You might also like
- Fitness RX For MenDocument84 pagesFitness RX For MenRujichon Iamphattanatam100% (1)
- Eating To Win: Activity, Diet and Weight ControlDocument23 pagesEating To Win: Activity, Diet and Weight ControlAbraham SolomonNo ratings yet
- Treatment of Night Eating SyndromeDocument12 pagesTreatment of Night Eating SyndromejoaomartinelliNo ratings yet
- The Metabolic Type Self Test PDFDocument24 pagesThe Metabolic Type Self Test PDFMonika KramliNo ratings yet
- Long-Term Changes in Energy Expenditure and Body Composition After Massive Weight Loss Induced by Gastric Bypass SurgeryDocument9 pagesLong-Term Changes in Energy Expenditure and Body Composition After Massive Weight Loss Induced by Gastric Bypass SurgeryJavier VegaNo ratings yet
- JI X HDL PESQUISA BIBLIOGRAFICADocument8 pagesJI X HDL PESQUISA BIBLIOGRAFICAJúlia MunizNo ratings yet
- High Energy Lunch Benefits Weight Loss More Than DinnerDocument8 pagesHigh Energy Lunch Benefits Weight Loss More Than DinnerRachmania BudiatiNo ratings yet
- Eating Late Associated With Less Weight LossDocument8 pagesEating Late Associated With Less Weight Lossellla 38No ratings yet
- Jur EngDocument8 pagesJur Engmeiimei meilienhaNo ratings yet
- Verreijen Et Al, 2017 - BIOACTIVE PROTEINDocument8 pagesVerreijen Et Al, 2017 - BIOACTIVE PROTEINAini MahmudahNo ratings yet
- Lundgreen Healthy Weight Loss Maintenance With Exercise 12Document12 pagesLundgreen Healthy Weight Loss Maintenance With Exercise 12Ricardo Parra ArangoNo ratings yet
- VegetariaDocument8 pagesVegetariaBenyi SapepaNo ratings yet
- Ntrs 513-Final PaperDocument8 pagesNtrs 513-Final Paperapi-203339953No ratings yet
- Metabolic Adaptation Is Not A Major Barrier To Weight-Loss MaintenanceDocument8 pagesMetabolic Adaptation Is Not A Major Barrier To Weight-Loss MaintenanceAgustin LopezNo ratings yet
- Effects of Manipulating Eating Frequency During A Behavioral Weight Loss Intervention: A Pilot Randomized Controlled TrialDocument9 pagesEffects of Manipulating Eating Frequency During A Behavioral Weight Loss Intervention: A Pilot Randomized Controlled TrialpedoculoojeteNo ratings yet
- Alternate Day Fasting and Endurance Exercise Combine To Reduce Body Weight and Favorably Alter Plasma Lipids in Obese HumansDocument10 pagesAlternate Day Fasting and Endurance Exercise Combine To Reduce Body Weight and Favorably Alter Plasma Lipids in Obese HumansAndres CaceresNo ratings yet
- Track 3 Eating Patterns and Behaviour P63Document15 pagesTrack 3 Eating Patterns and Behaviour P63Yuriko AndreNo ratings yet
- Nej Mo a 2206038Document12 pagesNej Mo a 2206038dravlamfNo ratings yet
- Differential Gene Expression in Adipose Tissue From Obese Human Subjects During Weight Loss and Weight MaintenanceDocument12 pagesDifferential Gene Expression in Adipose Tissue From Obese Human Subjects During Weight Loss and Weight Maintenancesergiuosan96No ratings yet
- Weight Loss Meta AnalysisDocument6 pagesWeight Loss Meta AnalysisYusuf YNo ratings yet
- Carbohydrate Loading and FemaleDocument18 pagesCarbohydrate Loading and Femaledavid fernandezNo ratings yet
- Weinsier 2000Document7 pagesWeinsier 2000NATHALIA PATRICIA TEOFILO BEZERRA DE MELONo ratings yet
- 2022 JastreboffDocument12 pages2022 JastreboffSinityNo ratings yet
- 1 s2.0 S0026049511003404 MainDocument8 pages1 s2.0 S0026049511003404 MainFrankis De Jesus Vanegas RomeroNo ratings yet
- Ajcn 9530614Document12 pagesAjcn 9530614Mateo TamayoNo ratings yet
- 2022 - JCEM - Metabolic Efficacy of Time-Restricted Eating in AdultsDocument14 pages2022 - JCEM - Metabolic Efficacy of Time-Restricted Eating in AdultsLuiz Fernando Fonseca VieiraNo ratings yet
- Effects of A Meal Replacement On Body CompositionDocument10 pagesEffects of A Meal Replacement On Body CompositionGiffariNo ratings yet
- Weight-Loss Diets For The Prevention and Treatment of ObesityDocument3 pagesWeight-Loss Diets For The Prevention and Treatment of ObesityRupita SitanggangNo ratings yet
- Oby 200353 ADocument8 pagesOby 200353 AGustavo SantosNo ratings yet
- Dietary counselling and food fortification improves outcomes in COPDDocument7 pagesDietary counselling and food fortification improves outcomes in COPDJames Cojab SacalNo ratings yet
- Am J Clin Nutr 2016 Valsesia Ajcn.116.137646Document10 pagesAm J Clin Nutr 2016 Valsesia Ajcn.116.137646kasabeNo ratings yet
- Daily Supplementation With The Lab4P Probiotic Consortium Induces Significant Weight Loss in Overweight AdultsDocument8 pagesDaily Supplementation With The Lab4P Probiotic Consortium Induces Significant Weight Loss in Overweight Adultsj vdkuilNo ratings yet
- Rapid MRI reveals liver fat reduction on low-carb dietDocument4 pagesRapid MRI reveals liver fat reduction on low-carb dietNeil Patrick AngelesNo ratings yet
- Dietary Protein Effect On Body CompositionDocument8 pagesDietary Protein Effect On Body CompositionAllisa RufaedahNo ratings yet
- Effect of Exercise Intensity On Abdominal Fat Loss During Calorie Restriction in Overweight and Obese Postmenopausal WomenDocument10 pagesEffect of Exercise Intensity On Abdominal Fat Loss During Calorie Restriction in Overweight and Obese Postmenopausal WomenΑΡΙΣΤΟΤΕΛΗΣ ΓΕΩΡΓΟΠΟΥΛΟΣNo ratings yet
- Jurnal Tugas 3Document7 pagesJurnal Tugas 3Yuan Zhi YiNo ratings yet
- 6 Carbohydrate Intake and ObesityDocument25 pages6 Carbohydrate Intake and ObesitymariaNo ratings yet
- Clinical NutritionDocument8 pagesClinical Nutritionlorenza osornioNo ratings yet
- 2010larsen PDFDocument12 pages2010larsen PDFLisiane PerinNo ratings yet
- Effects of A High-Protein Ketogenic Diet On Hunger, Appetite, and Weight Loss in Obese Men Feeding Ad Libitum-Am J Clin Nutr-2008-Johnstone-44-55Document12 pagesEffects of A High-Protein Ketogenic Diet On Hunger, Appetite, and Weight Loss in Obese Men Feeding Ad Libitum-Am J Clin Nutr-2008-Johnstone-44-55Ivonne BarrazaNo ratings yet
- Artigo 1Document7 pagesArtigo 1MATHEUS RODRIGUES DO NASCIMENTONo ratings yet
- Long-Term (5-Year) Effects of A Reduced-Fat Diet Intervention in Individuals With Glucose IntoleranceDocument6 pagesLong-Term (5-Year) Effects of A Reduced-Fat Diet Intervention in Individuals With Glucose IntoleranceMiguel Martinez GamboaNo ratings yet
- Biggest Loser 2015 ArticleDocument19 pagesBiggest Loser 2015 ArticleAliNo ratings yet
- How a High-Fat Diet Affects Skeletal Muscle and Insulin Sensitivity in HumansDocument5 pagesHow a High-Fat Diet Affects Skeletal Muscle and Insulin Sensitivity in HumansstarmittNo ratings yet
- Effect of Reducing Total Fat Intake On Body Weight Systematic Review and Meta-Analysis of Randomised Controlled Trials and Cohort StudiesDocument2 pagesEffect of Reducing Total Fat Intake On Body Weight Systematic Review and Meta-Analysis of Randomised Controlled Trials and Cohort Studiesines.queiros.nutricionistaNo ratings yet
- Intermittent Fasting Combined With Calorie Restriction Is Effective For Weight Loss and Cardio-Protection in Obese WomenDocument9 pagesIntermittent Fasting Combined With Calorie Restriction Is Effective For Weight Loss and Cardio-Protection in Obese Womenpriya1832No ratings yet
- Tfeq21 PDFDocument10 pagesTfeq21 PDFDarin MonerNo ratings yet
- Increased Consumption of Dairy Foods and Protein During Diet - and Exercise-Induced Weight Loss Promotes Fat Mass Loss and Lean Mass Gain in Overweight and Obese Premenopausal WomenDocument9 pagesIncreased Consumption of Dairy Foods and Protein During Diet - and Exercise-Induced Weight Loss Promotes Fat Mass Loss and Lean Mass Gain in Overweight and Obese Premenopausal Womenines.queiros.nutricionistaNo ratings yet
- Halawi 2017Document10 pagesHalawi 2017Mirilláiny AnacletoNo ratings yet
- Bdavighi 26 Safaeiyan 5481Document7 pagesBdavighi 26 Safaeiyan 5481Maikon MarquêsNo ratings yet
- Contemporary Clinical Trials: SciencedirectDocument11 pagesContemporary Clinical Trials: SciencedirectYusuf YNo ratings yet
- 1602350a pdf751186925Document6 pages1602350a pdf751186925Nutricionista Nixa RamírezNo ratings yet
- ??? Metabolic SlowingDocument8 pages??? Metabolic SlowingJes BakerNo ratings yet
- Practices Associated With Weight Loss VeDocument8 pagesPractices Associated With Weight Loss VePedro FerreiraNo ratings yet
- Trapp 2008Document8 pagesTrapp 2008GorkaBuesaNo ratings yet
- Weight Regain After RYGBDocument9 pagesWeight Regain After RYGBSorin Niky MocanuNo ratings yet
- Suplementacao em NutricaoDocument9 pagesSuplementacao em NutricaoJoyce CamposNo ratings yet
- Time-Restricted Feeding Plus Resistance Training in Active Females: A Randomized TrialDocument13 pagesTime-Restricted Feeding Plus Resistance Training in Active Females: A Randomized TrialRahman FirmansyahNo ratings yet
- Goh - Excess Fat in The Abdomen - 2018Document6 pagesGoh - Excess Fat in The Abdomen - 2018MIRIAM VIDURRIZAGANo ratings yet
- Similar Weight Loss With Low - or High-Carbohydrate Diets. Golay 1996Document5 pagesSimilar Weight Loss With Low - or High-Carbohydrate Diets. Golay 1996acolpoNo ratings yet
- 2015 AjcnDocument8 pages2015 Ajcnseb2008No ratings yet
- Long-Term Effectiveness of Diet-Plus-Exercise Interventions vs. Diet-Only Interventions For Weight Loss: A Meta-AnalysisDocument11 pagesLong-Term Effectiveness of Diet-Plus-Exercise Interventions vs. Diet-Only Interventions For Weight Loss: A Meta-AnalysisIkhsan JohnsonNo ratings yet
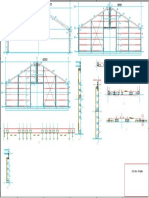
- Gevels en SpantenDocument1 pageGevels en SpantenCristi CapetisNo ratings yet
- Meal Frequency and Timing Are Associated With Changes in Body Mass Index in Adventist Health Study 2Document7 pagesMeal Frequency and Timing Are Associated With Changes in Body Mass Index in Adventist Health Study 2Cristi CapetisNo ratings yet
- Staaloverzicht 2 TWDocument1 pageStaaloverzicht 2 TWCristi CapetisNo ratings yet
- Ankerplan TWDocument1 pageAnkerplan TWCristi CapetisNo ratings yet
- Pes Statement WorksheetDocument2 pagesPes Statement Worksheetapi-638539712No ratings yet
- Anorexia Nervosa: A Literature Review: Progress in Health Sciences December 2020Document7 pagesAnorexia Nervosa: A Literature Review: Progress in Health Sciences December 2020Rayyan TariqNo ratings yet
- Excessive Oral Intake (NI-2.2)Document2 pagesExcessive Oral Intake (NI-2.2)Hasna KhairunnisaGIZINo ratings yet
- The Complete Guide to the HCG DietDocument89 pagesThe Complete Guide to the HCG DietManu0301No ratings yet
- Appetite Stimulants, Digestants and Carminatives: BP602T Pharmacology IIIDocument8 pagesAppetite Stimulants, Digestants and Carminatives: BP602T Pharmacology IIIAkshat sunil JainNo ratings yet
- Second Term 19-20Document24 pagesSecond Term 19-20Krizha Angela NicolasNo ratings yet
- Gelsemium Sempervirens Kent's Repertory PDFDocument41 pagesGelsemium Sempervirens Kent's Repertory PDFRajiv Sharma100% (1)
- Overweight Woman with Irregular Periods and Family History of ObesityDocument48 pagesOverweight Woman with Irregular Periods and Family History of ObesityKimberly Rosialda67% (3)
- Handout 6Document7 pagesHandout 6Nam Trần HoàiNo ratings yet
- Taste Preferences and Diet Palatability in CatsDocument13 pagesTaste Preferences and Diet Palatability in CatsRisky AndreaNo ratings yet
- Feeding the Helpless: Nursing ResponsibilitiesDocument39 pagesFeeding the Helpless: Nursing ResponsibilitiesAlyssa Claire TumulakNo ratings yet
- Journal entry #3: Stress signals checklistDocument2 pagesJournal entry #3: Stress signals checklistABDULJAMIR GAYAKNo ratings yet
- NCP-Resubmission - Mercado, Alyssa Marie R.Document4 pagesNCP-Resubmission - Mercado, Alyssa Marie R.Alyssa MercadoNo ratings yet
- NCP Dengue FeverDocument3 pagesNCP Dengue FeverLorainne BallesterosNo ratings yet
- Regulation of Body WeightDocument120 pagesRegulation of Body WeightCitra YuliasariNo ratings yet
- Nursing Diagnosis & INTERVENTIONDocument10 pagesNursing Diagnosis & INTERVENTIONK Jayakumar KandasamyNo ratings yet
- Tackling ObesityDocument5 pagesTackling ObesityDaimonas JocysNo ratings yet
- FOND 121.aswerdDocument8 pagesFOND 121.aswerdBrian NyakundiNo ratings yet
- Nutritional Guidelines COPDDocument2 pagesNutritional Guidelines COPDRod Rafael De LeonNo ratings yet
- Obeppar Medical SlidesDocument52 pagesObeppar Medical SlidesNimesh ModiNo ratings yet
- DibencozideDocument1 pageDibencozideSeno HyeonNo ratings yet
- Wardlaws Contemporary Nutrition A Functional Approach 5th Edition Wardlaw Test BankDocument38 pagesWardlaws Contemporary Nutrition A Functional Approach 5th Edition Wardlaw Test BankChristinaMcmahondbkfa100% (10)
- Nutrition Requirements and Stress Management in AdulthoodDocument25 pagesNutrition Requirements and Stress Management in AdulthoodCar OrdzNo ratings yet
- Approach To Loss of AppetiteDocument6 pagesApproach To Loss of AppetitePrithvi RameshNo ratings yet
- The Sleep Doctor'S Diet Plan by Michael Breuss, PHD The Sleep Doctor'S Diet PlanDocument5 pagesThe Sleep Doctor'S Diet Plan by Michael Breuss, PHD The Sleep Doctor'S Diet PlanshubhangivsNo ratings yet
- Hypno - Psychotherapy in Treating Obesity 1Document15 pagesHypno - Psychotherapy in Treating Obesity 1samkingjames003No ratings yet