You might also like
- Viral Hepatitis: Acute HepatitisFrom EverandViral Hepatitis: Acute HepatitisResat OzarasNo ratings yet
- The Worldwide Impact of Vaccination On The Control and Protection of Viral Hepatitis BDocument6 pagesThe Worldwide Impact of Vaccination On The Control and Protection of Viral Hepatitis BYle BravoNo ratings yet
- Hepatitis B Virus and Liver DiseaseFrom EverandHepatitis B Virus and Liver DiseaseJia-Horng KaoNo ratings yet
- Seminar: Christian Trépo, Henry L Y Chan, Anna LokDocument11 pagesSeminar: Christian Trépo, Henry L Y Chan, Anna LokGERALDINE JARAMILLO VARGASNo ratings yet
- mr1018 1 ch5Document21 pagesmr1018 1 ch5AkileshDhanushiyanNo ratings yet
- Immigration and Viral Hepatitis: Public HealthDocument8 pagesImmigration and Viral Hepatitis: Public HealthEdgar MejiaNo ratings yet
- Tentang World Hepatitis Day 2020Document8 pagesTentang World Hepatitis Day 2020YanMardianNo ratings yet
- Global Epidemiology of Hepatitis B Virus (HBV) Infection: Elizabeth W. Hwang, MD, Ramsey Cheung, MDDocument7 pagesGlobal Epidemiology of Hepatitis B Virus (HBV) Infection: Elizabeth W. Hwang, MD, Ramsey Cheung, MDivan gartikaNo ratings yet
- Epidemiology, Transmission, and Prevention of Hepatitis B Virus InfectionDocument20 pagesEpidemiology, Transmission, and Prevention of Hepatitis B Virus Infectionmayteveronica1000No ratings yet
- Hepatology - 2004 - Major - The Molecular Virology of Hepatitis CDocument21 pagesHepatology - 2004 - Major - The Molecular Virology of Hepatitis CEngr Hafiz Qasim AliNo ratings yet
- BHBHBHBHBHBHBHBHBHBHBHB HHBHDocument14 pagesBHBHBHBHBHBHBHBHBHBHBHB HHBHbubble_inNo ratings yet
- Immigration and Viral Hepatitis: Public HealthDocument8 pagesImmigration and Viral Hepatitis: Public HealthFenny Noor AidaNo ratings yet
- Hepatitis A-PrintDocument17 pagesHepatitis A-PrintVirginia EchoNo ratings yet
- Hepatitis BDocument11 pagesHepatitis BAdrián MartínezNo ratings yet
- Bdb06ff135c7ccb File 2Document29 pagesBdb06ff135c7ccb File 2Mary ThaherNo ratings yet
- Hepatocellular Carcinoma in HIV Positive PatientsDocument14 pagesHepatocellular Carcinoma in HIV Positive PatientsBayarbaatar BoldNo ratings yet
- Khvi 17 1819742Document24 pagesKhvi 17 1819742Sebastian BurgosNo ratings yet
- Prevention of Inection Related Tumor Bgr054Document9 pagesPrevention of Inection Related Tumor Bgr054heruNo ratings yet
- Hepatitis B Virus (HBV) : A Review On Its Prevalence and Infection in Different Areas of IraqDocument8 pagesHepatitis B Virus (HBV) : A Review On Its Prevalence and Infection in Different Areas of IraqKanhiya MahourNo ratings yet
- 05 - Hepatitis B Virus Infection - Lancet 2014Document11 pages05 - Hepatitis B Virus Infection - Lancet 2014Jmv VegaNo ratings yet
- Etiology and Evaluation of Diarrhea in AIDS: A Global Perspective at The MillenniumDocument10 pagesEtiology and Evaluation of Diarrhea in AIDS: A Global Perspective at The MillenniumSri Nowo MinartiNo ratings yet
- WatermarkDocument7 pagesWatermarktrimanovNo ratings yet
- Estimates On HCV Disease Burden Worldwide - Filling The GapsDocument5 pagesEstimates On HCV Disease Burden Worldwide - Filling The GapsRobert G. Gish, MDNo ratings yet
- Wgo 2016Document65 pagesWgo 2016IndahNo ratings yet
- Ijmsv02p0050 PDFDocument8 pagesIjmsv02p0050 PDFfikaanugrahNo ratings yet
- Hepatitis BDocument27 pagesHepatitis BlailashivaNo ratings yet
- Hepatitis b-1Document7 pagesHepatitis b-1api-550162163No ratings yet
- INTRODUCTION Final 5 (2) Sub 3Document25 pagesINTRODUCTION Final 5 (2) Sub 3Dawit g/kidanNo ratings yet
- Infección VIH Primer 2023Document21 pagesInfección VIH Primer 2023MedicazoNo ratings yet
- Hepatitis B Envelope AntigenDocument30 pagesHepatitis B Envelope AntigenBalogun Samuel AbiodunNo ratings yet
- 2015 Hepatitis B PDFDocument35 pages2015 Hepatitis B PDFMarcela MurafaNo ratings yet
- Kenya High Risk GroupsDocument8 pagesKenya High Risk GroupsjackleenNo ratings yet
- Epidemiology, Transmission, and Prevention of Hepatitis B Virus Infection - UpToDateDocument20 pagesEpidemiology, Transmission, and Prevention of Hepatitis B Virus Infection - UpToDatehochanh199xNo ratings yet
- Hepatitis Vaccines: Keywords: Hepatitis A, B, C, D, and E VaccinesDocument18 pagesHepatitis Vaccines: Keywords: Hepatitis A, B, C, D, and E VaccinesPutri Anita AchmadNo ratings yet
- Diagnosis of Viral Hepatitis: ReviewDocument13 pagesDiagnosis of Viral Hepatitis: ReviewReza Redha AnandaNo ratings yet
- Evolving Epidemiology of Hepatitis C Virus: ReviewDocument9 pagesEvolving Epidemiology of Hepatitis C Virus: Reviewtom ibnuNo ratings yet
- The Histories of HIVs: The Emergence of the Multiple Viruses That Caused the AIDS EpidemicsFrom EverandThe Histories of HIVs: The Emergence of the Multiple Viruses That Caused the AIDS EpidemicsNo ratings yet
- Hepatitis CDocument18 pagesHepatitis CGaudeamus IgiturNo ratings yet
- Prevalence and Risk Factors Associated With Chronic Hepatitis B Among Patients Attending Fort Portal Regional Referral Hospital in Kabarole District, Western UgandaDocument13 pagesPrevalence and Risk Factors Associated With Chronic Hepatitis B Among Patients Attending Fort Portal Regional Referral Hospital in Kabarole District, Western UgandaKIU PUBLICATION AND EXTENSIONNo ratings yet
- A Systematic Review of The Epidemiology of Hepatitis A in AfricaDocument15 pagesA Systematic Review of The Epidemiology of Hepatitis A in AfricaNinda PangestikaNo ratings yet
- WHO Position Paper HepBDocument9 pagesWHO Position Paper HepBpradipkshetriNo ratings yet
- Acquired Immunodeficiency Syndrome (HIV Infection, AIDS) : Dr. Rasha SalamaDocument42 pagesAcquired Immunodeficiency Syndrome (HIV Infection, AIDS) : Dr. Rasha SalamamalathiNo ratings yet
- Viral HepatitisDocument53 pagesViral HepatitisAmer JumahNo ratings yet
- Cleveland Clinic Journal of Medicine-2008Document9 pagesCleveland Clinic Journal of Medicine-2008api-208983018No ratings yet
- Hepatite EDocument22 pagesHepatite EYmirNo ratings yet
- 10.1016@S2352 30182030252 6Document10 pages10.1016@S2352 30182030252 6Rizky AmeliaNo ratings yet
- Done 2016 Cha Plan Action Prev Hep enDocument38 pagesDone 2016 Cha Plan Action Prev Hep enNurul MaghfirahNo ratings yet
- NIH Public Access: Epidemiology of HCC: Consider The PopulationDocument10 pagesNIH Public Access: Epidemiology of HCC: Consider The PopulationKe XuNo ratings yet
- Sande's HIV - AIDS Medicine (PDFDrive)Document562 pagesSande's HIV - AIDS Medicine (PDFDrive)angel muñozNo ratings yet
- New - Epidemiological Infectious DiseasesDocument25 pagesNew - Epidemiological Infectious DiseasesSharmaine MararacNo ratings yet
- Prevalence of HBVDocument7 pagesPrevalence of HBVAnas AhmadNo ratings yet
- The Spread, Treatment, and Prevention of HIV-1: Evolution of A Global PandemicDocument12 pagesThe Spread, Treatment, and Prevention of HIV-1: Evolution of A Global PandemicLatiefah NWNo ratings yet
- Khvi 15 10 1649532Document17 pagesKhvi 15 10 1649532bilou hertNo ratings yet
- Referat: Tema: Hepatita Virală B. Abordarea de Către Organizația Mondială A Sănătății (WHO)Document7 pagesReferat: Tema: Hepatita Virală B. Abordarea de Către Organizația Mondială A Sănătății (WHO)Nicanor GîscăNo ratings yet
- Communicable Diseases GIT InfectionDocument63 pagesCommunicable Diseases GIT InfectionReyadh JassemNo ratings yet
- The Prevalence of Hepatitis B Among Secondary School StudentsDocument27 pagesThe Prevalence of Hepatitis B Among Secondary School StudentsOMS PQMNo ratings yet
- Key Facts: Geographical DistributionDocument4 pagesKey Facts: Geographical DistributiondenyNo ratings yet
- Historia de La Hepatitis BDocument15 pagesHistoria de La Hepatitis BJhonatan Efrain Lopez CarbajalNo ratings yet
- Porphyromonas Gingivalis in AlzheimerDocument21 pagesPorphyromonas Gingivalis in AlzheimerJhonatan Efrain Lopez CarbajalNo ratings yet
- Depression Article LancetDocument13 pagesDepression Article LancetDjamil DamryNo ratings yet
- Clopidogrel Withdrawal: Is There A "Rebound" Phenomenon?: Thrombosis and Haemostasis February 2011Document11 pagesClopidogrel Withdrawal: Is There A "Rebound" Phenomenon?: Thrombosis and Haemostasis February 2011Jhonatan Efrain Lopez CarbajalNo ratings yet
- KUIPER Et Al-2007-Alimentary Pharmacology & TherapeuticsDocument11 pagesKUIPER Et Al-2007-Alimentary Pharmacology & TherapeuticsJhonatan Efrain Lopez CarbajalNo ratings yet
- Ascites: Pathogenesis and Terapeutic PrinciplesDocument10 pagesAscites: Pathogenesis and Terapeutic PrinciplesJhonatan Efrain Lopez CarbajalNo ratings yet
- Departamental CardioDocument9 pagesDepartamental CardioIsaac GuerreroNo ratings yet
- Más Allá Del ligando-GRCPDocument17 pagesMás Allá Del ligando-GRCPJhonatan Efrain Lopez CarbajalNo ratings yet
- John 2016Document7 pagesJohn 2016Jhonatan Efraín López CarbajalNo ratings yet
- Acscentsci 0c00272Document17 pagesAcscentsci 0c00272aliy aliyahNo ratings yet
- IJ Ijmm: Pathogenicity of Legionella PneumophilaDocument13 pagesIJ Ijmm: Pathogenicity of Legionella PneumophilaJhonatan Efrain Lopez CarbajalNo ratings yet
- Desai2017 PDFDocument13 pagesDesai2017 PDFJhonatan Efrain Lopez CarbajalNo ratings yet
- Acscentsci 0c00272Document17 pagesAcscentsci 0c00272aliy aliyahNo ratings yet
- Desai2017 PDFDocument13 pagesDesai2017 PDFJhonatan Efrain Lopez CarbajalNo ratings yet
- Desai2017 PDFDocument13 pagesDesai2017 PDFJhonatan Efrain Lopez CarbajalNo ratings yet
- Nuevas Ideas Sobre Un Enigmático Supresor TumoralDocument2 pagesNuevas Ideas Sobre Un Enigmático Supresor TumoralJhonatan Efrain Lopez CarbajalNo ratings yet
- Supresión Del Crecimiento Tumoral Inducible Por HipoxiaDocument6 pagesSupresión Del Crecimiento Tumoral Inducible Por HipoxiaJhonatan Efrain Lopez CarbajalNo ratings yet
- Supresión Del Crecimiento Tumoral Inducible Por HipoxiaDocument6 pagesSupresión Del Crecimiento Tumoral Inducible Por HipoxiaJhonatan Efrain Lopez CarbajalNo ratings yet
- Supresión Del Crecimiento Tumoral Inducible Por HipoxiaDocument6 pagesSupresión Del Crecimiento Tumoral Inducible Por HipoxiaJhonatan Efrain Lopez CarbajalNo ratings yet
- II If en April2015 EquitycompoundersDocument8 pagesII If en April2015 EquitycompoundersbgyggghjkkNo ratings yet
- Youth Worker Course Gold CoastDocument6 pagesYouth Worker Course Gold Coastf5dq3ch5100% (2)
- Package Suppdists': R Topics DocumentedDocument26 pagesPackage Suppdists': R Topics DocumentedHector Alejandro Cabezas CasanuevaNo ratings yet
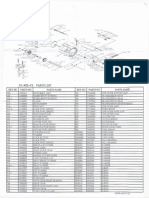
- Okuma CL302L Parts List & ManualDocument3 pagesOkuma CL302L Parts List & Manualcoolestkiwi100% (1)
- Tutorial Set (Queing Model)Document5 pagesTutorial Set (Queing Model)Samuel kwateiNo ratings yet
- Survey Questionnaire 3 - Student EngagementDocument2 pagesSurvey Questionnaire 3 - Student EngagementDAN MARK CAMINGAWANNo ratings yet
- SAP On ASE Development UpdateDocument16 pagesSAP On ASE Development Updatebetoy castroNo ratings yet
- TT21 28112019BNN (E)Document40 pagesTT21 28112019BNN (E)Thanh Tâm TrầnNo ratings yet
- Benjamin Gomez v. Enrico PalomarDocument11 pagesBenjamin Gomez v. Enrico PalomarUlyung DiamanteNo ratings yet
- Nutrition: DR Hiten KalraDocument81 pagesNutrition: DR Hiten KalraAmit SagarNo ratings yet
- Glass, Brittle Plastic and Ceramic Materials Control: BRC Global StandardsDocument8 pagesGlass, Brittle Plastic and Ceramic Materials Control: BRC Global StandardsNavaneethanNo ratings yet
- Cuadernillo de Ingles Grado 4 PrimariaDocument37 pagesCuadernillo de Ingles Grado 4 PrimariaMariaNo ratings yet
- Halftrack Track Chains InstructionsDocument4 pagesHalftrack Track Chains Instructionsddlevy0% (1)
- Well Control - Pore PressureDocument31 pagesWell Control - Pore PressureMiguel Pinto PonceNo ratings yet
- 50 Studies Every Anesthesiologist Shoud Know 2019Document305 pages50 Studies Every Anesthesiologist Shoud Know 2019pcut100% (2)
- Pressure Transducer Davs 311-1-0 Volt - XCMG PartsDocument1 pagePressure Transducer Davs 311-1-0 Volt - XCMG Partsej ejazNo ratings yet
- BCSP GuideDocument44 pagesBCSP GuideCarol Sarmiento DelgadoNo ratings yet
- Jeff Nippard's Workout Routine & Diet (2022) - Jacked GorillaDocument11 pagesJeff Nippard's Workout Routine & Diet (2022) - Jacked Gorillaticoninx100% (1)
- GIS Unit 2 Class TestDocument7 pagesGIS Unit 2 Class TestPrathamesh BhosaleNo ratings yet
- Government and BusinessDocument2 pagesGovernment and BusinessJoshua BrownNo ratings yet
- Study of Causal Factors of Road Accidents On Panipat-Samalkha Section of Nh-1Document7 pagesStudy of Causal Factors of Road Accidents On Panipat-Samalkha Section of Nh-1esatjournalsNo ratings yet
- Date CalcDocument8 pagesDate CalcPaolaNo ratings yet
- CMS-855B - 04052021Document49 pagesCMS-855B - 04052021Sheldon GunbyNo ratings yet
- Nitotile GroutDocument2 pagesNitotile GroutBalasubramanian AnanthNo ratings yet
- 08 LCD Slide Handout 1Document5 pages08 LCD Slide Handout 1Jana Gabrielle Canonigo0% (1)
- Admissions: Application ProceduresDocument13 pagesAdmissions: Application Proceduresisber7abdoNo ratings yet
- CH 7b - Shift InstructionsDocument20 pagesCH 7b - Shift Instructionsapi-237335979100% (1)
- Relationship Marketing & International RetailingDocument17 pagesRelationship Marketing & International Retailingpriyarp5075No ratings yet
- Cross Cultural Management: Hana MaumetDocument32 pagesCross Cultural Management: Hana MaumetGiovanni Francesco PalmaNo ratings yet