalangDocument63 pages(Upgraded) Trauma Multitrauma Kuliah Ummu MalangroroNo ratings yet
- 328 - Management of Polytrauma PatientDocument62 pages328 - Management of Polytrauma PatientvimalNo ratings yet
- Operative Versorgung Von Zentralen Talusfrakturen: Behandlungs-Ergebnisse Von 24 Fällen Im Mittel - Bis Langfristigen VerlaufDocument8 pagesOperative Versorgung Von Zentralen Talusfrakturen: Behandlungs-Ergebnisse Von 24 Fällen Im Mittel - Bis Langfristigen VerlaufFacundo ViláNo ratings yet
- Pocket Medicine, Fifth EditionDocument41 pagesPocket Medicine, Fifth Editionalaa100% (1)
- Paper N SummaryDocument2 pagesPaper N SummaryF ParikhNo ratings yet
- 6 DR NarsimuluDocument67 pages6 DR Narsimulushirish gundalaNo ratings yet
- Abdominal Trauma: Ghidirim GH., Mishin I., Zastavnitsky GH., Vozian MDocument129 pagesAbdominal Trauma: Ghidirim GH., Mishin I., Zastavnitsky GH., Vozian MBedah MalangNo ratings yet
- 2020 Hand and Wrist Pain - Clinical Diagnosis in Physical Medicine and RehabilitationDocument14 pages2020 Hand and Wrist Pain - Clinical Diagnosis in Physical Medicine and RehabilitationLộc Nguyễn ĐìnhNo ratings yet
- 132 2022 4294 Moesm1 EsmDocument2 pages132 2022 4294 Moesm1 EsmFernando Rojas GalleguillosNo ratings yet
- A Clinical Approach To Diagnosing Wrist Pain: Los Angeles, CaliforniaDocument6 pagesA Clinical Approach To Diagnosing Wrist Pain: Los Angeles, CaliforniaOtnil DNo ratings yet
- Comprehensive SummaryDocument37 pagesComprehensive Summaryhrg79qzwc2No ratings yet
- Rheumatology: - Red Flag DiagnosisDocument3 pagesRheumatology: - Red Flag DiagnosisEmilee Joice Rochelle MalutoNo ratings yet
- Dr. Arnadi Fraktur & DislokasiDocument77 pagesDr. Arnadi Fraktur & DislokasiPuji Yunisyah RahayuNo ratings yet
- Piciorul Diabetic CursDocument59 pagesPiciorul Diabetic Cursmichelle misu100% (1)
- Acute Musculoskeletal Problems: ModulesDocument42 pagesAcute Musculoskeletal Problems: ModulesSamuel ChoudhuryNo ratings yet
- Complications of FractureDocument3 pagesComplications of FractureGerardLumNo ratings yet
- TOS, Radial Nerve - Fessh 2023Document46 pagesTOS, Radial Nerve - Fessh 2023Professeur Christian DumontierNo ratings yet
- ProActive Training CaseStudy 5Document8 pagesProActive Training CaseStudy 5danthemanyvrNo ratings yet
- Bone Tumor Seminar: Types & ManagementDocument80 pagesBone Tumor Seminar: Types & ManagementPATHMAPRIYA GANESANNo ratings yet
- Bedah 2 Mei 2019 PDFDocument210 pagesBedah 2 Mei 2019 PDFRinto MangiwaNo ratings yet
- Managing Open FracturesDocument256 pagesManaging Open FracturesZhraaNo ratings yet
- Orthopaedic Emergencies AndreDocument49 pagesOrthopaedic Emergencies AndreLusi MunawarohNo ratings yet
- Osteoid Osteoma: A Diagnosis For Radicular Pain of ExtremitiesDocument7 pagesOsteoid Osteoma: A Diagnosis For Radicular Pain of ExtremitiesadeNo ratings yet
- Malignant Bone TumoursDocument38 pagesMalignant Bone Tumoursgdudex118811No ratings yet
- 9 AbdomenDocument19 pages9 AbdomenfebriyakNo ratings yet
- Tenosynovitis Treatment and DiagnosisDocument32 pagesTenosynovitis Treatment and DiagnosissultantraNo ratings yet
- 2-Sickle Cell Anemia PDFDocument21 pages2-Sickle Cell Anemia PDFJennyu YuNo ratings yet
- Osteomyelitis - Kaye WilkinsDocument50 pagesOsteomyelitis - Kaye WilkinsWindy MentariNo ratings yet
- Case FractureDocument40 pagesCase FractureNidhia BadjakNo ratings yet
- Spinal Cystic SchwannomaDocument3 pagesSpinal Cystic SchwannomahelenNo ratings yet
- Trauma Musculoskeletal - Spine FKK UMJ1Document92 pagesTrauma Musculoskeletal - Spine FKK UMJ1Hendra Hash AwoNo ratings yet
- MBChB Year 5 Surgery: Arterial AneurysmsDocument1 pageMBChB Year 5 Surgery: Arterial AneurysmsJason HarryNo ratings yet
- Rheumatology & Rehabilitation 2018-2019Document57 pagesRheumatology & Rehabilitation 2018-2019Selim TarekNo ratings yet
- Trauma Abdomen GuideDocument19 pagesTrauma Abdomen GuideMerlin MerlianaNo ratings yet
- TrumaDocument13 pagesTrumaShrestha Anjiv100% (1)
- Penanganan Trauma Muskuloskeletal Dan ImobilisasiDocument54 pagesPenanganan Trauma Muskuloskeletal Dan Imobilisasiamir hamzahNo ratings yet
- Adult Hip Pain (Ortho) WadaDocument25 pagesAdult Hip Pain (Ortho) WadaMeno AliNo ratings yet
- Principles of Management of Low Back Pain1Document39 pagesPrinciples of Management of Low Back Pain1Emmanuel DanielsNo ratings yet
- Sterilisation A-Wps OfficeDocument46 pagesSterilisation A-Wps OfficeEmmanuel DanielsNo ratings yet
- Aftermath of Endsars Protest Policy BriefDocument2 pagesAftermath of Endsars Protest Policy BriefEmmanuel DanielsNo ratings yet
- The Skin As An Organ at CBCDocument45 pagesThe Skin As An Organ at CBCEmmanuel DanielsNo ratings yet
- Pathology and Management of Congenital Talipes Equinovarus (Ctev)Document86 pagesPathology and Management of Congenital Talipes Equinovarus (Ctev)Emmanuel DanielsNo ratings yet
- Neurology Samson Corrected PDFDocument27 pagesNeurology Samson Corrected PDFamina67% (3)
- DISCUSS THE USE OF SPLINTS AND TRACTION IN OrthopaedicDocument51 pagesDISCUSS THE USE OF SPLINTS AND TRACTION IN OrthopaedicEmmanuel DanielsNo ratings yet
- NOA Calabar2021 Registration Guide OrthopaedicDocument9 pagesNOA Calabar2021 Registration Guide OrthopaedicEmmanuel DanielsNo ratings yet
- EXAMINATION OF A CASE OF CTEVDocument3 pagesEXAMINATION OF A CASE OF CTEVEmmanuel DanielsNo ratings yet
- Perfect Home TutorDocument9 pagesPerfect Home TutorEmmanuel DanielsNo ratings yet
- Pathology and Management of Congenital Talipes Equinovarus (Ctev)Document86 pagesPathology and Management of Congenital Talipes Equinovarus (Ctev)Emmanuel DanielsNo ratings yet
- Surgery in COVID-19 Pandemic: Risks, Procedures and EthicsDocument49 pagesSurgery in COVID-19 Pandemic: Risks, Procedures and EthicsEmmanuel DanielsNo ratings yet
- SoalDocument4 pagesSoalkurikulum man2wonosoboNo ratings yet
- What Is ReligionDocument15 pagesWhat Is ReligionMary Glou Melo PadilloNo ratings yet
- 6 Fsiqiatria-1524041346Document48 pages6 Fsiqiatria-1524041346მირანდა გიორგაშვილიNo ratings yet
- Json Cache 1Document5 pagesJson Cache 1Emmanuel AmoahNo ratings yet
- Group Assgnmt 8 Rev080515Document9 pagesGroup Assgnmt 8 Rev080515Suhaila NamakuNo ratings yet
- Processing, Handling and Storage of Agricultural Product 2Document6 pagesProcessing, Handling and Storage of Agricultural Product 2LittleagleNo ratings yet
- Ky203817 PSRPT 2022-05-17 14.39.33Document8 pagesKy203817 PSRPT 2022-05-17 14.39.33Thuy AnhNo ratings yet
- Recording of Dying DeclarationDocument6 pagesRecording of Dying DeclarationsarayusindhuNo ratings yet
- Foreign AidDocument4 pagesForeign AidJesse JhangraNo ratings yet
- Si Eft Mandate FormDocument1 pageSi Eft Mandate FormdSolarianNo ratings yet
- 09 Egyptian Architecture PDFDocument107 pages09 Egyptian Architecture PDFIra PecsonNo ratings yet
- Lab Manual 06 CSE 314 Sequence and Communication DiagramDocument6 pagesLab Manual 06 CSE 314 Sequence and Communication DiagramMufizul islam NirobNo ratings yet
- Amelia Wills CV 2021 VDocument4 pagesAmelia Wills CV 2021 Vapi-446566858No ratings yet
- OUM Human Anatomy Final Exam QuestionsDocument5 pagesOUM Human Anatomy Final Exam QuestionsAnandNo ratings yet
- 6 - 2010 Chapter 5 - Contrasting Cultural ValuesDocument39 pages6 - 2010 Chapter 5 - Contrasting Cultural ValuesHari KrishnaNo ratings yet
- 7) Set 3 Bi PT3 (Answer) PDFDocument4 pages7) Set 3 Bi PT3 (Answer) PDFTing ShiangNo ratings yet
- Abnormal Psychology Unit IDocument14 pagesAbnormal Psychology Unit IMahadevan K V100% (1)
- The Merchant of Venice QuestionsDocument9 pagesThe Merchant of Venice QuestionsHaranath Babu50% (4)
- Harsheen Kaur BhasinDocument20 pagesHarsheen Kaur Bhasincalvin kleinNo ratings yet
- Pathways Rw1 2e U7 TestDocument9 pagesPathways Rw1 2e U7 TestGrace Ann AbanteNo ratings yet
- Make Money OnlineDocument9 pagesMake Money OnlineTimiNo ratings yet
- Macroeconomics QuestionnaireDocument5 pagesMacroeconomics Questionnairevikrant vardhanNo ratings yet
- Weekly Capital Market Report Week Ending 22.07.2022 2022-07-22Document2 pagesWeekly Capital Market Report Week Ending 22.07.2022 2022-07-22Fuaad DodooNo ratings yet
- Evosys Fixed Scope Offering For Oracle Fusion Procurement Cloud ServiceDocument12 pagesEvosys Fixed Scope Offering For Oracle Fusion Procurement Cloud ServiceMunir AhmedNo ratings yet
- Thesis Chapter 123Document15 pagesThesis Chapter 123Chesca Mae PenalosaNo ratings yet
- Development Plan-Part IV, 2022-2023Document3 pagesDevelopment Plan-Part IV, 2022-2023Divina bentayao100% (5)
- Perlman Janice, The Myth of Marginality RevisitDocument36 pagesPerlman Janice, The Myth of Marginality RevisitLuisa F. RodriguezNo ratings yet
- Review of Esu Yoruba God Power and The IDocument7 pagesReview of Esu Yoruba God Power and The IBoris MilovicNo ratings yet
- Landman Training ManualDocument34 pagesLandman Training Manualflashanon100% (2)
- PH.D Scholars UGCDocument25 pagesPH.D Scholars UGCUsha MurthyNo ratings yet