You might also like
- Ar-800 Service ManualDocument14 pagesAr-800 Service ManualMarius Corneanu50% (4)
- Samsung H60 Ultrasonido Manual de ServicioDocument230 pagesSamsung H60 Ultrasonido Manual de Servicioresidencia siysNo ratings yet
- Recent Advances in Restorative DentistryDocument48 pagesRecent Advances in Restorative DentistryKranti Prajapati100% (4)
- Trouble Shooting For SK-600IIDocument13 pagesTrouble Shooting For SK-600IIdianNo ratings yet
- Life Fitness 95tiDocument190 pagesLife Fitness 95tiStanko Cane100% (1)
- Pilot Study of A New Freely Available Computer Aided Polyp Detection System in Clinical PracticeDocument6 pagesPilot Study of A New Freely Available Computer Aided Polyp Detection System in Clinical PracticeJoel TroyaNo ratings yet
- RoboticSurgery An Evolution in PracticeDocument3 pagesRoboticSurgery An Evolution in PracticeJoão Lourenço0% (1)
- Future Technologies and Human HealthDocument40 pagesFuture Technologies and Human HealthJohn SalibNo ratings yet
- Computer Vision in The Surgical Operating Room: Review ArticleDocument7 pagesComputer Vision in The Surgical Operating Room: Review Articlelabril.torresmNo ratings yet
- Computer Vision in The Surgical Operating Room: Review ArticleDocument7 pagesComputer Vision in The Surgical Operating Room: Review ArticleSantosh KBNo ratings yet
- Cath Lab PlanningDocument2 pagesCath Lab PlanningHenry SuarezNo ratings yet
- RoboticsDocument7 pagesRoboticsShubham KhandareNo ratings yet
- Robotics in General Surgery: James Wall, MD, Venita Chandra, MD and Thomas Krummel, MDDocument18 pagesRobotics in General Surgery: James Wall, MD, Venita Chandra, MD and Thomas Krummel, MDRizwan AhmedNo ratings yet
- Robotics in Colorectal Surgery: Telemonitoring and TeleroboticsDocument10 pagesRobotics in Colorectal Surgery: Telemonitoring and TeleroboticsprivedNo ratings yet
- Compression of Patient's Video For Transmission Over Low Bandwidth Network PDFDocument12 pagesCompression of Patient's Video For Transmission Over Low Bandwidth Network PDFdev- ledumNo ratings yet
- Neusoft NeuViz 64eDocument13 pagesNeusoft NeuViz 64eahmed_galal_waly1056No ratings yet
- Using A Clinical Protocol For Orthognathic Surgery and Assessing A 3-Dimensional Virtual ApproachDocument15 pagesUsing A Clinical Protocol For Orthognathic Surgery and Assessing A 3-Dimensional Virtual ApproachKorkmaz SayınsuNo ratings yet
- Emergence of Three-Dimensional Video Microsurgery For Male InfertilityDocument2 pagesEmergence of Three-Dimensional Video Microsurgery For Male InfertilityZaliyaNo ratings yet
- Bjs 9711Document15 pagesBjs 9711Bintang MuslimahNo ratings yet
- Liu - Ijos 2017Document11 pagesLiu - Ijos 2017Rohan BhagatNo ratings yet
- DicomWorks Software For Reviewing DICOM Studies AnDocument10 pagesDicomWorks Software For Reviewing DICOM Studies AnAhmed AlkabodyNo ratings yet
- Lgner 2017Document8 pagesLgner 2017paul00040No ratings yet
- The Effect of Video Surveillence (CCTV) On Security Challenges in and OrganizationDocument55 pagesThe Effect of Video Surveillence (CCTV) On Security Challenges in and Organizationfombere isofah tNo ratings yet
- 464 2023 Article 10078Document10 pages464 2023 Article 10078klene0064No ratings yet
- State-Of-The-Art On Cone Beam CT Imaging For Preoperative Planning of Implant PlacementDocument7 pagesState-Of-The-Art On Cone Beam CT Imaging For Preoperative Planning of Implant Placementanimeilove3No ratings yet
- An Easy-To-build, Low-Budget Point-Of-care Ultrasound Simulator From Linux To A Web-Based SolutionDocument6 pagesAn Easy-To-build, Low-Budget Point-Of-care Ultrasound Simulator From Linux To A Web-Based SolutionMostafa AbdelrahmanNo ratings yet
- A Real-Time Polyp-Detection System With Clinical Application in Colonoscopy Using Deep Convolutional Neural NetworksDocument38 pagesA Real-Time Polyp-Detection System With Clinical Application in Colonoscopy Using Deep Convolutional Neural NetworksJoel TroyaNo ratings yet
- Principles of Minimal Invasive SurgeryDocument39 pagesPrinciples of Minimal Invasive SurgeryAvinash KannanNo ratings yet
- Walliczek Dworschak2016Document10 pagesWalliczek Dworschak2016Eham AroraNo ratings yet
- REMOTE SURGERY: TELESURGERY OVER LONG DISTANCESDocument6 pagesREMOTE SURGERY: TELESURGERY OVER LONG DISTANCESramananbmeNo ratings yet
- Robotic SurgeryDocument10 pagesRobotic Surgerys_asmathNo ratings yet
- Ida - DigitalDocument97 pagesIda - DigitalBalaji V RNo ratings yet
- The Handy Urodynamics: PICO SMART Is Based On An AdvancedDocument4 pagesThe Handy Urodynamics: PICO SMART Is Based On An Advancedayham HamamaNo ratings yet
- Digital Cytopathology JCDocument26 pagesDigital Cytopathology JCAchin KumarNo ratings yet
- 1 s2.0 S225549711530077X MainDocument6 pages1 s2.0 S225549711530077X Mainaymohamad2020No ratings yet
- Robotic Assisted LaparosDocument5 pagesRobotic Assisted LaparosInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Robotic-Assisted Surgery For Low Rectal Dissection: From Better Views To Better OutcomeDocument6 pagesRobotic-Assisted Surgery For Low Rectal Dissection: From Better Views To Better OutcomeMarwa MedNo ratings yet
- A Durable Ultrasound Phantom For Trainees Using Common MaterialsDocument7 pagesA Durable Ultrasound Phantom For Trainees Using Common MaterialsYavuz DanisNo ratings yet
- Bariatric Robotic Surgery: A Comprehensive GuideFrom EverandBariatric Robotic Surgery: A Comprehensive GuideCarlos Eduardo DomeneNo ratings yet
- cs-d-aachen-didi_vrDocument4 pagescs-d-aachen-didi_vrMohammad saad aliNo ratings yet
- Digital RadiographyDocument10 pagesDigital Radiographyn fadhliiNo ratings yet
- Medical RobotsDocument26 pagesMedical Robotsajaygill5785No ratings yet
- Medray Letterhead TemplateDocument5 pagesMedray Letterhead TemplateSteve NjugiNo ratings yet
- Reappraisal of Telesurgery in The Era of High-SpeeDocument8 pagesReappraisal of Telesurgery in The Era of High-SpeeAbdulkareem 99No ratings yet
- Planning and Sizing With OsiriXHorosDocument23 pagesPlanning and Sizing With OsiriXHorosJanineNo ratings yet
- Training in Uniportal VATS LobectomyDocument7 pagesTraining in Uniportal VATS LobectomyAlin Ionut BurlacuNo ratings yet
- Surgical RoboticsreviewDocument8 pagesSurgical RoboticsreviewMangesh PachkawadeNo ratings yet
- Latest Trends in Minimally Invasive SurgeryDocument4 pagesLatest Trends in Minimally Invasive SurgeryMc_Lopez_1761No ratings yet
- Principles of Laparoscopic and Robotic SurgeryDocument14 pagesPrinciples of Laparoscopic and Robotic SurgeryMoha 78x.No ratings yet
- A New Digital Denture Procedure: A First Practitioners AppraisalDocument13 pagesA New Digital Denture Procedure: A First Practitioners Appraisalweiguo guanNo ratings yet
- A Clinician's Guide To Digital Radiography SystemsDocument5 pagesA Clinician's Guide To Digital Radiography SystemsRp ATNo ratings yet
- Design and Evaluation of A Low-Cost Smartphone Pulse OximeterDocument13 pagesDesign and Evaluation of A Low-Cost Smartphone Pulse Oximetermahsa sherbafiNo ratings yet
- Integrity of GPS INS IntegrationDocument359 pagesIntegrity of GPS INS IntegrationUmar BhattiNo ratings yet
- CT2S Benemerito2021Document9 pagesCT2S Benemerito2021Ivan BenemeritoNo ratings yet
- Histopathologist and InternetDocument2 pagesHistopathologist and InternetNischita JayarajNo ratings yet
- Anaesthesia in Robotic SurgeryDocument32 pagesAnaesthesia in Robotic SurgeryRaguNo ratings yet
- Somatom Scope: Answers For LifeDocument44 pagesSomatom Scope: Answers For LifeSalvador CordovaNo ratings yet
- Light Vein Viewer PDFDocument9 pagesLight Vein Viewer PDFirfanyNo ratings yet
- Recognition of Root Canal Orifices in Video Sequences As A Future Support System During Endodontic TreatmentDocument4 pagesRecognition of Root Canal Orifices in Video Sequences As A Future Support System During Endodontic TreatmentShubham NaikNo ratings yet
- Anaesthesia For Robotic SurgeryDocument5 pagesAnaesthesia For Robotic Surgerysangamitraachu100% (1)
- Audiology Telemedicine: Education and PracticeDocument7 pagesAudiology Telemedicine: Education and PracticeRoberta VianaNo ratings yet
- Recent Advances in MRI Technology Implications ForDocument7 pagesRecent Advances in MRI Technology Implications ForekajuliantaraNo ratings yet
- Voxel-Based Superimposition of Cone Beam CT Scans For Orthodontic and Craniofacial Follow-Up Overview and Clinical ImplementationDocument21 pagesVoxel-Based Superimposition of Cone Beam CT Scans For Orthodontic and Craniofacial Follow-Up Overview and Clinical ImplementationPhachara SiripraphonrojNo ratings yet
- DMN29 3Document2 pagesDMN29 3dianNo ratings yet
- KR-8100P - KR-8100P - Brown and White OpticiansDocument140 pagesKR-8100P - KR-8100P - Brown and White Opticiansdian0% (1)
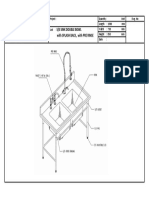
- Sink Double Bowl W Pre Rinse - 1500 X 750 X 850Document1 pageSink Double Bowl W Pre Rinse - 1500 X 750 X 850dianNo ratings yet
- Rodenstock Peristat and Perimat Operation ManualDocument141 pagesRodenstock Peristat and Perimat Operation ManualdianNo ratings yet
- RC-800 Maintenance Manual Doc. ID: OSP-4-86 ID: 01.0-0 RC-800 Check SheetDocument1 pageRC-800 Maintenance Manual Doc. ID: OSP-4-86 ID: 01.0-0 RC-800 Check SheetdianNo ratings yet
- ACME Quote-Word 2003Document4 pagesACME Quote-Word 2003Mutmainnah AGNo ratings yet
- Pedoman Gaji IDocument28 pagesPedoman Gaji IRezi Darma SetiawanNo ratings yet
- For This Product, Please Contact Us From Our WebsiteDocument1 pageFor This Product, Please Contact Us From Our WebsitedianNo ratings yet
- Gsi 39 Auto Tymp: Pure Tone & Tympanometry ScreenerDocument4 pagesGsi 39 Auto Tymp: Pure Tone & Tympanometry ScreenerdianNo ratings yet
- Nagman PHP pneumatic hand pumpsDocument2 pagesNagman PHP pneumatic hand pumpsjaigodaraNo ratings yet
- RC-5000 Maintenance Manual Doc. ID: OSP-4-08 ID: 01.0-0Document1 pageRC-5000 Maintenance Manual Doc. ID: OSP-4-08 ID: 01.0-0dian0% (1)
- Fukuda Denshi FCP-7101 ECG Monitor - Service Manual PDFDocument170 pagesFukuda Denshi FCP-7101 ECG Monitor - Service Manual PDFdianNo ratings yet
- 7 LieDocument2 pages7 LiedianNo ratings yet
- SK-600II Operator's Manual PDFDocument90 pagesSK-600II Operator's Manual PDFdian100% (1)
- Tata Naskah RSUAMDocument1 pageTata Naskah RSUAMdianNo ratings yet
- REP01 ReserveReportContentsDocument10 pagesREP01 ReserveReportContentsdianNo ratings yet
- ManRisk - FRS Tanti 260120150019Document21 pagesManRisk - FRS Tanti 260120150019lalu irwan romadhanNo ratings yet
- Classic III User Manual - English PDFDocument2 pagesClassic III User Manual - English PDFMuhammad BilalNo ratings yet
- Erbe Icc 50 80 SMDocument56 pagesErbe Icc 50 80 SMMiguel De Los Santos PavisicNo ratings yet
- Perbaikan USGDocument1 pagePerbaikan USGdianNo ratings yet
- SurgicalDocument1 pageSurgicaldianNo ratings yet
- Bending Device For Bone PlatesDocument1 pageBending Device For Bone PlatesdianNo ratings yet
- Step by Step Perbaikan Ct-ScanDocument1 pageStep by Step Perbaikan Ct-ScandianNo ratings yet
- 2014-05-23 Dialog+plus enDocument20 pages2014-05-23 Dialog+plus enRandy Mar TagudarNo ratings yet
- May Chay BoDocument142 pagesMay Chay BoHồ Vũ HoàngNo ratings yet
- 20110128112142Document107 pages20110128112142saito36No ratings yet
- Weekly Learning Activity Sheet Arts 10 Quarter 2 Week 6Document7 pagesWeekly Learning Activity Sheet Arts 10 Quarter 2 Week 6Judarlyn MadriaNo ratings yet
- User Guide: Issue 1.1 January 2006Document17 pagesUser Guide: Issue 1.1 January 2006Allegra AmiciNo ratings yet
- Philips Fwd796 Service ManualDocument66 pagesPhilips Fwd796 Service ManualEdilberto AvilaNo ratings yet
- Issue 107 Radio Parts Newsletter - December 2014Document8 pagesIssue 107 Radio Parts Newsletter - December 2014Radio PartsNo ratings yet
- Social Media Image Sizes 2020 A4 PDFDocument19 pagesSocial Media Image Sizes 2020 A4 PDFAndreea MariaNo ratings yet
- The Master and Margarita 2005 TV Series DVDrip Rus With Eng Sub (Download Torrent) - TPBDocument3 pagesThe Master and Margarita 2005 TV Series DVDrip Rus With Eng Sub (Download Torrent) - TPBVictor O. KrausskopfNo ratings yet
- Marantz NR1711 Information Sheet 4k120Document2 pagesMarantz NR1711 Information Sheet 4k120lhaurenceNo ratings yet
- Spirent ChromaticDocument4 pagesSpirent ChromaticulahotiNo ratings yet
- V2460 Manual de InstruçãoDocument44 pagesV2460 Manual de InstruçãoWalefi SilvaNo ratings yet
- Service Manual: Harman/kardonDocument130 pagesService Manual: Harman/kardoncharlyvega100% (3)
- iVMS-4200 Client Software: User ManualDocument331 pagesiVMS-4200 Client Software: User Manualsmk yekaNo ratings yet
- dvdr3570h Service Manual PDFDocument160 pagesdvdr3570h Service Manual PDFMalfoyNo ratings yet
- Lista de CanaisDocument2 pagesLista de CanaisLuiz Humberto100% (1)
- DSS Exam - V2Document11 pagesDSS Exam - V2pr2020016No ratings yet
- LGE Internal T-Con Board Repair GuideDocument5 pagesLGE Internal T-Con Board Repair GuideLeonel Martinez CarrazanaNo ratings yet
- Cisco Video Surveillance Manager Safety and Security Desktop User GuideDocument188 pagesCisco Video Surveillance Manager Safety and Security Desktop User GuideJosue LimaNo ratings yet
- Computer GraphicsDocument50 pagesComputer GraphicsmvdurgadeviNo ratings yet
- Case Study IMCDocument4 pagesCase Study IMCkashif780No ratings yet
- Study and Analysis of Various Video Encryption Algorithms: Ashwitha Vijaya Murari. TDocument5 pagesStudy and Analysis of Various Video Encryption Algorithms: Ashwitha Vijaya Murari. TChatradi HarikaNo ratings yet
- Raspored D3 KanalaDocument30 pagesRaspored D3 Kanalav_nikolic86No ratings yet
- Circuit Explanation of LCD Models for Latin AmericaDocument78 pagesCircuit Explanation of LCD Models for Latin AmericaAntonio ChavezNo ratings yet
- Sony Cp-082s Chassis, Vx-14-21mw1u TV-VCR SMDocument80 pagesSony Cp-082s Chassis, Vx-14-21mw1u TV-VCR SMRoger Martínez BermúdezNo ratings yet
- Ivms-4200 Data SheetDocument4 pagesIvms-4200 Data SheetcloscaNo ratings yet
- MuPS 4000Document2 pagesMuPS 4000gatito1971No ratings yet
- Provix Catalog 2019Document12 pagesProvix Catalog 2019andyandy2590No ratings yet
- Instruction Manual: Connections - Connecting Speakers Playback Setup Troubleshooting Appendix Supplementary InformationDocument131 pagesInstruction Manual: Connections - Connecting Speakers Playback Setup Troubleshooting Appendix Supplementary InformationWeslei BritoNo ratings yet
- Benq GL 940 LCD Monitor User ManualDocument34 pagesBenq GL 940 LCD Monitor User Manualpichi100No ratings yet
- DP Video Others 13112 DriversDocument144 pagesDP Video Others 13112 Driverslimitless freefireNo ratings yet
- Standards For Distributing Video Over IP: Including SMPTE 2022Document8 pagesStandards For Distributing Video Over IP: Including SMPTE 2022DivyaSasiNo ratings yet