You might also like
- GaugesDocument33 pagesGaugesUsman ansarNo ratings yet
- Geotecnical Limit State AustralianDocument6 pagesGeotecnical Limit State Australianprashanth c.nNo ratings yet
- A Modified Functionally Generated Path Technique FGP For Making Posterior Unit Metal Ceramic Crown PDFDocument8 pagesA Modified Functionally Generated Path Technique FGP For Making Posterior Unit Metal Ceramic Crown PDFDrRanjeet Kumar ChaudharyNo ratings yet
- 3d Printing in Fixed ProsthodonticsDocument5 pages3d Printing in Fixed ProsthodonticsCherifNo ratings yet
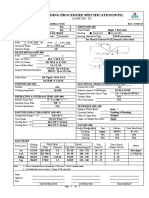
- Welding Procedure Specification (WPS) : (Asme Sec. Ix)Document1 pageWelding Procedure Specification (WPS) : (Asme Sec. Ix)Ahmed Lepda100% (1)
- Start DateDocument2 pagesStart DateHussainNo ratings yet
- Digital Dentistry and Digital ImpressionsDocument117 pagesDigital Dentistry and Digital ImpressionsAnonymous 0pg1qSpONo ratings yet
- Clinical Applications of Digital Dental TechnologyFrom EverandClinical Applications of Digital Dental TechnologyRadi MasriNo ratings yet
- Soil Testing Report 20170711 PDFDocument82 pagesSoil Testing Report 20170711 PDFvijayarajrameshNo ratings yet
- Comparacion Del Ajuste MarginalDocument6 pagesComparacion Del Ajuste MarginalXiomara Reyes palominoNo ratings yet
- Impresion CerámicaDocument15 pagesImpresion Cerámicacarlos andres giraldoNo ratings yet
- Articulo Medit 2023Document6 pagesArticulo Medit 2023Nancy LópezNo ratings yet
- Impresiones 3DDocument9 pagesImpresiones 3DDeyvi Emerson Rivas ZarateNo ratings yet
- JCM 09 03984Document8 pagesJCM 09 03984Zaharia NedealcovNo ratings yet
- Ing. Serag M. A Comparative Study of The Accuracy of Dies Made From Digital IntraDocument6 pagesIng. Serag M. A Comparative Study of The Accuracy of Dies Made From Digital IntraBavilonia K PaolaNo ratings yet
- Ear ProsthesisDocument6 pagesEar ProsthesisSkAliHassan100% (1)
- 3D Printing - An Alternative of Conventional Crown Fabrication A Case ReportDocument7 pages3D Printing - An Alternative of Conventional Crown Fabrication A Case ReportBalavigneshwaran bt18ipf04No ratings yet
- Evaluation of The Accuracy of Digital and 3d-Printed Casts Compared With Conventional Stone CastsDocument7 pagesEvaluation of The Accuracy of Digital and 3d-Printed Casts Compared With Conventional Stone CastsAlfred OrozcoNo ratings yet
- Comparison of Accuracy Between A Conventional and Two Digital Intraoral Impression TechniquesDocument7 pagesComparison of Accuracy Between A Conventional and Two Digital Intraoral Impression TechniquesDiego LopezNo ratings yet
- 1 s2.0 S0022391322006904 MainDocument8 pages1 s2.0 S0022391322006904 MainceramicameoNo ratings yet
- 1 s2.0 S002239132030562X MainDocument4 pages1 s2.0 S002239132030562X MainDANTE DELEGUERYNo ratings yet
- Sim 2018Document7 pagesSim 2018Bear BunnyNo ratings yet
- 2020 JPDDocument5 pages2020 JPDLuis Felipe SchneiderNo ratings yet
- CAD CAM Hybrid Hyrax, AJO - PDF - BenedictDocument6 pagesCAD CAM Hybrid Hyrax, AJO - PDF - BenedictCassiana SilvaNo ratings yet
- Trueness of CADCAM Digitization With ADocument14 pagesTrueness of CADCAM Digitization With ABedah Mulut dan Maksilofasial 2023No ratings yet
- Case Report Implant Planning SurgeryDocument8 pagesCase Report Implant Planning SurgeryPrita HapsariNo ratings yet
- 25 Gianetti2022Document8 pages25 Gianetti2022jessicajacovetti1No ratings yet
- 1 s2.0 S0300571223000684 MainDocument8 pages1 s2.0 S0300571223000684 MainFlávia de Souza BastosNo ratings yet
- Comparing The Accuracy Trueness and Precision of Models of Fixed Dental Prostheses Fabricated by Digital and Conventional Workflows 2019Document6 pagesComparing The Accuracy Trueness and Precision of Models of Fixed Dental Prostheses Fabricated by Digital and Conventional Workflows 2019ANDREA LOZANO CAMPOSNo ratings yet
- Fabricating Complete Dentures With CAD/CAM Technology: A B C DDocument5 pagesFabricating Complete Dentures With CAD/CAM Technology: A B C DPaulusMetehNo ratings yet
- Precision and Accuracy of A Digital Impression Scanner in Full-Arch Implant RehabilitationDocument5 pagesPrecision and Accuracy of A Digital Impression Scanner in Full-Arch Implant Rehabilitationgeorgios031No ratings yet
- Ijp 4835Document8 pagesIjp 4835Vishal SharmaNo ratings yet
- Jced 13 E487Document6 pagesJced 13 E487Rafaela VillamaguaNo ratings yet
- Intraoral Scanning To Fabricate Complete Dentures With Functional Borders: A Proof-Of-Concept Case ReportDocument7 pagesIntraoral Scanning To Fabricate Complete Dentures With Functional Borders: A Proof-Of-Concept Case ReportVeronica Regina RosselleNo ratings yet
- Comparison of Repeatability Between Intraoral Digital Scanner and Extraoral Digital Scanner An Invitro Study.Document7 pagesComparison of Repeatability Between Intraoral Digital Scanner and Extraoral Digital Scanner An Invitro Study.Alex BurdeNo ratings yet
- Mafe AnexoDocument7 pagesMafe AnexoGABRIELA NIETO GONZALEZNo ratings yet
- 10 1016@j Prosdent 2016 08 036Document7 pages10 1016@j Prosdent 2016 08 036José Carlos Herrera IbarraNo ratings yet
- Materials 14 01550Document13 pagesMaterials 14 01550marcela fajardoNo ratings yet
- APRD - 2 (2) - 33-36 (B)Document4 pagesAPRD - 2 (2) - 33-36 (B)Nur Syfa MufidhahNo ratings yet
- 10 1016@j Prosdent 2017 06 019-2Document6 pages10 1016@j Prosdent 2017 06 019-2Paulina Vargas DíazNo ratings yet
- Evaluation of Fit For 3d-Printed Retainers Compared With Thermoform RetainersDocument8 pagesEvaluation of Fit For 3d-Printed Retainers Compared With Thermoform RetainersDr.Prakher SainiNo ratings yet
- Digital Versus Conventional Impressions in Fixed Prosthodontics: A ReviewDocument7 pagesDigital Versus Conventional Impressions in Fixed Prosthodontics: A Reviewruthy arias anahuaNo ratings yet
- Piedra 2018 Digitalworkflowforthedesignandadditivelymanufactureofasplintedframeworkandcustomtrayfortheimpressionofmultipleimplants Adentaltechnique JPDDocument8 pagesPiedra 2018 Digitalworkflowforthedesignandadditivelymanufactureofasplintedframeworkandcustomtrayfortheimpressionofmultipleimplants Adentaltechnique JPDUmesh ChauhanNo ratings yet
- Guth Et Al 2013Document8 pagesGuth Et Al 2013João BotelhoNo ratings yet
- Trueness Analysis of Zirconia Crowns Fabricated With 3d PrintingDocument7 pagesTrueness Analysis of Zirconia Crowns Fabricated With 3d PrintingAlex BurdeNo ratings yet
- Virtual Evaluation For CAD-CAM-fabricated Complete DenturesDocument6 pagesVirtual Evaluation For CAD-CAM-fabricated Complete DenturesDanny Eduardo RomeroNo ratings yet
- CAD-CAM Milled Versus Rapidly Prototyped (3d-Printed) Complete Dentures: An in Vitro Evaluation of TruenessDocument7 pagesCAD-CAM Milled Versus Rapidly Prototyped (3d-Printed) Complete Dentures: An in Vitro Evaluation of TruenessAkshayaa BalajiNo ratings yet
- 784 2009 Article 291Document8 pages784 2009 Article 291EddieLee VeraNo ratings yet
- CAD/CAM Produces Dentures With Improved FitDocument7 pagesCAD/CAM Produces Dentures With Improved FitAkshayaa BalajiNo ratings yet
- Digital Work Ow For Image-Guided Immediate Implant Placement by Using The Socket-Shield Technique and Custom Abutment in The Esthetic AreaDocument5 pagesDigital Work Ow For Image-Guided Immediate Implant Placement by Using The Socket-Shield Technique and Custom Abutment in The Esthetic AreaEduin GiraldoNo ratings yet
- Accuracy of CAD-CAM-fabricated Removable Partial Dentures: Research andDocument7 pagesAccuracy of CAD-CAM-fabricated Removable Partial Dentures: Research andHelena VenanteNo ratings yet
- Precision and Trueness of Dental Models Manufactured With Different 3-Dimensional Printing TechniquesDocument10 pagesPrecision and Trueness of Dental Models Manufactured With Different 3-Dimensional Printing TechniquesMonojit DuttaNo ratings yet
- Uso de Sistemas de Impresion Digital Con Scaners Intraorales para Fabricacion de Protesis FijaDocument7 pagesUso de Sistemas de Impresion Digital Con Scaners Intraorales para Fabricacion de Protesis FijaPaola Alexandra LaguadoNo ratings yet
- Art 2Document6 pagesArt 2Florin Eugen ConstantinescuNo ratings yet
- Are Different Generations of CAD/CAM Milling Machines Capable To Produce Restorations With Similar Quality?Document6 pagesAre Different Generations of CAD/CAM Milling Machines Capable To Produce Restorations With Similar Quality?Deyvi Emerson Rivas ZarateNo ratings yet
- Van Der Meer-2012-Application of Intra-Oral de PDFDocument8 pagesVan Der Meer-2012-Application of Intra-Oral de PDFAdinaBicaNo ratings yet
- Creacion de Un Archivo de Dentadura Total Digital, Una Tecnica DentalDocument5 pagesCreacion de Un Archivo de Dentadura Total Digital, Una Tecnica DentalPaola Alexandra LaguadoNo ratings yet
- Dynamic Designing of Dental Prostheses: International Design Conference - Design 2016Document6 pagesDynamic Designing of Dental Prostheses: International Design Conference - Design 2016Nenad BojceticNo ratings yet
- Accuracy in The Digital Work Ow: From Data Acquisition To The Digitally Milled CastDocument6 pagesAccuracy in The Digital Work Ow: From Data Acquisition To The Digitally Milled Castmarianaduque82No ratings yet
- Journal of Prosthodontic Research: Hirotaka Nishiyama, Asuka Taniguchi, Shinpei Tanaka, Kazuyoshi BabaDocument6 pagesJournal of Prosthodontic Research: Hirotaka Nishiyama, Asuka Taniguchi, Shinpei Tanaka, Kazuyoshi BabaPriscilia YovianiNo ratings yet
- PAPER BY DR CKB NAIR Dental BarsDocument8 pagesPAPER BY DR CKB NAIR Dental BarsDr CKB NairNo ratings yet
- Comparison of Denture Base Adaptation Between CAD/CAM and Conventional Fabrication TechniquesDocument8 pagesComparison of Denture Base Adaptation Between CAD/CAM and Conventional Fabrication TechniquesVictor LappostNo ratings yet
- 10 1016@j Joen 2018 11 006 PDFDocument5 pages10 1016@j Joen 2018 11 006 PDFVijithNo ratings yet
- Three-Dimensional Assessment of Virtual Bracket Removal For Orthodontic Retainers: A Prospective Clinical StudyDocument10 pagesThree-Dimensional Assessment of Virtual Bracket Removal For Orthodontic Retainers: A Prospective Clinical StudyAndré DrumondNo ratings yet
- Direct Mechanical Data Acquisition of Dental Impressions For The Manufacturing of CAD-CAM RestorationsDocument6 pagesDirect Mechanical Data Acquisition of Dental Impressions For The Manufacturing of CAD-CAM RestorationsAlex BurdeNo ratings yet
- 65 - JPR - D - 20 - 00169 - 1Document7 pages65 - JPR - D - 20 - 00169 - 1Gt SolarcNo ratings yet
- Tutorial 5 - Flexural Members - Lateral Torsional BucklingDocument32 pagesTutorial 5 - Flexural Members - Lateral Torsional BucklingChan Keng ChunNo ratings yet
- ITC Johnston Complete Family Pack Font ListDocument2 pagesITC Johnston Complete Family Pack Font ListSenthuTu0% (1)
- Mouthwash, PEG, Sulfate, Betaine FreeDocument2 pagesMouthwash, PEG, Sulfate, Betaine FreerekhilaNo ratings yet
- 4aa4 1063enwDocument8 pages4aa4 1063enwHenderson and SantosNo ratings yet
- Catalogue of Jumbo: Jumbo Power Technology Co.,LimitedDocument20 pagesCatalogue of Jumbo: Jumbo Power Technology Co.,LimitedJosé Daniel Interventoria AP MocoaNo ratings yet
- A Study On Customer Awareness and Satisfaction Towards Flipkart Shopping - With Special Reference To Pollachi TalukDocument4 pagesA Study On Customer Awareness and Satisfaction Towards Flipkart Shopping - With Special Reference To Pollachi TalukMukul SomgadeNo ratings yet
- Endodontic and Restorative Management of A Lower Molar With A Calcified Pulp Chamber.Document7 pagesEndodontic and Restorative Management of A Lower Molar With A Calcified Pulp Chamber.Nicolas SantanderNo ratings yet
- Reasearch ProposalDocument9 pagesReasearch Proposalamel amoulaNo ratings yet
- Rocna and Vulcan Anchor DimensionsDocument2 pagesRocna and Vulcan Anchor DimensionsJoseph PintoNo ratings yet
- Unit II Evolution of TQMDocument36 pagesUnit II Evolution of TQMsbmallurNo ratings yet
- Ebook Sobotta Atlas of Anatomy Vol 1 General Anatomy and Musculoskeletal System English Latin16Th Ed PDF Full Chapter PDFDocument68 pagesEbook Sobotta Atlas of Anatomy Vol 1 General Anatomy and Musculoskeletal System English Latin16Th Ed PDF Full Chapter PDFkarren.brown188100% (25)
- Pedagogy MCQsDocument85 pagesPedagogy MCQsPrasanna KumarNo ratings yet
- LP Science2 q2w5Document7 pagesLP Science2 q2w5Gaila Mae Abejuela SanorjoNo ratings yet
- Case-Friedland Timbers CompanyDocument2 pagesCase-Friedland Timbers Companytalented guy0% (1)
- CFA Level I - Timetable (August 2021 Exam) (V2)Document1 pageCFA Level I - Timetable (August 2021 Exam) (V2)Via Commerce Sdn BhdNo ratings yet
- Revealed Comparative AdvantageDocument5 pagesRevealed Comparative AdvantageiamrahulkumarNo ratings yet
- Simulación de Eventos Discretos Eduardo García Dunna May 4, 2015Document22 pagesSimulación de Eventos Discretos Eduardo García Dunna May 4, 2015Andrea GutierrezNo ratings yet
- Delta Background-Group AssignmentDocument2 pagesDelta Background-Group AssignmentTinashe100% (2)
- OTPBank Securities SI 20210217Document6 pagesOTPBank Securities SI 20210217bdsourav0No ratings yet
- AION 7.9 Part2 PatchNotes ENDocument10 pagesAION 7.9 Part2 PatchNotes ENRosaArandaNo ratings yet
- International Journal of Transportation Science and TechnologyDocument11 pagesInternational Journal of Transportation Science and TechnologyIrvin SmithNo ratings yet
- Tesla - Tunguska Explosion 1908 PDFDocument9 pagesTesla - Tunguska Explosion 1908 PDFMircea Gabriel BalanNo ratings yet
- Panasonic SC BT200Document60 pagesPanasonic SC BT200Mark CoatesNo ratings yet
- Plains Cotton Coop Ass'n V Goodpasture Computer Service, Inc, 807 F 2d 1256Document9 pagesPlains Cotton Coop Ass'n V Goodpasture Computer Service, Inc, 807 F 2d 1256gesmerNo ratings yet