You might also like
- Understanding Periodontal Diseases: Assessment and Diagnostic Procedures in PracticeFrom EverandUnderstanding Periodontal Diseases: Assessment and Diagnostic Procedures in PracticeNo ratings yet
- Epidemiology of Periodontal DiseasesDocument14 pagesEpidemiology of Periodontal DiseasesFrancisca DinamarcaNo ratings yet
- Global epidemiology of periodontal diseaseDocument16 pagesGlobal epidemiology of periodontal diseaseBrenda Carolina Pattigno ForeroNo ratings yet
- Epidemiology of Periodontal DiseasesDocument14 pagesEpidemiology of Periodontal DiseasescynjesNo ratings yet
- Periodontitis Increases The Risk of Respiratory Disease Mortality in OlderDocument5 pagesPeriodontitis Increases The Risk of Respiratory Disease Mortality in OlderJavier Ramos GascaNo ratings yet
- The Clinical Course of Chronic Periodontitis 2Document8 pagesThe Clinical Course of Chronic Periodontitis 2Iris PavičićNo ratings yet
- Obesity and Oral Health - Is There An Association?: Collegium Antropologicum September 2012Document6 pagesObesity and Oral Health - Is There An Association?: Collegium Antropologicum September 2012Nicolas YoungNo ratings yet
- Prpic2012 PDFDocument6 pagesPrpic2012 PDFNicolas YoungNo ratings yet
- Obesity Linked to Poor Dental HealthDocument6 pagesObesity Linked to Poor Dental HealthNicolas YoungNo ratings yet
- Obesity Linked to Poor Dental HealthDocument6 pagesObesity Linked to Poor Dental HealthNicolas YoungNo ratings yet
- InTech-Epidemiology and Risk Factors of Periodontal DiseaseDocument18 pagesInTech-Epidemiology and Risk Factors of Periodontal DiseaseTrefina PranaNo ratings yet
- Billings Et Al-2018-Journal of Clinical PeriodontologyDocument19 pagesBillings Et Al-2018-Journal of Clinical PeriodontologyCristian CulcitchiNo ratings yet
- Technical Aspects of Treatment in Relation To Treatment OutcomeDocument14 pagesTechnical Aspects of Treatment in Relation To Treatment OutcomekochikaghochiNo ratings yet
- Kinane - Periodontitis Modified by Systemic FactorsDocument10 pagesKinane - Periodontitis Modified by Systemic FactorsSebastián Payero GutiérrezNo ratings yet
- CDH Mar14 3309-Zenthà Fer Pp27-31 3Document5 pagesCDH Mar14 3309-Zenthà Fer Pp27-31 3Stevie FebriliaNo ratings yet
- Johanssen ReviewDocument16 pagesJohanssen Reviewsidra malikNo ratings yet
- Ajwani 2003Document9 pagesAjwani 2003SRINIVASAN NARASIMHANNo ratings yet
- Association Between Asthma and Periodontal DiseaseDocument20 pagesAssociation Between Asthma and Periodontal DiseaseSheila ParreirasNo ratings yet
- Risk Factors For Periodontal DiseaseDocument37 pagesRisk Factors For Periodontal DiseaseBelee Vera AcuñaNo ratings yet
- Di Iorio - SR World Workshop 08.01.18Document62 pagesDi Iorio - SR World Workshop 08.01.18aziz alsohailNo ratings yet
- Association Between Periodontal Health andDocument7 pagesAssociation Between Periodontal Health andTran DuongNo ratings yet
- Journal of Periodontology - 2018 - Needleman - Mean Annual Attachment Bone Level and Tooth Loss A Systematic ReviewDocument20 pagesJournal of Periodontology - 2018 - Needleman - Mean Annual Attachment Bone Level and Tooth Loss A Systematic ReviewMonica MartínezNo ratings yet
- His To Pathological Features ofDocument10 pagesHis To Pathological Features ofEdric DjiemeshaNo ratings yet
- Boutiou2021 Article HereditaryGingivalFibromatosisDocument9 pagesBoutiou2021 Article HereditaryGingivalFibromatosisRoxana OneaNo ratings yet
- JCT 2013102511342874Document8 pagesJCT 2013102511342874RiestaKierantiNo ratings yet
- Features of The Course of Generalized Periodontitis in Patients With Chronic Obstructive Pulmonary BronchitisDocument4 pagesFeatures of The Course of Generalized Periodontitis in Patients With Chronic Obstructive Pulmonary BronchitisAcademic JournalNo ratings yet
- Polak Et Al-2015-Journal of Clinical Periodontology PDFDocument13 pagesPolak Et Al-2015-Journal of Clinical Periodontology PDFChristine HacheNo ratings yet
- MXX 006Document10 pagesMXX 006badria bawazirNo ratings yet
- Periodontal Risk Assessment, Diagnosis and Treatment PlanningDocument22 pagesPeriodontal Risk Assessment, Diagnosis and Treatment PlanningHenry E. CoaquiraNo ratings yet
- Periodontitis Associated with Respiratory DiseaseDocument6 pagesPeriodontitis Associated with Respiratory DiseaseAquila FP SinagaNo ratings yet
- Association Between Periodontitis and Arterial Hypertension: A Systematic Review and Meta-AnalysisDocument15 pagesAssociation Between Periodontitis and Arterial Hypertension: A Systematic Review and Meta-AnalysisPentiya Vita AyuniNo ratings yet
- Pulpal Inflammation and Incidence of Coronary Heart Disease Joshipura 2006Document5 pagesPulpal Inflammation and Incidence of Coronary Heart Disease Joshipura 2006Jing XueNo ratings yet
- Investigation of Volatile Sulfur Compound Level and Halitosis in Patients With Gingivitis and PeriodontitisDocument11 pagesInvestigation of Volatile Sulfur Compound Level and Halitosis in Patients With Gingivitis and PeriodontitisBilly TrầnNo ratings yet
- Ravald Et Al-2012-Journal of Clinical Periodontology PDFDocument7 pagesRavald Et Al-2012-Journal of Clinical Periodontology PDFChristine HacheNo ratings yet
- Caranza Diagnosis EnglishDocument3 pagesCaranza Diagnosis EnglishZuwandi Abd KadirNo ratings yet
- Recurrence Rates After Surgical Removal of Oral Leukoplakia-A Prospective Longitudinal Multi-Centre StudyDocument13 pagesRecurrence Rates After Surgical Removal of Oral Leukoplakia-A Prospective Longitudinal Multi-Centre StudyRafa LopezNo ratings yet
- Anaerobic BacteriaDocument9 pagesAnaerobic BacteriaKali corgiNo ratings yet
- Periodontal Disease in ChildrenDocument23 pagesPeriodontal Disease in ChildrenBiswaroop ChandraNo ratings yet
- Albandar 2002 Global Epidemiology OverviewDocument4 pagesAlbandar 2002 Global Epidemiology OverviewjeremyvoNo ratings yet
- Global Epidemiology of Periodontal Diseases: An Overview: J M. A & T E. RDocument4 pagesGlobal Epidemiology of Periodontal Diseases: An Overview: J M. A & T E. RkochikaghochiNo ratings yet
- Peerj 5258Document17 pagesPeerj 5258mmputraNo ratings yet
- Abstracts: Abstracts On This Page Have Been Chosen and Edited by DR Trevor WattsDocument1 pageAbstracts: Abstracts On This Page Have Been Chosen and Edited by DR Trevor WattssummoneNo ratings yet
- Risk Factors For Otitis Media in Rural, Preschool South Indian ChildrenDocument20 pagesRisk Factors For Otitis Media in Rural, Preschool South Indian ChildrengoolnuulNo ratings yet
- Journal Pone 0091059Document5 pagesJournal Pone 0091059AgusBhaktiNo ratings yet
- Craniofacial Morphology of HIV-positive Children and Adolescents Undergoing Antiretroviral Therapy: A Pilot StudyDocument10 pagesCraniofacial Morphology of HIV-positive Children and Adolescents Undergoing Antiretroviral Therapy: A Pilot StudyMonojit DuttaNo ratings yet
- Chacon Conversatorio.Document5 pagesChacon Conversatorio.JacoboGonzálezNo ratings yet
- Diploma de Endodoncia Online 18-19Document7 pagesDiploma de Endodoncia Online 18-19shivaniNo ratings yet
- Is Orthodontic Treatment A Risk Factor For Temporomandibular Disorders?Document7 pagesIs Orthodontic Treatment A Risk Factor For Temporomandibular Disorders?gloriagaskNo ratings yet
- 10 1111@idj 12576Document7 pages10 1111@idj 12576badria bawazirNo ratings yet
- Asociacin Enfermedad Periodontal EnfermedadessistTmicasDocument7 pagesAsociacin Enfermedad Periodontal EnfermedadessistTmicasNadya PurwantyNo ratings yet
- Chronic Rhinosinusitis-An Update On Epidemiology, Pathogenesis and ManagementDocument5 pagesChronic Rhinosinusitis-An Update On Epidemiology, Pathogenesis and ManagementNaufal NrwNo ratings yet
- Association of Obesity With Periodontitis, Tooth Loss and Oral Hygiene in Non-Smoking AdultsDocument6 pagesAssociation of Obesity With Periodontitis, Tooth Loss and Oral Hygiene in Non-Smoking AdultsNicolas YoungNo ratings yet
- Association Between Periodontal Pathogens and SeveDocument9 pagesAssociation Between Periodontal Pathogens and Sevepennyshevlin1No ratings yet
- Progression of Periodontal Disease in Individuals With Cleft Lip Alveolus and Palate 8 Year Longitudinal StudyDocument13 pagesProgression of Periodontal Disease in Individuals With Cleft Lip Alveolus and Palate 8 Year Longitudinal StudyAthenaeum Scientific PublishersNo ratings yet
- Chronic Periodontitis GuideDocument80 pagesChronic Periodontitis GuideDrRahat SaleemNo ratings yet
- Journal ToolsDocument22 pagesJournal ToolsChilly0104No ratings yet
- Journal of Periodontology - 2020 - Beck - Periodontal Disease Classifications and Incident Coronary Heart Disease in TheDocument10 pagesJournal of Periodontology - 2020 - Beck - Periodontal Disease Classifications and Incident Coronary Heart Disease in TheSung Soon ChangNo ratings yet
- Chronic Marginal PeriodontitisDocument21 pagesChronic Marginal PeriodontitisLaslo Mihaela Larisa100% (1)
- Periopan - Critical Issues in Periodontal ResearchDocument64 pagesPeriopan - Critical Issues in Periodontal Researchrevu dasNo ratings yet
- Clinical Study: Periodontal Status in Smokers and Nonsmokers: A Clinical, Microbiological, and Histopathological StudyDocument10 pagesClinical Study: Periodontal Status in Smokers and Nonsmokers: A Clinical, Microbiological, and Histopathological StudykleberNo ratings yet
- Supportive Periodontal TherapyDocument6 pagesSupportive Periodontal TherapyIris PavičićNo ratings yet
- 2005 - Blackwell MunsgardDocument78 pages2005 - Blackwell MunsgardIris PavičićNo ratings yet
- Schatzle2004 Gingivitis InflamacionDocument6 pagesSchatzle2004 Gingivitis InflamaciondaruNo ratings yet
- The Clinical Course of Chronic Periodontitis 3Document11 pagesThe Clinical Course of Chronic Periodontitis 3Iris PavičićNo ratings yet
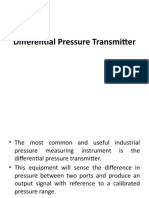
- Differential Pressure TransmitterDocument14 pagesDifferential Pressure TransmitterZainab KadhemNo ratings yet
- Wo PRJ #304Document2 pagesWo PRJ #304Gigin PlusNo ratings yet
- Microwave TubesDocument36 pagesMicrowave TubesHINDUSTAN KNOW 1No ratings yet
- Restraint Prevalence and Perceived Coercion Among Psychiatric Inpatientsfrom South IndiaDocument7 pagesRestraint Prevalence and Perceived Coercion Among Psychiatric Inpatientsfrom South IndiaEdson HilárioNo ratings yet
- The Pediatric Mandible I. A Primer On Growth and DevelopmentDocument10 pagesThe Pediatric Mandible I. A Primer On Growth and DevelopmentJulián David Ríos ZuluagaNo ratings yet
- Electricity Merit Badge Class 1 2017Document34 pagesElectricity Merit Badge Class 1 2017RoshanNo ratings yet
- PPR - LISTS - Registered Medicine Price List - 20221127 BahrainDocument318 pagesPPR - LISTS - Registered Medicine Price List - 20221127 BahrainvdvedNo ratings yet
- Include The Following in Your RTI ApplicationDocument4 pagesInclude The Following in Your RTI ApplicationRam LoharNo ratings yet
- 08 Ergonomics - 01Document35 pages08 Ergonomics - 01Cholan PillaiNo ratings yet
- Lab Report P2 A1 - IDocument19 pagesLab Report P2 A1 - Inzirh 01No ratings yet
- Five Brothers and Their Mother's LoveDocument4 pagesFive Brothers and Their Mother's Lovevelo67% (3)
- Corporate Governance at HavellsDocument16 pagesCorporate Governance at HavellsVishal Pundir100% (1)
- Audi A6 Allroad Model 2013 Brochure - 2012.08Document58 pagesAudi A6 Allroad Model 2013 Brochure - 2012.08Arkadiusz KNo ratings yet
- Sect 5Document25 pagesSect 5PuneetNo ratings yet
- Flatworms Round Worms and Anne Lids LabDocument6 pagesFlatworms Round Worms and Anne Lids LabBellaNo ratings yet
- Iocl Section 1 - Process SpecficationDocument73 pagesIocl Section 1 - Process SpecficationYogi173No ratings yet
- Inverter Controlled Mig Welding-Machine YD-400GT3 Operating ManualDocument53 pagesInverter Controlled Mig Welding-Machine YD-400GT3 Operating ManualsunhuynhNo ratings yet
- Which Statement On Physical Development of Infants and Toddlers Is TRUEDocument9 pagesWhich Statement On Physical Development of Infants and Toddlers Is TRUEKristylle Renz100% (1)
- Pradhan Mantri Gram Sadak Yojana Pradhan Mantri Gram Sadak YojanaDocument19 pagesPradhan Mantri Gram Sadak Yojana Pradhan Mantri Gram Sadak Yojanapriyajaiswal428No ratings yet
- Dead ZoneDocument10 pagesDead ZoneariannaNo ratings yet
- Buller, Paul F. - Schuler, Randall S - Managing Organizations and People - Cases in Management, Organizational Behavior and Human Resource Management-Thomson - South-Western (2006)Document530 pagesBuller, Paul F. - Schuler, Randall S - Managing Organizations and People - Cases in Management, Organizational Behavior and Human Resource Management-Thomson - South-Western (2006)ezekiel capuzNo ratings yet
- Organizational StrategiesDocument2 pagesOrganizational Strategiesapi-362784633No ratings yet
- Grooved Peg BoardDocument2 pagesGrooved Peg BoarddanifgNo ratings yet
- Spectralis Touch Panel Upgrade GuideDocument10 pagesSpectralis Touch Panel Upgrade GuideMohamed AbdulaalNo ratings yet
- World Health OrganizationDocument13 pagesWorld Health OrganizationVincent Ranara Sabornido100% (1)
- MODULE 9: Personal Relationships: Albert Abarabar, Erica Soriano, Lloyd Sarandi, Julius Dela CruzDocument18 pagesMODULE 9: Personal Relationships: Albert Abarabar, Erica Soriano, Lloyd Sarandi, Julius Dela CruzMark Gil GuillermoNo ratings yet
- WHO Guidelines For Drinking Water: Parameters Standard Limits As Per WHO Guidelines (MG/L)Document3 pagesWHO Guidelines For Drinking Water: Parameters Standard Limits As Per WHO Guidelines (MG/L)114912No ratings yet
- Awwa-C302 (1995)Document28 pagesAwwa-C302 (1995)masoudNo ratings yet
- Etymology: StructureDocument2 pagesEtymology: StructureNaga VNo ratings yet
- Noise DetectorDocument19 pagesNoise DetectorPlaban Pratim BhuyanNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (14)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)