You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Cardiogenic ShockDocument14 pagesCardiogenic ShockZellanien hdNo ratings yet
- Pulses: Shu Chi HuanDocument1 pagePulses: Shu Chi HuanRicardo TeixeiraNo ratings yet
- 150421007-1504 Lipids CalibratorDocument8 pages150421007-1504 Lipids CalibratorSabithaNo ratings yet
- Cardiogenic Pulmonary EdemaDocument1 pageCardiogenic Pulmonary EdemaAirish LimNo ratings yet
- Mass Transport - Checklist PDFDocument3 pagesMass Transport - Checklist PDFZain KhanNo ratings yet
- Prelims Pedia 102Document10 pagesPrelims Pedia 102quidditch07No ratings yet
- Description: Clonidine: Drug Mechanism of Action Indication Contraindication Adverse Effects Nursing ImplicationsDocument2 pagesDescription: Clonidine: Drug Mechanism of Action Indication Contraindication Adverse Effects Nursing ImplicationsThimiNo ratings yet
- Adequacy of PerfusionDocument11 pagesAdequacy of PerfusionLaiba SiddiqueNo ratings yet
- PathoDocument2 pagesPathohrry stylesNo ratings yet
- Obtaining An ECG ChecklistDocument2 pagesObtaining An ECG ChecklistSophia DimayugaNo ratings yet
- Adrenergic and Anti-Adrenergic DrugsDocument54 pagesAdrenergic and Anti-Adrenergic DrugsChittaranjan Padhy100% (1)
- (English) About Your Heart Attack - Nucleus Health (DownSub - Com)Document2 pages(English) About Your Heart Attack - Nucleus Health (DownSub - Com)Ken Brian NasolNo ratings yet
- Knowledge of Post Discharge Home Care Management Among Patients With Myocardial InfarctionDocument49 pagesKnowledge of Post Discharge Home Care Management Among Patients With Myocardial InfarctionRumela Ganguly ChakrabortyNo ratings yet
- History TakingDocument12 pagesHistory TakingNG RUI ZHAONo ratings yet
- Paralele Lijekova: Generičko Ime Djelovanje Tvorničko ImeDocument3 pagesParalele Lijekova: Generičko Ime Djelovanje Tvorničko ImeStella GašparušNo ratings yet
- KDIGO BP Management in CKD GL Public Review Draft Jan 31 2020Document135 pagesKDIGO BP Management in CKD GL Public Review Draft Jan 31 2020Razel Kinette AzotesNo ratings yet
- RFQ Form - Hemodialysis MachineDocument2 pagesRFQ Form - Hemodialysis MachineStanley GanNo ratings yet
- Rotablator Brochure (PI-208403-AD)Document3 pagesRotablator Brochure (PI-208403-AD)Nasru llahNo ratings yet
- Family Medicine I - All Questions For Final and MidtermDocument64 pagesFamily Medicine I - All Questions For Final and Midtermzdfdgsdgsh sggaesgsNo ratings yet
- Biodex Biostep 2 ManualDocument28 pagesBiodex Biostep 2 ManualCzar BidNo ratings yet
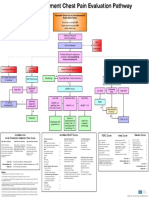
- Emergency Department Chest Pain Evaluation PathwayDocument2 pagesEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidNo ratings yet
- (:875 (: "M FlyerDocument1 page(:875 (: "M FlyerFsNo ratings yet
- High Sensitivity Cardiac Troponin T Increases After STR - 2019 - Clinical BiocheDocument6 pagesHigh Sensitivity Cardiac Troponin T Increases After STR - 2019 - Clinical BiocheFrankenstein MelancholyNo ratings yet
- Congenital Heart DiseaseDocument43 pagesCongenital Heart DiseaseSanjanaNo ratings yet
- 28,29 Management of Cardiac ArrhythmiasDocument41 pages28,29 Management of Cardiac ArrhythmiasSL Dr ChEMiSNo ratings yet
- Pathophysiology of Cardiogenic Pulmonary Edema - UpToDateDocument14 pagesPathophysiology of Cardiogenic Pulmonary Edema - UpToDateStefani AtlleNo ratings yet
- IschemicheartdiseaseDocument11 pagesIschemicheartdiseaseZaimon MaulionNo ratings yet
- Teacher'S Health Card: M SingleDocument3 pagesTeacher'S Health Card: M SingleNathaniel AlobaNo ratings yet
- Sympathetic Agonist and Antagonist 23Document12 pagesSympathetic Agonist and Antagonist 23PNo ratings yet
- Catalogue Catalogue: People - Health.CareDocument24 pagesCatalogue Catalogue: People - Health.Careiffat hanifNo ratings yet