You might also like
- AP Psych Anatomy The Brain - Coloring Worksheet - Visual MapDocument2 pagesAP Psych Anatomy The Brain - Coloring Worksheet - Visual MapTiffany GallinaNo ratings yet
- Design ParameterDocument13 pagesDesign ParameterkennysawegNo ratings yet
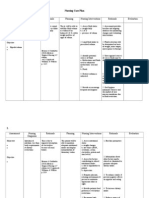
- Nursing Care Plan CKDDocument6 pagesNursing Care Plan CKDReylan Deo Rallo Asio100% (5)
- Womens Basketball Spring Strength Training-2Document1 pageWomens Basketball Spring Strength Training-2api-548848665No ratings yet
- Service Manual: Autoclave Sterilising Sterilclave 18/24Document29 pagesService Manual: Autoclave Sterilising Sterilclave 18/24hüseyin vururNo ratings yet
- DV TUD Brochure 2015v2-SecuredDocument16 pagesDV TUD Brochure 2015v2-SecuredJR RZNo ratings yet
- Karyotype Lab PDFDocument5 pagesKaryotype Lab PDFwelfredo yuNo ratings yet
- 3 - Karyotyping LabDocument17 pages3 - Karyotyping LabEd HouNo ratings yet
- Growth RoataionDocument148 pagesGrowth Roataiondr_nilofervevai2360100% (2)
- Components and Nozzles: Job GuideDocument106 pagesComponents and Nozzles: Job GuideArtur TylickiNo ratings yet
- Damasio Cortical EmotionDocument10 pagesDamasio Cortical EmotionTatiana BuianinaNo ratings yet
- Human KaryotypingDocument7 pagesHuman KaryotypingEditorialranged CartoonistoplaneNo ratings yet
- Prefrontal DerechoDocument10 pagesPrefrontal DerechoSantiago Sepulveda LopezNo ratings yet
- Risa 10Document10 pagesRisa 10gloriaNo ratings yet
- Autobiographical Memory of The Recent Past FollowingDocument12 pagesAutobiographical Memory of The Recent Past FollowingCarlosNo ratings yet
- Noncompaction Left Ventricular Myocardium: Isolated ofDocument8 pagesNoncompaction Left Ventricular Myocardium: Isolated ofMariana NicolaescuNo ratings yet
- Altarelli Et Al-2014-Human Brain MappingDocument19 pagesAltarelli Et Al-2014-Human Brain MappingCharitini PetridouNo ratings yet
- Feline Hyperaesthesia Syndrome Amengualbatle2018Document8 pagesFeline Hyperaesthesia Syndrome Amengualbatle2018João Telhado PereiraNo ratings yet
- Borges 2018Document8 pagesBorges 2018Anthony VillafañeNo ratings yet
- Ooa 90139Document8 pagesOoa 90139Sergio Henrique O. SantosNo ratings yet
- Mujeres Postrau HipocampoDocument4 pagesMujeres Postrau Hipocampojoseluis garrido leccaNo ratings yet
- Cimpanezi Si Exprimare EmotiiDocument11 pagesCimpanezi Si Exprimare Emotiimyhaela_marculescuNo ratings yet
- Morphology and Morphometry of Mental Foramen in Dry Human MandiblesDocument3 pagesMorphology and Morphometry of Mental Foramen in Dry Human MandiblesDragos CiongaruNo ratings yet
- Teratoma in ChildrenDocument5 pagesTeratoma in ChildrenRif'aNo ratings yet
- Awareness of The Functioning of One's Own Limbs Mediated by The Insular Cortex?Document5 pagesAwareness of The Functioning of One's Own Limbs Mediated by The Insular Cortex?Julian GorositoNo ratings yet
- Impairment of Inferior Longitudinal Fasciculus Plays A Role in Visual Memory DisturbanceDocument5 pagesImpairment of Inferior Longitudinal Fasciculus Plays A Role in Visual Memory DisturbanceRuth Noemy Ruiz MangandiNo ratings yet
- Left Ventricular Myxoma: Case ReportDocument5 pagesLeft Ventricular Myxoma: Case ReportSabrina JonesNo ratings yet
- Autobiographical Memory in AmnesiaDocument11 pagesAutobiographical Memory in AmnesiaCarlosNo ratings yet
- Brugger 2013Document7 pagesBrugger 2013Lucas MirandaNo ratings yet
- A Case Series of Tessier 3, 4, 7 and Combined 4, 7 Craniofacial CleftsDocument5 pagesA Case Series of Tessier 3, 4, 7 and Combined 4, 7 Craniofacial CleftsMohammad Wildan Hari SHNo ratings yet
- Antonio Damasio, Hanna Damasio - Fear and The Human AmigdalaDocument13 pagesAntonio Damasio, Hanna Damasio - Fear and The Human AmigdalaAna Victoria Casillas ZapataNo ratings yet
- Test Bank For The Developing Human Clinically Oriented Embryology 8th Edition Moore Isbn 10 1416037063 Isbn 13 9781416037064 DownloadDocument28 pagesTest Bank For The Developing Human Clinically Oriented Embryology 8th Edition Moore Isbn 10 1416037063 Isbn 13 9781416037064 Downloadwhitneycoxmrtsgiwdkx100% (19)
- Ajay D. Wasan, MD, MSC, and Menekse Alpay, MD: Key PointsDocument13 pagesAjay D. Wasan, MD, MSC, and Menekse Alpay, MD: Key PointsMarilyn PinedaNo ratings yet
- SR Human KaryotypeDocument5 pagesSR Human KaryotypeLuz CorralesNo ratings yet
- Pediatric Intraoral RanulaDocument5 pagesPediatric Intraoral RanularinahpsNo ratings yet
- XII Biology Assignment 02Document3 pagesXII Biology Assignment 02RAKSHITHA KNo ratings yet
- Measuring The Duration of Post Traumatic AmnesiaDocument4 pagesMeasuring The Duration of Post Traumatic AmnesiaAnonymous R6ex8BM0No ratings yet
- Lab 07 HandoutDocument10 pagesLab 07 HandoutShyNo ratings yet
- Brain Hemispheres Selectively Track The Expected Value of Contralateral OptionsDocument10 pagesBrain Hemispheres Selectively Track The Expected Value of Contralateral OptionsFrontiersNo ratings yet
- Determinants of Infarct Size During Permanent Occlusion of A Coronary Artery in The Closed Chest DogDocument8 pagesDeterminants of Infarct Size During Permanent Occlusion of A Coronary Artery in The Closed Chest DogAji PrimaNo ratings yet
- 2014 Revisión Sistemática de Columna en Sujetos Asintomáticos PediátricosDocument6 pages2014 Revisión Sistemática de Columna en Sujetos Asintomáticos PediátricosAnyela Gineth Chisaca NieblesNo ratings yet
- 2009 Cheng Schizophrenia Classification Using Regions of Interest in Brain MRIDocument6 pages2009 Cheng Schizophrenia Classification Using Regions of Interest in Brain MRImarciliomeiraNo ratings yet
- Blum 2014Document8 pagesBlum 2014maisaokadaNo ratings yet
- Lis - Spe 2 Moodle A3Document2 pagesLis - Spe 2 Moodle A3Mỹ Khánh HoàngNo ratings yet
- Lee 2018Document4 pagesLee 2018Yogi Putra Adhi PradanaNo ratings yet
- MRI in ChildrenDocument12 pagesMRI in ChildrenNita HandayaniNo ratings yet
- Common Dysmorphic Syndromes in The NICUDocument12 pagesCommon Dysmorphic Syndromes in The NICUDaniel PuertasNo ratings yet
- Ajns 10 276Document6 pagesAjns 10 276Eriekafebriayana RNo ratings yet
- Neural Basis of Prosopagnosia: An fMRI Study: Nouchine HadjikhaniDocument7 pagesNeural Basis of Prosopagnosia: An fMRI Study: Nouchine HadjikhaniBappaditya ChowdhuryNo ratings yet
- Hansen & HansenDocument8 pagesHansen & HansenStéfanie PaesNo ratings yet
- VPP Practical Manual Paper-IDocument135 pagesVPP Practical Manual Paper-I1kshitiz ThakurNo ratings yet
- White and Gray Matter Development in Human Fetal, Newborn and Pediatric BrainsDocument13 pagesWhite and Gray Matter Development in Human Fetal, Newborn and Pediatric BrainsyadiNo ratings yet
- Talk Bad ExampleDocument15 pagesTalk Bad ExampleSarfaraj OviNo ratings yet
- 1 s2.0 S1059131103002322 MainDocument9 pages1 s2.0 S1059131103002322 Maindoni AfrianNo ratings yet
- 1868-Article Text-6804-1-10-20180620Document3 pages1868-Article Text-6804-1-10-20180620Wina ViqaNo ratings yet
- Neuropsychological Abnormalities in A Patient Diagnosed With Frontoparietal MeningiomaDocument4 pagesNeuropsychological Abnormalities in A Patient Diagnosed With Frontoparietal MeningiomaJhoan CaicedoNo ratings yet
- Development of The Human Tail Bud and Splanchnic Mesenchyme: Original ArticleDocument7 pagesDevelopment of The Human Tail Bud and Splanchnic Mesenchyme: Original Articleproject-247758No ratings yet
- Metastatic Brain Tumors - A Retrospective Review in East AzarbyjanDocument3 pagesMetastatic Brain Tumors - A Retrospective Review in East AzarbyjanNailul HumamNo ratings yet
- BrainAsimetry Nelson&Fuku&Aznar)Document4 pagesBrainAsimetry Nelson&Fuku&Aznar)José Antonio Aznar CasanovaNo ratings yet
- The Forced-Choice Paradigm and The Perception of Facial Expressions of EmotionDocument11 pagesThe Forced-Choice Paradigm and The Perception of Facial Expressions of EmotionjnkjnNo ratings yet
- Develop Med Child Neuro - 2007 - Laurent Vannier - Assessment of Unilateral Spatial Neglect in Children Using The TeddyDocument6 pagesDevelop Med Child Neuro - 2007 - Laurent Vannier - Assessment of Unilateral Spatial Neglect in Children Using The TeddyElisabeth MarionNo ratings yet
- 01 Sap 0000182656 59384 A2Document5 pages01 Sap 0000182656 59384 A2Karuna ShresthaNo ratings yet
- 6 - Embryology - PASS - MRCOG 2017Document22 pages6 - Embryology - PASS - MRCOG 2017emadhishamaburawiNo ratings yet
- Phenomenological Research Design Presentation 7-4-2022Document17 pagesPhenomenological Research Design Presentation 7-4-2022Afar FahmieNo ratings yet
- The Outgroup Homogeneity Effect: What Happens When Faces Are Angry?Document15 pagesThe Outgroup Homogeneity Effect: What Happens When Faces Are Angry?DanielNo ratings yet
- Turner's Syndrome: Review ArticleDocument12 pagesTurner's Syndrome: Review ArticleAnonymous LAWfm7No ratings yet
- Genetic Disorder Fact SheetDocument3 pagesGenetic Disorder Fact SheetPreethy JayNo ratings yet
- Atlas of the Prenatal Mouse BrainFrom EverandAtlas of the Prenatal Mouse BrainUta B. SchambraNo ratings yet
- Ijesrt: International Journal of Engineering Sciences & Research TechnologyDocument11 pagesIjesrt: International Journal of Engineering Sciences & Research TechnologyAna MariaNo ratings yet
- Monobond Etch&PrimeDocument23 pagesMonobond Etch&Primehot_teethNo ratings yet
- HUDA Policy Allowing Four BasementsDocument3 pagesHUDA Policy Allowing Four BasementsRahul JindalNo ratings yet
- HUAWEI CUN U29-Bitel Phone Upgrade Guide - V1.1 - 20161128Document10 pagesHUAWEI CUN U29-Bitel Phone Upgrade Guide - V1.1 - 20161128Danny J GonzalezNo ratings yet
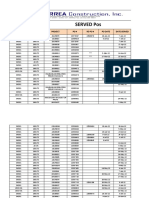
- Served POsDocument21 pagesServed POsYay DumaliNo ratings yet
- HB806TM PDFDocument121 pagesHB806TM PDFhermie100% (1)
- Literature Review and Case StudyDocument4 pagesLiterature Review and Case StudyNimNo ratings yet
- RmitDocument9 pagesRmitrajeevermaNo ratings yet
- Harga Satuan Precast 2017Document2 pagesHarga Satuan Precast 2017GenTigaBrotherhood BantenNo ratings yet
- Identifying, Understanding, and Analyzing: by Steven M. Rinaldi, James P. Peerenboom, and Terrence K. KellyDocument15 pagesIdentifying, Understanding, and Analyzing: by Steven M. Rinaldi, James P. Peerenboom, and Terrence K. KellySFC JGDNo ratings yet
- Martin Gwapo JheroDocument8 pagesMartin Gwapo Jherokent baboys19No ratings yet
- Dungeon Gits: Very Small RoleplayingDocument6 pagesDungeon Gits: Very Small RoleplayingjedvardNo ratings yet
- Wind PumpDocument6 pagesWind PumpCarlos Castillo PalmaNo ratings yet
- Classified Coordinate Geometry Further Maths ExercisesDocument24 pagesClassified Coordinate Geometry Further Maths ExercisesAbrar RahmanNo ratings yet
- Worksheet of EDC - 2018Document2 pagesWorksheet of EDC - 2018pranavmurthyNo ratings yet
- Burroughs Jungle Tales of TarzanDocument133 pagesBurroughs Jungle Tales of Tarzanfr1z1derNo ratings yet
- Dinah HWDocument6 pagesDinah HWDinah AquinoNo ratings yet
- Tetrasteel 800 BrochureDocument4 pagesTetrasteel 800 BrochurejcrandleNo ratings yet
- An Accurate DDS Method Using Compound Frequency Tuning Word and Its FPGA ImplementationDocument14 pagesAn Accurate DDS Method Using Compound Frequency Tuning Word and Its FPGA ImplementationKit CornNo ratings yet
- 2021 CAPEX - THEODORE Chiller Spares v1.3Document6 pages2021 CAPEX - THEODORE Chiller Spares v1.3Paul CansinoNo ratings yet
- Personalized Implants Restore Smiles - EDRMedesoDocument7 pagesPersonalized Implants Restore Smiles - EDRMedesovivekanandNo ratings yet