You might also like
- Landman Training ManualDocument34 pagesLandman Training Manualflashanon100% (2)
- Dennis McGuire: Mental Wellness and Good Health in Teens and Adults With Down SyndromeDocument23 pagesDennis McGuire: Mental Wellness and Good Health in Teens and Adults With Down SyndromeGlobalDownSyndromeNo ratings yet
- ADHD Conners Self-Report TeenDocument3 pagesADHD Conners Self-Report TeenLisa HernandezNo ratings yet
- Mechanisms of Change in Prolonged Exposure Therapy For PTSD-Implications For Clinical PracticeDocument9 pagesMechanisms of Change in Prolonged Exposure Therapy For PTSD-Implications For Clinical PracticeKelly GCNo ratings yet
- Clinical Global Impression-Bipolar (Cgi-Bp)Document2 pagesClinical Global Impression-Bipolar (Cgi-Bp)abhilasha8dwivediNo ratings yet
- 1983 - The Brief Symptom Inventory, An Introductory ReportDocument11 pages1983 - The Brief Symptom Inventory, An Introductory ReportBogdan BaceanuNo ratings yet
- (Tdah) ADD-AdultQ by Jasper&GoldbergDocument2 pages(Tdah) ADD-AdultQ by Jasper&GoldbergJohn Steppenwolf100% (1)
- Autistic Intelligence: Interaction, Individuality, and the Challenges of DiagnosisFrom EverandAutistic Intelligence: Interaction, Individuality, and the Challenges of DiagnosisNo ratings yet
- The Identification of Autistic Adults’ Perception of Their Own Diagnostic Pathway: A Research Dissertation Submitted for the Degree of Master of Autism at Sheffield Hallam UniversityFrom EverandThe Identification of Autistic Adults’ Perception of Their Own Diagnostic Pathway: A Research Dissertation Submitted for the Degree of Master of Autism at Sheffield Hallam UniversityNo ratings yet
- 240-Item Personality Inventory UncoveredDocument8 pages240-Item Personality Inventory UncoveredDeepa Dutt100% (1)
- Autism PDFDocument41 pagesAutism PDFflower21No ratings yet
- Coventry Grid Interview (CGI)Document20 pagesCoventry Grid Interview (CGI)Aliens-and-antsNo ratings yet
- The Autism-Spectrum Quotient (AQ) : Evidence From Asperger Syndrome/High-Functioning Autism, Males and Females, Scientists and MathematiciansDocument13 pagesThe Autism-Spectrum Quotient (AQ) : Evidence From Asperger Syndrome/High-Functioning Autism, Males and Females, Scientists and MathematiciansDamian Maya0% (1)
- An Update On The Comorbidity of ADHD and ASDDocument16 pagesAn Update On The Comorbidity of ADHD and ASDCristina SolerNo ratings yet
- ASC1Document17 pagesASC1AndyBrookeNo ratings yet
- JoDD 17-1 26-37 Schroeder Et AlDocument12 pagesJoDD 17-1 26-37 Schroeder Et AlEspíritu CiudadanoNo ratings yet
- Autism 07april 2019Document26 pagesAutism 07april 2019هلا دلبحNo ratings yet
- Emotional CPR - AustraliaDocument1 pageEmotional CPR - AustraliaSharon A Stocker0% (1)
- Self-Regulation Assessment ScaleDocument2 pagesSelf-Regulation Assessment Scaleapi-383607481No ratings yet
- Autism Spectrum DisorderDocument58 pagesAutism Spectrum DisorderPriscilla ChumrooNo ratings yet
- Standards of Diagnostic Assessment For Autism Spectrum DisorderDocument8 pagesStandards of Diagnostic Assessment For Autism Spectrum DisorderLoreto Opazo RojasNo ratings yet
- Bipolar Disorder Assessment and Management 35109814379461Document49 pagesBipolar Disorder Assessment and Management 35109814379461Ana Maria Coral LeitonNo ratings yet
- Supporting Students With Challenging BehaviorsDocument4 pagesSupporting Students With Challenging Behaviorsapi-357465278No ratings yet
- Adhd - Asrs .ScreenDocument4 pagesAdhd - Asrs .ScreenKenth GenobisNo ratings yet
- Use of The ADOS and ADI-R in Children With PsychosisDocument25 pagesUse of The ADOS and ADI-R in Children With PsychosiscaristaNo ratings yet
- Detection of Bipolar Disorder BJP 2011 Young 3 4Document3 pagesDetection of Bipolar Disorder BJP 2011 Young 3 4Gede GiriNo ratings yet
- Autism Spectrum Disorder Friendly School Guidelines 2016Document11 pagesAutism Spectrum Disorder Friendly School Guidelines 2016Pudu MounikaNo ratings yet
- Adhd Psych AssessmentDocument13 pagesAdhd Psych AssessmentJoan G. Huyo-aNo ratings yet
- SchizophreniaDocument2 pagesSchizophreniaIT’S ME HAYLA100% (1)
- Relaxation Techiques For Test AnxietyDocument3 pagesRelaxation Techiques For Test AnxietySuzannah ArthurNo ratings yet
- ODD Quick Fact Sheet For Parents Guardians and Child Serving Professionals 2.24.14Document2 pagesODD Quick Fact Sheet For Parents Guardians and Child Serving Professionals 2.24.14narcis2009No ratings yet
- NIH Public AccessDocument23 pagesNIH Public AccessBárbara AndreaNo ratings yet
- Oxford Handbooks Online: Intellectual DisabilitiesDocument20 pagesOxford Handbooks Online: Intellectual DisabilitiesCristina100% (1)
- First Friday Presentation 2 3 23Document60 pagesFirst Friday Presentation 2 3 23api-339789222No ratings yet
- CARSDocument18 pagesCARSzarish.shireenNo ratings yet
- Emdr 2002Document14 pagesEmdr 2002jivinaNo ratings yet
- About Case Studies of ADHD in Childre1Document6 pagesAbout Case Studies of ADHD in Childre1PearlCladelLapidezNo ratings yet
- Interventions For Classroom DisruptionDocument54 pagesInterventions For Classroom DisruptionnosunarNo ratings yet
- Modified Coventry Model - Including PDA ProfileDocument13 pagesModified Coventry Model - Including PDA ProfileAliens-and-antsNo ratings yet
- Call To Mind - Dateless - Jasper Goldberg Adult ADD Screening Examination Version 5Document1 pageCall To Mind - Dateless - Jasper Goldberg Adult ADD Screening Examination Version 5Khoa Dang Truong0% (1)
- ADHD Scoring InstructionsDocument1 pageADHD Scoring Instructionsnaseeruddin1No ratings yet
- GARS 2 - ArticleDocument20 pagesGARS 2 - ArticleGoropadNo ratings yet
- Recording Consent FormDocument1 pageRecording Consent Form000766401No ratings yet
- Parenting - AsdDocument9 pagesParenting - Asdapi-391945267No ratings yet
- AngerDocument58 pagesAngerasdfNo ratings yet
- Pediatric Evaluation of Disability InventoryDocument1 pagePediatric Evaluation of Disability InventoryBacus Regina RoseNo ratings yet
- Child and AdolescentDocument59 pagesChild and AdolescentJaezNo ratings yet
- CatDocument12 pagesCatnini345No ratings yet
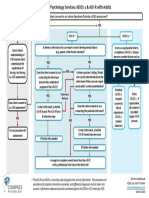
- Compass Psychology Services: ADOS-2 & ADI-R FlowchartDocument1 pageCompass Psychology Services: ADOS-2 & ADI-R Flowchartaspire centerNo ratings yet
- Acceptance and Commitment Therapy (ACT) As A Career Counseling StrategyDocument17 pagesAcceptance and Commitment Therapy (ACT) As A Career Counseling Strategydavid.settembrinoNo ratings yet
- Zaki & Williams (2013) - Interpersonal Emotion RegulationDocument9 pagesZaki & Williams (2013) - Interpersonal Emotion Regulationalessarpon7557No ratings yet
- DSM 5 Intellectual Disability Fact SheetDocument2 pagesDSM 5 Intellectual Disability Fact SheetMelissa Ortega MaguiñaNo ratings yet
- CBI-R Cambridge Behavioural InventoryDocument2 pagesCBI-R Cambridge Behavioural InventoryNikos AndronasNo ratings yet
- Attention Deficit/ Hyperactivity Disorder: Changes To The DisorderDocument2 pagesAttention Deficit/ Hyperactivity Disorder: Changes To The DisorderGemanDuenasNo ratings yet
- 2022-2023 Trauma Informed Care Microcredential Information BookletDocument12 pages2022-2023 Trauma Informed Care Microcredential Information Bookletapi-260883031100% (1)
- Panic DisorderDocument323 pagesPanic DisorderTabitha MuscasNo ratings yet
- Clinical GuidelineDocument86 pagesClinical GuidelineJae MedinaNo ratings yet
- TIPP WorksheetDocument2 pagesTIPP WorksheethddixonNo ratings yet
- Final Group Counseling Project - Stress ManagementDocument82 pagesFinal Group Counseling Project - Stress Managementapi-548101945No ratings yet
- M Torres Neuropsychological Report 5Document12 pagesM Torres Neuropsychological Report 5Reyna De AlbaNo ratings yet
- 10th IIT Foundation PDFDocument170 pages10th IIT Foundation PDFbondala pavan100% (1)
- USD - DPF Cleaning Machine - POSEYDON1000 - PolDocument8 pagesUSD - DPF Cleaning Machine - POSEYDON1000 - PolAbaidi RabieNo ratings yet
- Calculating Calories for Weight Training SuccessDocument12 pagesCalculating Calories for Weight Training SuccessFadil Arif MuhammadNo ratings yet
- VALUE BASED QUESTIONS FROM MATHEMATICS GRADE 10Document6 pagesVALUE BASED QUESTIONS FROM MATHEMATICS GRADE 10allyvluvyNo ratings yet
- Fabric Trademark and Brand Name IndexDocument15 pagesFabric Trademark and Brand Name Indexsukrat20No ratings yet
- Wiring Diagram Obp 1 v2Document5 pagesWiring Diagram Obp 1 v2Jorge Luis Vera AlmeidaNo ratings yet
- 2689 26489 1 PBDocument9 pages2689 26489 1 PBAntonio EspañaNo ratings yet
- Learning, Perception, Attitudes, Values, and Ethics: Fundamentals of Organizational Behavior 2eDocument21 pagesLearning, Perception, Attitudes, Values, and Ethics: Fundamentals of Organizational Behavior 2eJp AlvarezNo ratings yet
- Dictation TechniquesDocument12 pagesDictation TechniquesMuhamad IbrohimNo ratings yet
- Consumer Perception of Digital Payment Modes in IndiaDocument14 pagesConsumer Perception of Digital Payment Modes in Indiakarthick50% (2)
- 1967 Painting Israeli VallejoDocument1 page1967 Painting Israeli VallejoMiloš CiniburkNo ratings yet
- GES1003 AY1819 CLS Tutorial 1Document4 pagesGES1003 AY1819 CLS Tutorial 1AshwinNo ratings yet
- Microsoft Word BasicsDocument25 pagesMicrosoft Word Basicsitsudatte18No ratings yet
- Se Lab Da-2Document12 pagesSe Lab Da-2Anvesh PenkeNo ratings yet
- l3 Immunization & Cold ChainDocument53 pagesl3 Immunization & Cold ChainNur AinaaNo ratings yet
- Policy Based Routing On Fortigate FirewallDocument2 pagesPolicy Based Routing On Fortigate FirewalldanNo ratings yet
- Diesel Pump of The Desmi GroupDocument10 pagesDiesel Pump of The Desmi Groupngocdhxd92No ratings yet
- MSc Thesis on VAW in PhilippinesDocument100 pagesMSc Thesis on VAW in Philippineselma cutamoraNo ratings yet
- Prompt 2022Document12 pagesPrompt 2022cecilferrosNo ratings yet
- Emerson Field Tools Quick Start GuideDocument48 pagesEmerson Field Tools Quick Start Guidepks_2410No ratings yet
- OUM Human Anatomy Final Exam QuestionsDocument5 pagesOUM Human Anatomy Final Exam QuestionsAnandNo ratings yet
- Si Eft Mandate FormDocument1 pageSi Eft Mandate FormdSolarianNo ratings yet
- OOD ch11Document31 pagesOOD ch11Pumapana GamingNo ratings yet
- Teaching As Noble ProfessionDocument1 pageTeaching As Noble ProfessionJeric AcostaNo ratings yet
- Buckley V UkDocument12 pagesBuckley V UkShriya ChandankarNo ratings yet
- Villariba - Document Analysis - Jose RizalDocument2 pagesVillariba - Document Analysis - Jose RizalkrishaNo ratings yet
- DepEd Memorandum on SHS Curriculum MappingDocument8 pagesDepEd Memorandum on SHS Curriculum MappingMichevelli RiveraNo ratings yet
- MgstreamDocument2 pagesMgstreamSaiful ManalaoNo ratings yet
- Common Expressions in Business 2Document2 pagesCommon Expressions in Business 2abdeljelil manelNo ratings yet