You might also like
- 9 Types of Female Orgasms ExplainedDocument4 pages9 Types of Female Orgasms ExplainedAbdul SyukurNo ratings yet
- Care of Patient With Respiratory DisordersDocument35 pagesCare of Patient With Respiratory Disorderskriiteeabns100% (1)
- Surgical Site InfectionDocument8 pagesSurgical Site Infection1234chocoNo ratings yet
- Fat-Burning FoodsDocument11 pagesFat-Burning FoodsRamzi FaddoulNo ratings yet
- Brief History of Patient Safety Culture and ScienceDocument4 pagesBrief History of Patient Safety Culture and ScienceHoli100% (1)
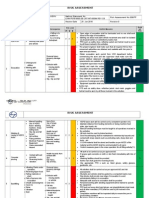
- Hse Risk Assessment - 006 Ra - Hdpe Duct LayingDocument7 pagesHse Risk Assessment - 006 Ra - Hdpe Duct Layingbinunalukandam83% (12)
- World Patient Safety DayDocument17 pagesWorld Patient Safety DayNam PHẠM THÀNHNo ratings yet
- Food Safety Plan For CateringDocument80 pagesFood Safety Plan For CateringNghia Khang100% (1)
- Prevention of Surgical Site InfectionDocument10 pagesPrevention of Surgical Site InfectionValiant Baybay100% (1)
- Solution Focused TherapyDocument8 pagesSolution Focused Therapyrimpa29No ratings yet
- Scalpel Safety Sinnott2010Document9 pagesScalpel Safety Sinnott2010Guille Puertas100% (1)
- Babu Jagjivan RamDocument24 pagesBabu Jagjivan RamAnonymous qFWInco8cNo ratings yet
- SpitzDocument30 pagesSpitzprabhatNo ratings yet
- Human Skin Wounds: A Growing Threat to Public Health and the EconomyDocument14 pagesHuman Skin Wounds: A Growing Threat to Public Health and the EconomyNurul Mahyani DaudNo ratings yet
- Chandan K. Sen, PHD PDFDocument14 pagesChandan K. Sen, PHD PDFNurul Mahyani DaudNo ratings yet
- Elderly Hip Fracture PatientsDocument7 pagesElderly Hip Fracture PatientspamancastroNo ratings yet
- WHO HIS SDS 2017.11 Eng PDFDocument20 pagesWHO HIS SDS 2017.11 Eng PDFJayalakshmi JayarajanNo ratings yet
- Articulo 2Document9 pagesArticulo 2Gustavo Gonzales ChavezNo ratings yet
- Falls Prevention in Hospitals-The Need For A New Approach An Integrative ArticleDocument4 pagesFalls Prevention in Hospitals-The Need For A New Approach An Integrative ArticleDwi NopriyantoNo ratings yet
- 4839701Document12 pages4839701mkoffietranhanssaviolaNo ratings yet
- Evidence-Based Medicine: The Evaluation and Treatment of Pressure InjuriesDocument12 pagesEvidence-Based Medicine: The Evaluation and Treatment of Pressure InjuriesIndahEkaPutriNo ratings yet
- Pressure Ulcer Assessment and Treatment (PDFDrive)Document88 pagesPressure Ulcer Assessment and Treatment (PDFDrive)Amna AliNo ratings yet
- Late Immune Consequences of Combat Trauma: A Review of Trauma-Related Immune Dysfunction and Potential TherapiesDocument13 pagesLate Immune Consequences of Combat Trauma: A Review of Trauma-Related Immune Dysfunction and Potential TherapiesQariahMaulidiahAminNo ratings yet
- Acute Management of Open Fractures An Evidence Based Review PDFDocument9 pagesAcute Management of Open Fractures An Evidence Based Review PDFSusPa Naraha100% (1)
- MSC Proposal - Quantitative - 2019Document32 pagesMSC Proposal - Quantitative - 2019Lihle Mirriam MdlaloseNo ratings yet
- 2018 Seasonal InfluenzaDocument47 pages2018 Seasonal InfluenzaMariaNo ratings yet
- The Most Effective Fall Prevention Program For Patients Over 65 Years - An Integrated Literature ReviewDocument26 pagesThe Most Effective Fall Prevention Program For Patients Over 65 Years - An Integrated Literature Reviewhal kadduNo ratings yet
- Hard-To-Heal Wounds, Biofilm and Wound Healing: An Intricate InterrelationshipDocument6 pagesHard-To-Heal Wounds, Biofilm and Wound Healing: An Intricate InterrelationshipHan's OfficialNo ratings yet
- Jurnal LainDocument22 pagesJurnal LainBudi ArsanaNo ratings yet
- Atls MedscapeDocument5 pagesAtls MedscapeCastay GuerraNo ratings yet
- Surgical Site InfectionsDocument29 pagesSurgical Site Infectionsalfredochelo1921No ratings yet
- Burden of Surgical Site Infections in The NetherlandsDocument10 pagesBurden of Surgical Site Infections in The NetherlandsKanokwan BorwornphiphattanachaiNo ratings yet
- 2016 Article 329Document6 pages2016 Article 329anon_242145531No ratings yet
- Dr. Santi Rahayu Dewayanti, MM, Sp. P, FCCP, FISR - RevDocument31 pagesDr. Santi Rahayu Dewayanti, MM, Sp. P, FCCP, FISR - RevRensa KaruniaNo ratings yet
- Influenza GuidelinesDocument47 pagesInfluenza GuidelinesKok Hui DiongNo ratings yet
- Improving global patient safety through coordinated actionDocument8 pagesImproving global patient safety through coordinated actioncynthiaNo ratings yet
- Updated IDSA GuidelinesDocument47 pagesUpdated IDSA GuidelinesAhmed EzzatNo ratings yet
- Global Patient Safety Challenge - WHODocument35 pagesGlobal Patient Safety Challenge - WHOjoaopinheiro88No ratings yet
- HHS Public Access: Chest Trauma Outcomes: Public Versus Private Level I Trauma CentersDocument19 pagesHHS Public Access: Chest Trauma Outcomes: Public Versus Private Level I Trauma CentersIthaNo ratings yet
- Healthcare Costs of Injuries in the PhilippinesDocument6 pagesHealthcare Costs of Injuries in the Philippineshaechan's fluffy bucket hatNo ratings yet
- Clinical Errors and Medical Negligence: ReviewDocument11 pagesClinical Errors and Medical Negligence: ReviewAnggreanyAshariNo ratings yet
- Pathophysiology in Patients With PolytraumaDocument13 pagesPathophysiology in Patients With PolytraumaRodolfo M. N.B.No ratings yet
- Avoidable Surgical Disasters: Errors or Preventable OutcomesDocument7 pagesAvoidable Surgical Disasters: Errors or Preventable OutcomesGopi JaladiNo ratings yet
- Pre Hos TraumaDocument11 pagesPre Hos TraumaGel OmugtongNo ratings yet
- Antimicrobials and Non-Healing WoundsDocument92 pagesAntimicrobials and Non-Healing WoundsNelu CastravetNo ratings yet
- Duodeno-Pancreatic and Extrahepatic Biliary Tree Trauma - WSES-AAST Guidelines Open AccessDocument23 pagesDuodeno-Pancreatic and Extrahepatic Biliary Tree Trauma - WSES-AAST Guidelines Open AccessDiego Andres VasquezNo ratings yet
- Management of Burns Patient Before Arrival at National Orthopedic Hospital EnuguDocument41 pagesManagement of Burns Patient Before Arrival at National Orthopedic Hospital EnuguDONEKE MIRACLENo ratings yet
- Ren 2018Document7 pagesRen 2018atikahanifahNo ratings yet
- Patient Safety Menurut WHODocument9 pagesPatient Safety Menurut WHOAlwan NugrohoNo ratings yet
- 10 Facts On Patient SafetyDocument3 pages10 Facts On Patient SafetySafiqulatif AbdillahNo ratings yet
- Does Pressure Cause Pressure Ulcers? An Inquiry Into The Etiology of Pressure UlcersDocument9 pagesDoes Pressure Cause Pressure Ulcers? An Inquiry Into The Etiology of Pressure Ulcersvaleria molinaNo ratings yet
- 68 2020 Article 1412Document7 pages68 2020 Article 1412Andres De LeonNo ratings yet
- Risk FactorDocument5 pagesRisk FactorBima AryaputraNo ratings yet
- Trauma ThoraxDocument7 pagesTrauma ThoraxLuqmanul Hakim JunaiddenNo ratings yet
- Wound CareDocument42 pagesWound CareNorma Khoirun Nisa100% (1)
- Acute Nursing Care of The Older Adult With Fragility Hip Fracture: An International Perspective (Part 2)Document26 pagesAcute Nursing Care of The Older Adult With Fragility Hip Fracture: An International Perspective (Part 2)spring flowerNo ratings yet
- The Impact of Pressure Ulcers: Bony Sacrum Coccyx Heels Hips Elbows Knees Ankles CraniumDocument48 pagesThe Impact of Pressure Ulcers: Bony Sacrum Coccyx Heels Hips Elbows Knees Ankles CraniumVanessa Camille DomingoNo ratings yet
- Risk Factors For Falls in Hospital In-Patients: A Prospective Nested Case Control StudyDocument7 pagesRisk Factors For Falls in Hospital In-Patients: A Prospective Nested Case Control StudyNurhasanah HaryaniNo ratings yet
- Pitt Et 2008Document8 pagesPitt Et 2008GrevaldoNo ratings yet
- Maxillofacial TraumaDocument15 pagesMaxillofacial TraumadewiswahyuNo ratings yet
- Patient Safety WHODocument8 pagesPatient Safety WHONovitaSariNo ratings yet
- Eichinger2021_Article_ChallengesInThePREHOSPITALEmerDocument12 pagesEichinger2021_Article_ChallengesInThePREHOSPITALEmerBarry TraceyNo ratings yet
- Presus DR HardDocument5 pagesPresus DR HardAhmad MusafiNo ratings yet
- Ronald V. Maier, M.D.: Awards: FundingDocument5 pagesRonald V. Maier, M.D.: Awards: Fundingyanuar andaniNo ratings yet
- Peek Et Al. Rib Fractures Nation-Wide StudyDocument7 pagesPeek Et Al. Rib Fractures Nation-Wide StudyRut Herdianti P. EkasiwiNo ratings yet
- Sciadv Ade7007Document11 pagesSciadv Ade7007Poramate PITAK-ARNNOPNo ratings yet
- Ol 20 1 441 PDFDocument7 pagesOl 20 1 441 PDFeka satyani belinaNo ratings yet
- Pressure Ulcers in the Aging Population: A Guide for CliniciansFrom EverandPressure Ulcers in the Aging Population: A Guide for CliniciansDavid R. Thomas, MDNo ratings yet
- Defect eDocument2 pagesDefect eHeba VerebceanNo ratings yet
- The Use of Chitin and Chitosan in MDocument21 pagesThe Use of Chitin and Chitosan in MHeba VerebceanNo ratings yet
- Gerry Rayman Prashanth Vas Ketan Dhatariya Vicki Driver Agnes Hartemann Magnus Londahl Alberto Piaggesi Jan Apelqvist Chris Attinger Fran GameDocument17 pagesGerry Rayman Prashanth Vas Ketan Dhatariya Vicki Driver Agnes Hartemann Magnus Londahl Alberto Piaggesi Jan Apelqvist Chris Attinger Fran GameHeba VerebceanNo ratings yet
- Structura ProteinelorDocument6 pagesStructura Proteinelorconstiinta47No ratings yet
- Cazuri CliniceDocument32 pagesCazuri CliniceHeba VerebceanNo ratings yet
- Ijerph 19 01338 v2Document25 pagesIjerph 19 01338 v2Heba VerebceanNo ratings yet
- 6 Parenteral Nutrition Online PDF-62175Document42 pages6 Parenteral Nutrition Online PDF-62175Heba VerebceanNo ratings yet
- Health-Related Quality of Life, Self-Esteem, and Functional Status of Patients With Leg UlcersDocument8 pagesHealth-Related Quality of Life, Self-Esteem, and Functional Status of Patients With Leg UlcersHeba VerebceanNo ratings yet
- Mo Loney 2004Document4 pagesMo Loney 2004Heba VerebceanNo ratings yet
- Wound Management For The 21st Century: Combining Effectiveness and EfficiencyDocument11 pagesWound Management For The 21st Century: Combining Effectiveness and EfficiencyHeba VerebceanNo ratings yet
- Hydrocolloid Dressing PDFDocument17 pagesHydrocolloid Dressing PDFeyleenNo ratings yet
- Chronic Cutaneous Ulcers: Etiology and Epidemiology: Taniaj. PhillipsDocument5 pagesChronic Cutaneous Ulcers: Etiology and Epidemiology: Taniaj. PhillipsHeba VerebceanNo ratings yet
- Dr. Amit Gupta Associate Professor Dept of SurgeryDocument43 pagesDr. Amit Gupta Associate Professor Dept of SurgeryHeba VerebceanNo ratings yet
- 37b7c2326a4dcbaa729c0a733d8b8c42Document1 page37b7c2326a4dcbaa729c0a733d8b8c42Heba VerebceanNo ratings yet
- Special Wound Healing Methods Used in Ancient Egypt and The Mythological BackgroundDocument6 pagesSpecial Wound Healing Methods Used in Ancient Egypt and The Mythological BackgroundHeba VerebceanNo ratings yet
- Krull 1985Document8 pagesKrull 1985Heba VerebceanNo ratings yet
- Krull 1985Document8 pagesKrull 1985Heba VerebceanNo ratings yet
- Mo Loney 2004Document4 pagesMo Loney 2004Heba VerebceanNo ratings yet
- 10 3389@fbioe 2020 00182Document17 pages10 3389@fbioe 2020 00182Heba VerebceanNo ratings yet
- Chronic Wound Healing Review: Current Management and TreatmentsDocument12 pagesChronic Wound Healing Review: Current Management and TreatmentsHeba VerebceanNo ratings yet
- Chronic Cutaneous Ulcers: Etiology and Epidemiology: Taniaj. PhillipsDocument5 pagesChronic Cutaneous Ulcers: Etiology and Epidemiology: Taniaj. PhillipsHeba VerebceanNo ratings yet
- Student Letter 2022Document1 pageStudent Letter 2022Heba VerebceanNo ratings yet
- Student Letter 2022Document1 pageStudent Letter 2022Heba VerebceanNo ratings yet
- Study Case Analysis GuidelineDocument1 pageStudy Case Analysis GuidelineHeba VerebceanNo ratings yet
- Study Case Analysis GuidelineDocument1 pageStudy Case Analysis GuidelineHeba VerebceanNo ratings yet
- Alcoholism and mental health conditionsDocument2 pagesAlcoholism and mental health conditionsHeba VerebceanNo ratings yet
- 10 3389@fbioe 2020 00182Document17 pages10 3389@fbioe 2020 00182Heba VerebceanNo ratings yet
- Study Case Analysis GuidelineDocument1 pageStudy Case Analysis GuidelineHeba VerebceanNo ratings yet
- 01 Raspuns La Teste. SensibilitateaDocument1 page01 Raspuns La Teste. SensibilitateaHeba VerebceanNo ratings yet
- Calculator NotesDocument4 pagesCalculator NotessdiamanNo ratings yet
- Young InfantDocument69 pagesYoung InfantAurora Doris BatagaNo ratings yet
- Human Population and EnvironmentDocument4 pagesHuman Population and Environmentmonkeybike88No ratings yet
- A Study On Environmental Impact of Madukkarai Limestone Mine, CoimbatoreDocument11 pagesA Study On Environmental Impact of Madukkarai Limestone Mine, CoimbatoreRamasamyNagarajan100% (1)
- Vacation With Sunny Leone - Without FlightDocument4 pagesVacation With Sunny Leone - Without FlightkalidasdoraemonNo ratings yet
- Republic Act 10932 Anti-Hospital Deposit LawDocument9 pagesRepublic Act 10932 Anti-Hospital Deposit LawVenus PangilinanNo ratings yet
- Central Pain Syndrome - Pathophysiol., Diag., Mgmt. - S. Canavero, Et. Al., (Cambridge, 2006) WW PDFDocument398 pagesCentral Pain Syndrome - Pathophysiol., Diag., Mgmt. - S. Canavero, Et. Al., (Cambridge, 2006) WW PDFRomeo-Remus RaffaiNo ratings yet
- (Bio 024) Lab Activity 12 - BloodDocument9 pages(Bio 024) Lab Activity 12 - Bloodelaq dr100% (1)
- MSDSDocument3 pagesMSDSSiti Nurjanah SeptianiNo ratings yet
- Intrathecal MTX & Cytarabine & Hydrocortisone V4 2.15Document2 pagesIntrathecal MTX & Cytarabine & Hydrocortisone V4 2.15GabrielNo ratings yet
- Pathological Urine ConstituentsDocument22 pagesPathological Urine Constituentsmanni1001100% (3)
- Soal Bahasa Inggris Kelas 5Document8 pagesSoal Bahasa Inggris Kelas 5imam hambaliNo ratings yet
- Nursing Care Plan for Patient SafetyDocument9 pagesNursing Care Plan for Patient SafetyACOB, Jamil C.No ratings yet
- Maynilad Valenzuela Sewerage Project Environmental ReportDocument297 pagesMaynilad Valenzuela Sewerage Project Environmental ReportmarvilouNo ratings yet
- Que No4 & 5-With Clues and Without CluesDocument4 pagesQue No4 & 5-With Clues and Without CluesMir Yamin Uddin ZidanNo ratings yet
- Nursing and Midwifery Board Candidate Handbook RN OSCE ExaminationDocument25 pagesNursing and Midwifery Board Candidate Handbook RN OSCE ExaminationkemalayazNo ratings yet
- Exercises For Task 3 InglesDocument3 pagesExercises For Task 3 InglesNoelia De Los SantosNo ratings yet
- CV 2020Document3 pagesCV 2020api-519861494No ratings yet
- Marihuana EsquizofreniaDocument30 pagesMarihuana EsquizofreniaJ Elver SilvaNo ratings yet
- Connectors 2Document14 pagesConnectors 2Irene SánchezNo ratings yet
- Guide To Patient Support and Regional Cancer ServicesDocument76 pagesGuide To Patient Support and Regional Cancer Servicesgiovanna2004No ratings yet
- Awarness About Breast CancerDocument4 pagesAwarness About Breast CancerliaahlanNo ratings yet