You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- High-Risk Pregnancy CareDocument34 pagesHigh-Risk Pregnancy CareShaufyqyn EzaniNo ratings yet
- BookOfSuicide1 201Document103 pagesBookOfSuicide1 201DEShifNo ratings yet
- Ansi A10.42Document23 pagesAnsi A10.42pedro la rosa100% (1)
- 5 Day Challenge FBDocument13 pages5 Day Challenge FBInees100% (1)
- Power Point AutismDocument11 pagesPower Point Autismjakolej949954100% (1)
- The Art of Threads A Comprehensive ReviewDocument17 pagesThe Art of Threads A Comprehensive Reviewalejandro Gonzàlez80% (5)
- PANCE Word Associations PDFDocument27 pagesPANCE Word Associations PDFkatNo ratings yet
- Water Resources EngineeringDocument22 pagesWater Resources EngineeringBethel Princess Flores100% (1)
- Simulidae BlackflyDocument17 pagesSimulidae BlackflyVasimNo ratings yet
- Vessel Due FDocument2 pagesVessel Due Fianecunar88% (8)
- IPO Vijaya Diagnostic - 01092021 1630476491Document6 pagesIPO Vijaya Diagnostic - 01092021 1630476491Neil MannikarNo ratings yet
- Folleto Medicamentos de Alto Riesgo GeneralidadesDocument1 pageFolleto Medicamentos de Alto Riesgo GeneralidadesGabee MoralesNo ratings yet
- Lumbar Spinal Stenosis: Syndrome, Diagnostics and Treatment: Nature Reviews Neurology August 2009Document13 pagesLumbar Spinal Stenosis: Syndrome, Diagnostics and Treatment: Nature Reviews Neurology August 2009Surya PangeranNo ratings yet
- Neurosurgery Cases and Reviews NCR 4 056Document11 pagesNeurosurgery Cases and Reviews NCR 4 056Surya PangeranNo ratings yet
- Degenerative Cervical Myelopathy: Clinical Presentation, Assessment, and Natural HistoryDocument12 pagesDegenerative Cervical Myelopathy: Clinical Presentation, Assessment, and Natural HistorySurya PangeranNo ratings yet
- Cervical Spondylotic Myelopathy: A Guide To Diagnosis and ManagementDocument11 pagesCervical Spondylotic Myelopathy: A Guide To Diagnosis and ManagementSurya PangeranNo ratings yet
- OetDocument5 pagesOetGina Victor100% (2)
- Work Smarts Logic Smart GuideDocument2 pagesWork Smarts Logic Smart GuideDian KhoeroniNo ratings yet
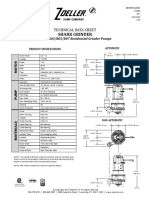
- Ficha Tecnica E803Document2 pagesFicha Tecnica E803Zenen AlarconNo ratings yet
- Protocol SummaryDocument4 pagesProtocol Summaryapi-635954562No ratings yet
- CHOLElithiasisDocument93 pagesCHOLElithiasisfranciscomaricris13No ratings yet
- Jenis PestisidaDocument12 pagesJenis PestisidahenryashterNo ratings yet
- Pediatric Nursing Caring For Children and Their Families 3rd Edition Potts Test BankDocument18 pagesPediatric Nursing Caring For Children and Their Families 3rd Edition Potts Test Bankannabellaauroravb5cf100% (24)
- 1.neuro Intro-1 UMTDocument51 pages1.neuro Intro-1 UMTLOVELY WALEEDNo ratings yet
- Name: Mark Jhon T. Baliwang Section: Aluminum-ADocument2 pagesName: Mark Jhon T. Baliwang Section: Aluminum-ATayaban Van GihNo ratings yet
- Financial Markets: Saint Columban College Pagadian CityDocument11 pagesFinancial Markets: Saint Columban College Pagadian CityangelNo ratings yet
- Loyola Public School, Loyola Nagar, Guntur - 522005 Promotion From Class VIII To IXDocument1 pageLoyola Public School, Loyola Nagar, Guntur - 522005 Promotion From Class VIII To IXDevi KalyanNo ratings yet
- NMC Strategy 2020 2025 SummaryDocument12 pagesNMC Strategy 2020 2025 SummaryNiq CstrNo ratings yet
- Falls Efficacy Scale PDFDocument2 pagesFalls Efficacy Scale PDFRyanNo ratings yet
- Makalah Reading Format Pleasure: Dosen Pengampuh: Irfan Hamonangan Tarihoran, S.S., M. HumDocument6 pagesMakalah Reading Format Pleasure: Dosen Pengampuh: Irfan Hamonangan Tarihoran, S.S., M. HumTitania JulinarNo ratings yet
- Online Course in Science Journalism: Lesson 2 - Finding and Judging Science StoriesDocument22 pagesOnline Course in Science Journalism: Lesson 2 - Finding and Judging Science StoriesleksremeshNo ratings yet
- Temporomandibular Disorders: A Term Whose Time Has Passed!: PerspectivesDocument2 pagesTemporomandibular Disorders: A Term Whose Time Has Passed!: PerspectivesUmer HussainNo ratings yet
- Clinical ResumeDocument6 pagesClinical Resumeapi-284041802No ratings yet
- Mpulungu Trust Summary ProfileDocument4 pagesMpulungu Trust Summary ProfileViktor Dmitri KanyozeNo ratings yet