You might also like
- QSP 07 Quality Assurance Programme For Intensive Care Units & HduDocument10 pagesQSP 07 Quality Assurance Programme For Intensive Care Units & HduAniruddha ChatterjeeNo ratings yet
- Gap Report Astha HospitalDocument49 pagesGap Report Astha HospitalNidhi VijanNo ratings yet
- Apex Quality Manual-Ashwini Ver 2Document101 pagesApex Quality Manual-Ashwini Ver 2MANORANJANNo ratings yet
- 2 Process Addresses Discharge of All Patients Including Medico-Legal Cases and Patients Leaving Against Medical Advice.Document6 pages2 Process Addresses Discharge of All Patients Including Medico-Legal Cases and Patients Leaving Against Medical Advice.Sanjay Kadam100% (1)
- Patient Safety Organization A Complete Guide - 2020 EditionFrom EverandPatient Safety Organization A Complete Guide - 2020 EditionNo ratings yet
- NABH QI ListDocument9 pagesNABH QI ListMangesh VirkarNo ratings yet
- 1 Procedure(s) Guide Collection, Identification, Handling, Safe Transportation, Processing and Disposal of Specimens.Document10 pages1 Procedure(s) Guide Collection, Identification, Handling, Safe Transportation, Processing and Disposal of Specimens.Sanjay KadamNo ratings yet
- Checklist For Hospital For Data CollectionDocument8 pagesChecklist For Hospital For Data CollectionMuhammad Nadeem NasirNo ratings yet
- Quality Plan Sl. No. Monitoring Record What When How WhoDocument7 pagesQuality Plan Sl. No. Monitoring Record What When How WhosandhyakrishnanNo ratings yet
- All NCs RCADocument40 pagesAll NCs RCAJatoveda HaldarNo ratings yet
- 13 Patient Saefty and Quality ImprovementDocument36 pages13 Patient Saefty and Quality ImprovementShafiq Ur RahmanNo ratings yet
- Quality Introduction: Performance IndicatorDocument28 pagesQuality Introduction: Performance IndicatorLiza VarouqaNo ratings yet
- NABH Course BroucherDocument3 pagesNABH Course Brouchercxz43210% (1)
- New Objective Elements 5th Edition of NABHDocument7 pagesNew Objective Elements 5th Edition of NABHsoni100% (1)
- Crowd Management PolicyDocument3 pagesCrowd Management PolicyAffan sami rayeenNo ratings yet
- NABH AdvantageDocument19 pagesNABH Advantagedr_vikasNo ratings yet
- Obeid Specialized Hospital - Riyadh: Quality Indicator Form 2018 2019Document2 pagesObeid Specialized Hospital - Riyadh: Quality Indicator Form 2018 2019LovelydePerioNo ratings yet
- Medical Case Sheet AuditDocument2 pagesMedical Case Sheet AuditSrinivas PolikepatiNo ratings yet
- Checklist of Anaesthesia Department For NABH Accreditation PreparationDocument3 pagesChecklist of Anaesthesia Department For NABH Accreditation PreparationPayal ThakkerNo ratings yet
- Patient SafetyDocument27 pagesPatient Safetyarahman168No ratings yet
- Document Name Document Number Date Created Date Implemented Name: Designation: Signature: Name: Designation: SignatureDocument49 pagesDocument Name Document Number Date Created Date Implemented Name: Designation: Signature: Name: Designation: Signaturecorona virusNo ratings yet
- MSDSDocument11 pagesMSDSPrabhat Kumar100% (1)
- Improving Healthcare Through Advocacy: A Guide for the Health and Helping ProfessionsFrom EverandImproving Healthcare Through Advocacy: A Guide for the Health and Helping ProfessionsNo ratings yet
- QA For Radiology DepartmentDocument3 pagesQA For Radiology DepartmentRaviraj Pishe100% (1)
- Pest and Vermin Control PolicyDocument4 pagesPest and Vermin Control PolicyCaesar A. Alesna100% (1)
- Clinical Audit Topics SampleDocument3 pagesClinical Audit Topics Samplebalaji srinivasanNo ratings yet
- AuditDocument3 pagesAuditMr. BamsNo ratings yet
- 12 Documented Disciplinary and Grievance Handling Procedure.Document8 pages12 Documented Disciplinary and Grievance Handling Procedure.Sanjay KadamNo ratings yet
- Homoeopathy Indicators NABHDocument105 pagesHomoeopathy Indicators NABHMamoni MaityNo ratings yet
- 15 Define Process To Whom The Patient Record Can Be ReleasedDocument8 pages15 Define Process To Whom The Patient Record Can Be ReleasedSanjay KadamNo ratings yet
- 4+Roadmap+to+NABH+ +finalDocument18 pages4+Roadmap+to+NABH+ +finalSameer BugdeNo ratings yet
- Aac 05 - Laboratory Services Are Provided As Per The Scope of The Hospital'S Services and Laboratory Safety Requirements - 1.0 PurposeDocument6 pagesAac 05 - Laboratory Services Are Provided As Per The Scope of The Hospital'S Services and Laboratory Safety Requirements - 1.0 PurposeBhavna ThakurNo ratings yet
- INDICATORSDocument15 pagesINDICATORSMonish ParmarNo ratings yet
- Guidebook - Entry LevelDocument42 pagesGuidebook - Entry Levelrahul8390No ratings yet
- Kayakalp Standards NABHDocument18 pagesKayakalp Standards NABHSwati BajpaiNo ratings yet
- PfeDocument2 pagesPfeCaryl Lou Casamayor100% (3)
- Availability of Emergency MedicationDocument2 pagesAvailability of Emergency MedicationLovelydePerioNo ratings yet
- 7-Performance MeasurementDocument2 pages7-Performance MeasurementHammad Awan100% (1)
- Healthcare Environmental Services A Complete Guide - 2020 EditionFrom EverandHealthcare Environmental Services A Complete Guide - 2020 EditionNo ratings yet
- Apex Quality ManualDocument141 pagesApex Quality ManualDiksha Gumber100% (2)
- DH Ratnagiri Quality ManualDocument71 pagesDH Ratnagiri Quality ManualPrabhat Kumar100% (2)
- Mortuary Services Checklist - Random 202335531Document4 pagesMortuary Services Checklist - Random 202335531Marion KonesNo ratings yet
- Standard Operating Procedure-SOP: Name of InstitutionDocument4 pagesStandard Operating Procedure-SOP: Name of InstitutionRose jane TambasenNo ratings yet
- Format-Product Recall QSP 8.3.2 F01Document1 pageFormat-Product Recall QSP 8.3.2 F01Ankur Dhir100% (1)
- Annual Appraisal 2019 EDocument2 pagesAnnual Appraisal 2019 EPrince Jhessie L. AbellaNo ratings yet
- Cqi Indicators As Per Nabh 4Th Edition: S. No. Standard Ref. Deptt. KPI Formula FrequencyDocument6 pagesCqi Indicators As Per Nabh 4Th Edition: S. No. Standard Ref. Deptt. KPI Formula FrequencyNatasha BhasinNo ratings yet
- COP 3 & PFR 1.5 - Care of Vulnerable PatientsDocument4 pagesCOP 3 & PFR 1.5 - Care of Vulnerable Patientsn_robinNo ratings yet
- CSSD Performance Quality Analysis at A Super Speciality HospitalDocument29 pagesCSSD Performance Quality Analysis at A Super Speciality HospitalD. GandhirajNo ratings yet
- Deficiencies Observed During Pre-Assessment - Paf 2 Hospital (Full Accreditation) : Date(s) of VisitDocument8 pagesDeficiencies Observed During Pre-Assessment - Paf 2 Hospital (Full Accreditation) : Date(s) of Visitpranit mNo ratings yet
- Gap Analysis Report For Health Care Organnization (Hco) Hospital ProfileDocument7 pagesGap Analysis Report For Health Care Organnization (Hco) Hospital ProfileDhananjay SainiNo ratings yet
- Standard Operating Proceduresgov1Document197 pagesStandard Operating Proceduresgov1Adam ShawNo ratings yet
- Sterilization Audit Checklist SPSmedicalDocument2 pagesSterilization Audit Checklist SPSmedicalHosam MahmoudNo ratings yet
- 2019 Audit ChecklistDocument27 pages2019 Audit ChecklistChhaiyaAgrawalNo ratings yet
- Hospital CommitteesDocument22 pagesHospital CommitteesKarthika MNo ratings yet
- Quality Manual Mental HospitalDocument54 pagesQuality Manual Mental Hospitalsurigao doctors'No ratings yet
- SOP - CQI ProgramDocument20 pagesSOP - CQI Programaaminah tariqNo ratings yet
- Minutes Infection Control Committee Mar 08Document5 pagesMinutes Infection Control Committee Mar 08Czarina Guinto100% (1)
- Medication Error Report FormDocument2 pagesMedication Error Report FormAhmad TaramsyNo ratings yet
- Privileging - Resident Medical OfficerDocument6 pagesPrivileging - Resident Medical OfficerAjaiwant CheemaNo ratings yet
- SOPs For Laboratory-1 PDFDocument178 pagesSOPs For Laboratory-1 PDFNadir A Ibrahim100% (1)
- Adrrf 2Document1 pageAdrrf 2Aniruddha ChatterjeeNo ratings yet
- Nmhaacqsp7 Quality Assurance Programme For ImagingDocument9 pagesNmhaacqsp7 Quality Assurance Programme For ImagingAniruddha ChatterjeeNo ratings yet
- Nmhaacqsp3 Policy & Procedure For Discharge of Patient Including MLC & Absconded CasesDocument10 pagesNmhaacqsp3 Policy & Procedure For Discharge of Patient Including MLC & Absconded CasesAniruddha ChatterjeeNo ratings yet
- Nursing Monitoring NGDocument2 pagesNursing Monitoring NGAniruddha ChatterjeeNo ratings yet
- Nmhaacqsp1 Policy & Procedure For Admission and Registration of Patient & Non-Availability of BedsDocument16 pagesNmhaacqsp1 Policy & Procedure For Admission and Registration of Patient & Non-Availability of BedsAniruddha ChatterjeeNo ratings yet
- Sub: Letter of Appointment For Quality Manager: Mr. Sukhveer Singh Rawat 1, CANAL ROAD, KANDOLI-248001Document2 pagesSub: Letter of Appointment For Quality Manager: Mr. Sukhveer Singh Rawat 1, CANAL ROAD, KANDOLI-248001Aniruddha ChatterjeeNo ratings yet
- R. K. Life Services Pvt. LTD: (Department of Laboratory Medicine)Document7 pagesR. K. Life Services Pvt. LTD: (Department of Laboratory Medicine)Aniruddha ChatterjeeNo ratings yet
- Confidentiality Declaration Of: R. K. Life Services Pvt. LTD (Department of Laboratory Medicine)Document1 pageConfidentiality Declaration Of: R. K. Life Services Pvt. LTD (Department of Laboratory Medicine)Aniruddha ChatterjeeNo ratings yet
- List of Approved Referal LabDocument1 pageList of Approved Referal LabAniruddha ChatterjeeNo ratings yet
- R. K. Life Services Private Limited (Department of Laboratory Medicine)Document1 pageR. K. Life Services Private Limited (Department of Laboratory Medicine)Aniruddha ChatterjeeNo ratings yet
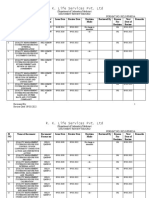
- R. K. Life Services Pvt. LTD: (Department of Laboratory Medicine) Document Review Record Format No: Rkls/Fm/05/ADocument4 pagesR. K. Life Services Pvt. LTD: (Department of Laboratory Medicine) Document Review Record Format No: Rkls/Fm/05/AAniruddha ChatterjeeNo ratings yet
- Document Review RevisionDocument1 pageDocument Review RevisionAniruddha ChatterjeeNo ratings yet
- Sop-Clinical PathologyDocument25 pagesSop-Clinical PathologyAniruddha Chatterjee100% (1)
- Standard Operating Procedure For Clinical Biochemistry: R. K. Life Services Private LimitedDocument7 pagesStandard Operating Procedure For Clinical Biochemistry: R. K. Life Services Private LimitedAniruddha ChatterjeeNo ratings yet
- Sop-Exl 200Document88 pagesSop-Exl 200Aniruddha ChatterjeeNo ratings yet
- HR Manual: Tata Motors HospitalDocument43 pagesHR Manual: Tata Motors HospitalAniruddha ChatterjeeNo ratings yet
- SOP-Advia Centaur XPDocument45 pagesSOP-Advia Centaur XPAniruddha Chatterjee100% (1)
- Policy & Procedure For Retention and Destruction of Medical RecordsDocument7 pagesPolicy & Procedure For Retention and Destruction of Medical RecordsAniruddha ChatterjeeNo ratings yet
- Standard Operating Procedure (Biochemistry - Diasys RESPONS - 910)Document17 pagesStandard Operating Procedure (Biochemistry - Diasys RESPONS - 910)Aniruddha ChatterjeeNo ratings yet
- QSP 05 Surgical ProcedureDocument8 pagesQSP 05 Surgical ProcedureAniruddha ChatterjeeNo ratings yet
- Confidentiality, Integrity and Security of InformationDocument9 pagesConfidentiality, Integrity and Security of InformationAniruddha ChatterjeeNo ratings yet
- QSP 04 Procedure For Referral of PatientDocument6 pagesQSP 04 Procedure For Referral of PatientAniruddha ChatterjeeNo ratings yet
- MR MeetingDocument12 pagesMR MeetingAniruddha ChatterjeeNo ratings yet
- QSP 02 Discharge Procedure Including Medico Legal CasesDocument14 pagesQSP 02 Discharge Procedure Including Medico Legal CasesAniruddha ChatterjeeNo ratings yet
- Preventive Action PlanDocument11 pagesPreventive Action PlanAniruddha Chatterjee100% (1)
- Evidence Based Practice in NursingDocument3 pagesEvidence Based Practice in NursingThrift Advisory100% (2)
- Standards For SHCODocument40 pagesStandards For SHCOEka BNo ratings yet
- Nurs FPX 4010 Assessment 4 Stakeholder PresentationDocument8 pagesNurs FPX 4010 Assessment 4 Stakeholder PresentationEmma WatsonNo ratings yet
- CT Aquilion Start (Mcact0337eaa)Document15 pagesCT Aquilion Start (Mcact0337eaa)JuanGabrielVillamizarNo ratings yet
- Using SBAR To Communicate Falls Risk and Management in Interprofessional Rehabilitation Teams PDFDocument54 pagesUsing SBAR To Communicate Falls Risk and Management in Interprofessional Rehabilitation Teams PDFmehara1920No ratings yet
- Unit 5.5 - JCIDocument38 pagesUnit 5.5 - JCILakshmi Sowjanya AkurathiNo ratings yet
- NURSFPX 4060 Assessment 4Document1 pageNURSFPX 4060 Assessment 4Adam JonesNo ratings yet
- Downloaded From FILIPINO NURSES CENTRAL (WWW - Nursescentral.ning - Com)Document3 pagesDownloaded From FILIPINO NURSES CENTRAL (WWW - Nursescentral.ning - Com)Filipino Nurses CentralNo ratings yet
- BcBsServiceBenefitPlan 2013Document152 pagesBcBsServiceBenefitPlan 2013mpersiNo ratings yet
- The Effect of System Complexity On Patient SafetyDocument12 pagesThe Effect of System Complexity On Patient SafetyDaniel Cooper100% (1)
- Brief Biodata DR Shakti Gupta Latest 210812Document4 pagesBrief Biodata DR Shakti Gupta Latest 210812Amgad Aly FahmyNo ratings yet
- Or-01-005 Surgical Safety ChecklistDocument3 pagesOr-01-005 Surgical Safety ChecklistOHHC ORNo ratings yet
- Kern Ricular MethodDocument30 pagesKern Ricular MethodPrincy FernandoNo ratings yet
- 2020 Competencies Assessment Tool: Ache Healthcare ExecutiveDocument28 pages2020 Competencies Assessment Tool: Ache Healthcare ExecutiveNader ElbokleNo ratings yet
- Ebook Interpersonal Relationships - Professional Communication Skills For Canadian Nurses PDF Full Chapter PDFDocument67 pagesEbook Interpersonal Relationships - Professional Communication Skills For Canadian Nurses PDF Full Chapter PDFconnie.lee826100% (30)
- Risk Matrix For Risk ManagersDocument18 pagesRisk Matrix For Risk ManagersTunas Andiranto100% (2)
- Digital Literac-WPS Office1Document21 pagesDigital Literac-WPS Office1Yamah PrincewillNo ratings yet
- Impact of Health Information Technology Adoption and Its Drivers On Quality of Care & Patient Safety in The Health Care Sector of PakistanDocument18 pagesImpact of Health Information Technology Adoption and Its Drivers On Quality of Care & Patient Safety in The Health Care Sector of PakistanRima RaisyiahNo ratings yet
- National Core StandardsDocument3 pagesNational Core StandardsReginald MaswanganyiNo ratings yet
- Medication Error Concept and Reporting Practices in Saudi Arabia A Multiregional Study Among Healthcare ProfessionalsDocument13 pagesMedication Error Concept and Reporting Practices in Saudi Arabia A Multiregional Study Among Healthcare ProfessionalsAbdulRahman MuthannaNo ratings yet
- Medical ErrorsDocument7 pagesMedical ErrorsDwi SurantoNo ratings yet
- Change Assignment - Nurs 442Document5 pagesChange Assignment - Nurs 442api-558100249No ratings yet
- Kastberg KaitlynDocument33 pagesKastberg Kaitlynapi-641524095No ratings yet
- Bedside Handover SOP PDFDocument20 pagesBedside Handover SOP PDFDewi Ratna Sari100% (1)
- Leadership in NursingDocument14 pagesLeadership in NursingzainuddinNo ratings yet
- Quality Manager CVDocument3 pagesQuality Manager CVQuality SystemNo ratings yet
- HOSP SIBU Policy FebDocument79 pagesHOSP SIBU Policy Febdanial78100% (1)
- S. No Topic Learning Objectives: P.D.A Building, Block # IV, Phase-V, Hayatabad PeshawarDocument2 pagesS. No Topic Learning Objectives: P.D.A Building, Block # IV, Phase-V, Hayatabad PeshawarWaqasNo ratings yet
- Nurs FPX 4900 Assessment 2 Assessing The Problem Quality Safety and Cost ConsiderationsDocument9 pagesNurs FPX 4900 Assessment 2 Assessing The Problem Quality Safety and Cost Considerationslilykevin075No ratings yet
- Sbar:: An Implementation ToolkitDocument48 pagesSbar:: An Implementation ToolkitDiaz FalihaNo ratings yet