You might also like
- POSITION EMS Spinal Precautions and The Use of The Long BackboardDocument2 pagesPOSITION EMS Spinal Precautions and The Use of The Long BackboardJade OttoniNo ratings yet
- Patients Immobilized With A Long Spine Board Rarely Have Unstable Thoracolumbar InjuriesDocument8 pagesPatients Immobilized With A Long Spine Board Rarely Have Unstable Thoracolumbar InjuriesJade OttoniNo ratings yet
- Out of Hospital Spinal Immobilization - Its Effect On Neurologic InjuryDocument7 pagesOut of Hospital Spinal Immobilization - Its Effect On Neurologic InjuryJade OttoniNo ratings yet
- Pre-Hospital Spinal Immobilisation - An Initial Consensus StatementDocument4 pagesPre-Hospital Spinal Immobilisation - An Initial Consensus StatementJade OttoniNo ratings yet
- Less Is More: Psychologists Can Learn More by Studying Fewer PeopleDocument4 pagesLess Is More: Psychologists Can Learn More by Studying Fewer PeopleJade OttoniNo ratings yet
- Michael 1974Document7 pagesMichael 1974Jade OttoniNo ratings yet
- (NEXUS) Selective Cervical Spine Radiography in Blunt Trauma - Methodology of The National Emergency X-Radiography Utilization StudyDocument9 pages(NEXUS) Selective Cervical Spine Radiography in Blunt Trauma - Methodology of The National Emergency X-Radiography Utilization StudyJade OttoniNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- First Aid TrainingDocument3 pagesFirst Aid Trainingkenshi maddNo ratings yet
- The Script of English DramaDocument4 pagesThe Script of English DramaDhania DjulianNo ratings yet
- Chapter 1 Part 1 Multiple ChoiceDocument4 pagesChapter 1 Part 1 Multiple ChoiceArlanosaurusNo ratings yet
- First Aid Manual - 9th Edition RevisedDocument289 pagesFirst Aid Manual - 9th Edition RevisedJanko Mesić91% (34)
- First Aid For UnconsciousnessDocument3 pagesFirst Aid For UnconsciousnessHazel Mjkristell Basallote FranceNo ratings yet
- Assessment Tool - AmbulanceDocument12 pagesAssessment Tool - AmbulanceJerome Angelo LascanoNo ratings yet
- Special Articles: Awake Intubation Intubation After Induction of General AnesthesiaDocument1 pageSpecial Articles: Awake Intubation Intubation After Induction of General AnesthesiaOKE channelNo ratings yet
- CPR PosterDocument1 pageCPR PosterHemantNo ratings yet
- Four Basic Rules: Prefinal Safety, Security and Emergency PreparednessDocument3 pagesFour Basic Rules: Prefinal Safety, Security and Emergency PreparednessQueenie Kaye FrontalNo ratings yet
- Medico-Legal Aspect of InjuryDocument25 pagesMedico-Legal Aspect of InjuryShahriar Shaon100% (1)
- Triage and Disaster: Nur Masyeerah Abdul JalilDocument22 pagesTriage and Disaster: Nur Masyeerah Abdul JalilnavenNo ratings yet
- Transport of The Critically Ill Patient PDFDocument4 pagesTransport of The Critically Ill Patient PDFaksinuNo ratings yet
- TesteDocument589 pagesTesteJose Wo Oliveira SobrinhoNo ratings yet
- Glasgow Coma ScaleDocument3 pagesGlasgow Coma ScaleMuhamad RidloNo ratings yet
- Basic First Aid in Sports InjuriesDocument26 pagesBasic First Aid in Sports InjuriesAkanksha PatilNo ratings yet
- Pascrell Letter To HCADocument4 pagesPascrell Letter To HCARachel CohrsNo ratings yet
- First Aid: Help School ProjectDocument6 pagesFirst Aid: Help School Projectabhishek_magic123No ratings yet
- Penetrating TraumaDocument29 pagesPenetrating TraumaArdianto SucintaNo ratings yet
- WHO Tools Slide Deck: September 2019Document15 pagesWHO Tools Slide Deck: September 2019Araa AsukaNo ratings yet
- First Responders Functions, Responsibilities and ProceduresDocument36 pagesFirst Responders Functions, Responsibilities and ProceduresDennis Esik MaligayaNo ratings yet
- ATLS Case ScenarioDocument13 pagesATLS Case ScenarioJenny Schneider100% (2)
- Closed Head Injury CPG 2nd Ed Algorithm 2Document1 pageClosed Head Injury CPG 2nd Ed Algorithm 2Nick PaulNo ratings yet
- JADWAL BLENDED LEARNING BTCLS 5 HariDocument3 pagesJADWAL BLENDED LEARNING BTCLS 5 HariwidyaaladinNo ratings yet
- Medical Plan ICS 206Document3 pagesMedical Plan ICS 206RexNo ratings yet
- NZ Nursing Assessment Framework SummaryDocument3 pagesNZ Nursing Assessment Framework SummaryvlahndysonNo ratings yet
- Agreement For Medical TransportationDocument4 pagesAgreement For Medical TransportationJoga BonitaNo ratings yet
- 4 - Prehospital Management Particularities of The Patient With Cardiorespiratory ArrestDocument18 pages4 - Prehospital Management Particularities of The Patient With Cardiorespiratory ArrestGhimpu DanielaNo ratings yet
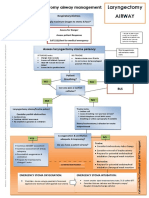
- Laryngectomy Airway: Emergency Tracheostomy Airway ManagementDocument1 pageLaryngectomy Airway: Emergency Tracheostomy Airway ManagementDana IlieNo ratings yet
- The First, First ResponderDocument26 pagesThe First, First ResponderJose Enrique Patron GonzalezNo ratings yet
- 2023 12 14 HCA ComplaintDocument58 pages2023 12 14 HCA ComplaintMitchell BlackNo ratings yet