You might also like
- Short Textbook of Endodontics: AbcdeDocument7 pagesShort Textbook of Endodontics: AbcdeCristinaNo ratings yet
- 03 Principles of Coronal Access Cavity PreparationDocument5 pages03 Principles of Coronal Access Cavity PreparationRamiz FareedNo ratings yet
- 4 - Access Cavity of Anterior Teeth 2022Document48 pages4 - Access Cavity of Anterior Teeth 2022mrbyy619No ratings yet
- ACCESS CAVITY PREPARATION AnjaliDocument69 pagesACCESS CAVITY PREPARATION Anjalianjali sNo ratings yet
- ثDocument40 pagesثZakria Al-HadadNo ratings yet
- Access Cavity Preparation in Anterior TeethDocument18 pagesAccess Cavity Preparation in Anterior TeethRahul KumarNo ratings yet
- Department of Conservative Dentistry: Presented By: Nikita GoyalDocument27 pagesDepartment of Conservative Dentistry: Presented By: Nikita GoyalAnkita GoyalNo ratings yet
- Guide For Practical Steps-Access Opening For Anterior TeethDocument12 pagesGuide For Practical Steps-Access Opening For Anterior Teethabdul rahman mohammed salehNo ratings yet
- Access CavityDocument41 pagesAccess CavityAndra GhiranNo ratings yet
- Access Cavity Preparation FinalDocument63 pagesAccess Cavity Preparation Finalrasagna reddyNo ratings yet
- Fundamentals of Cavity PreparationsDocument77 pagesFundamentals of Cavity PreparationsAlloo Osama Awsi100% (2)
- Class I Cavity Preparation For Amalgam Restoration: Prepared By: DR. Afnan ElwadiaDocument74 pagesClass I Cavity Preparation For Amalgam Restoration: Prepared By: DR. Afnan ElwadiaAssssssNo ratings yet
- Access Cavity Preparation: Dr. Ahmed NegmDocument55 pagesAccess Cavity Preparation: Dr. Ahmed NegmSantika IndahsariNo ratings yet
- Endo Access Cavity Preparation 5Document176 pagesEndo Access Cavity Preparation 5ahead1234No ratings yet
- 3-Access Cavity Preparation PDFDocument60 pages3-Access Cavity Preparation PDFAllisyia MalauNo ratings yet
- Access Opening Preparation: EndodonticsDocument10 pagesAccess Opening Preparation: Endodonticsكاظم عبد الحسينNo ratings yet
- Definition of Cavity PreparationDocument76 pagesDefinition of Cavity PreparationDaniel AryanNo ratings yet
- L2. Tooth Morphology and Access OpeningsDocument6 pagesL2. Tooth Morphology and Access OpeningsUnghianu Constantin IulianNo ratings yet
- Class I Cavity Preparation-2Document43 pagesClass I Cavity Preparation-2معاذ نوري محمدNo ratings yet
- Endodontic coronal cavity preparation outlineDocument14 pagesEndodontic coronal cavity preparation outlinemahaNo ratings yet
- Occlusal Cavity Definition and DesignDocument51 pagesOcclusal Cavity Definition and DesignWael RaafatNo ratings yet
- Access Cavity Preparation An Anatomical and Clinical Perspective June 2011Document10 pagesAccess Cavity Preparation An Anatomical and Clinical Perspective June 2011Eri Lupitasari100% (1)
- Class V Amalgam CavityDocument65 pagesClass V Amalgam CavitySoham D PrajapatiNo ratings yet
- انو محاضرة ثانية اسنان ذي قارDocument12 pagesانو محاضرة ثانية اسنان ذي قارhaider yahyaNo ratings yet
- Access Cavity For EndodonticsDocument5 pagesAccess Cavity For EndodonticsAhmed AbozaidNo ratings yet
- Access Opening Chapter 5Document17 pagesAccess Opening Chapter 5misdduaaNo ratings yet
- Adts Guidelines For Access CavityDocument7 pagesAdts Guidelines For Access Cavityrojek63No ratings yet
- Access Cavity Preparation PDFDocument46 pagesAccess Cavity Preparation PDFNandithaNair100% (2)
- Intro to Endodontic TreatmentDocument18 pagesIntro to Endodontic TreatmentGareth DoodyNo ratings yet
- Cavity PrepDocument10 pagesCavity PrepShruti GolaiNo ratings yet
- Access Cavity Preparation: Lecture ThreeDocument17 pagesAccess Cavity Preparation: Lecture ThreeAli UmarNo ratings yet
- Curse 3Document53 pagesCurse 3Nia AdibNo ratings yet
- Class V Amalgam CavityDocument65 pagesClass V Amalgam CavityJasper Tan Min ZhenNo ratings yet
- Endo Access Cavity PrepDocument57 pagesEndo Access Cavity PrepConnie K AmakaliNo ratings yet
- Intracoronal Restorations in FPDDocument60 pagesIntracoronal Restorations in FPDChandni SetiaNo ratings yet
- ACCESS CAVITY PREPARATION GUIDELINESDocument35 pagesACCESS CAVITY PREPARATION GUIDELINESShaheen Aboobacker Reniya ShaheenNo ratings yet
- Endo Pre FinalsDocument18 pagesEndo Pre FinalsRayne Gelle100% (2)
- Endo Access Cavity PreparationDocument61 pagesEndo Access Cavity PreparationGabi Cosmin50% (6)
- Amalgam Cavity Preparation Class 1Document51 pagesAmalgam Cavity Preparation Class 1Hadil Altilbani100% (1)
- Conservative Dentistry: Classification of CavityDocument12 pagesConservative Dentistry: Classification of Cavityنور الحلوهNo ratings yet
- Endo 2 PDFDocument5 pagesEndo 2 PDFNabila RizkikaNo ratings yet
- Class VDocument37 pagesClass VyahyaNo ratings yet
- Amalgam RestorationsDocument75 pagesAmalgam RestorationsGaddafi HamzaNo ratings yet
- A Practical Guide To Endodontic Access Cavity PrepDocument19 pagesA Practical Guide To Endodontic Access Cavity PrepRajeev GargNo ratings yet
- 2 Principles of Access PrepDocument24 pages2 Principles of Access Prepmrbyy619No ratings yet
- Class V Amalgam CavityDocument38 pagesClass V Amalgam CavityAbdur RehmanNo ratings yet
- Introduction +morphology PDFDocument201 pagesIntroduction +morphology PDFbadr abdelkaderNo ratings yet
- Endodontic mishaps prevention and managementDocument29 pagesEndodontic mishaps prevention and managementYomna NimerNo ratings yet
- BDS 8126 Access To AnteriorsDocument73 pagesBDS 8126 Access To AnteriorsNouraHabiba28No ratings yet
- 6 - Access Cavity of Premolars 2022Document24 pages6 - Access Cavity of Premolars 2022mrbyy619No ratings yet
- Endodontic Cavity PreparationDocument166 pagesEndodontic Cavity Preparationagusaranp0% (1)
- Periodontic seminar (Recovered)Document16 pagesPeriodontic seminar (Recovered)Eng BeboNo ratings yet
- Amalgam Rastorations: Outline FormDocument5 pagesAmalgam Rastorations: Outline FormALI abd-alamamNo ratings yet
- Interceptive Orthodontics: A Practical Guide to Occlusal ManagementFrom EverandInterceptive Orthodontics: A Practical Guide to Occlusal ManagementNo ratings yet
- Clinical Cases in Restorative and Reconstructive DentistryFrom EverandClinical Cases in Restorative and Reconstructive DentistryRating: 5 out of 5 stars5/5 (1)
- World Cup Generates Billions in RevenueDocument20 pagesWorld Cup Generates Billions in RevenueCristinaNo ratings yet
- MlcrsDocument4 pagesMlcrsCristinaNo ratings yet
- UdalipaDocument4 pagesUdalipaCristinaNo ratings yet
- SLNGMZDocument10 pagesSLNGMZCristinaNo ratings yet
- JSTBBDocument5 pagesJSTBBCristinaNo ratings yet
- Stifturi DiferiteDocument13 pagesStifturi DiferiteCristinaNo ratings yet
- Chlorine Oxidation States and OxoacidsDocument11 pagesChlorine Oxidation States and OxoacidsCristinaNo ratings yet
- Sem 3Document11 pagesSem 3CristinaNo ratings yet
- WKNDDocument10 pagesWKNDCristinaNo ratings yet
- Sem 2Document7 pagesSem 2CristinaNo ratings yet
- Everything about stainless steel in 38 charactersDocument6 pagesEverything about stainless steel in 38 charactersCristinaNo ratings yet
- MesiahDocument18 pagesMesiahCristinaNo ratings yet
- GuavaDocument8 pagesGuavaCristinaNo ratings yet
- Acryl 7Document6 pagesAcryl 7CristinaNo ratings yet
- Acryl 3Document11 pagesAcryl 3CristinaNo ratings yet
- Classifying Wounds and Blood Vessel TypesDocument4 pagesClassifying Wounds and Blood Vessel TypesCristinaNo ratings yet
- KednrikDocument6 pagesKednrikCristinaNo ratings yet
- Acryl 6Document7 pagesAcryl 6CristinaNo ratings yet
- Reducing alcohol abuse stigma to improve treatmentDocument10 pagesReducing alcohol abuse stigma to improve treatmentCristinaNo ratings yet
- MigosDocument5 pagesMigosCristinaNo ratings yet
- OffsetDocument8 pagesOffsetCristinaNo ratings yet
- IndexeniDocument4 pagesIndexeniCristinaNo ratings yet
- BaliDocument10 pagesBaliCristinaNo ratings yet
- MangoDocument4 pagesMangoCristinaNo ratings yet
- ProtozoareDocument7 pagesProtozoareCristinaNo ratings yet
- JcoleDocument11 pagesJcoleCristinaNo ratings yet
- MrnightmaDocument5 pagesMrnightmaCristinaNo ratings yet
- CornfornDocument6 pagesCornfornCristinaNo ratings yet
- AmeobaDocument4 pagesAmeobaCristinaNo ratings yet
- Cotton 22Document10 pagesCotton 22CristinaNo ratings yet
- Brochure Mini BooklerDocument12 pagesBrochure Mini BooklerPT. Magnus Indo MedikaNo ratings yet
- מצגת מערכת עיכולDocument74 pagesמצגת מערכת עיכולnataliya36No ratings yet
- Resume: DR Dulla Rahul Krishna Provisional Registration No. APMC/FMR/108392 PH No. 8886036236Document3 pagesResume: DR Dulla Rahul Krishna Provisional Registration No. APMC/FMR/108392 PH No. 8886036236T.S.ayuduNo ratings yet
- Paranasal Sinus Anatomy - Overview, Gross Anatomy, Microscopic AnatomyDocument12 pagesParanasal Sinus Anatomy - Overview, Gross Anatomy, Microscopic AnatomyKienlevy100% (1)
- Craniotomy: AngiographyDocument3 pagesCraniotomy: AngiographyyogieNo ratings yet
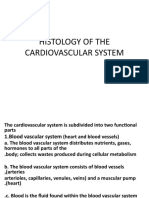
- Histology of The Cardiovascular System#Document36 pagesHistology of The Cardiovascular System#DonaldNo ratings yet
- Trauma DuodenalDocument5 pagesTrauma Duodenalpancholin_9No ratings yet
- Presentation VVFDocument60 pagesPresentation VVFMairmon KhanNo ratings yet
- Perioperative Nursing Care IssuesDocument7 pagesPerioperative Nursing Care IssuesAziil LiizaNo ratings yet
- Modul Saccrum and CoxigeusDocument7 pagesModul Saccrum and Coxigeusmazidah fauziyyah24No ratings yet
- By: Jacqueline I. Esmundo, R.N.MNDocument28 pagesBy: Jacqueline I. Esmundo, R.N.MNdomlhynNo ratings yet
- An Interesting Case of Gluteal Swelling - Intramuscular Myxoma (IMM) by DR Zothansanga ZadengDocument3 pagesAn Interesting Case of Gluteal Swelling - Intramuscular Myxoma (IMM) by DR Zothansanga ZadengCJ MazualaNo ratings yet
- Shoulder CodeDocument2 pagesShoulder CodeNasfikurNo ratings yet
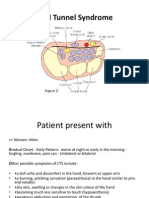
- Carpal Tunnel Syndrome Power Point PresentationDocument6 pagesCarpal Tunnel Syndrome Power Point Presentationapi-237061134No ratings yet
- Severe Acute Mitral Valve Regurgitation in A COVID-19 - Infected PatientDocument6 pagesSevere Acute Mitral Valve Regurgitation in A COVID-19 - Infected Patientkamel salemNo ratings yet
- Acls PDFDocument53 pagesAcls PDFKeez HaruNo ratings yet
- International Journal of Surgery Case ReportsDocument4 pagesInternational Journal of Surgery Case ReportsFhy Ghokiel AbiezNo ratings yet
- Postoperative Nausea and VomitingDocument45 pagesPostoperative Nausea and Vomitingprem kotiNo ratings yet
- Solitaire FR BrochureDocument2 pagesSolitaire FR Brochuredsk778894No ratings yet
- DVT DR Moses KazeevuDocument24 pagesDVT DR Moses KazeevuMoses Jr KazevuNo ratings yet
- MAY RECALL 2021: ELDERLY WOMAN WITH CONFUSION LIKELY HAS DELIRIUMDocument47 pagesMAY RECALL 2021: ELDERLY WOMAN WITH CONFUSION LIKELY HAS DELIRIUMschool adressNo ratings yet
- Treatment Analysis of Acute ParaproctitisDocument4 pagesTreatment Analysis of Acute ParaproctitisCentral Asian StudiesNo ratings yet
- The Skeletal SystemDocument3 pagesThe Skeletal SystemMiguel GumatayNo ratings yet
- Superficial Thinning of The DIEP Flap A Safe.6Document5 pagesSuperficial Thinning of The DIEP Flap A Safe.6noskovNo ratings yet
- UW Health Job for Endoscopy TechnicianDocument2 pagesUW Health Job for Endoscopy TechnicianAnupam KumarNo ratings yet
- Post-Op Eye Care InstructionsDocument1 pagePost-Op Eye Care InstructionsProtip SinhaNo ratings yet
- HemostasisDocument23 pagesHemostasisSwathi BNo ratings yet
- Pacemakers, Cardiac, External, Noninvasive Electrodes Invasive Electrodes, TransesophagealDocument10 pagesPacemakers, Cardiac, External, Noninvasive Electrodes Invasive Electrodes, TransesophagealKevin RubioNo ratings yet
- Full download book Chapman Nakielnys Guide To Radiological Procedures Pdf pdfDocument41 pagesFull download book Chapman Nakielnys Guide To Radiological Procedures Pdf pdfmaureen.fine870100% (14)
- Repair Cornea SuturesDocument14 pagesRepair Cornea SuturesBima RizkiNo ratings yet