You might also like
- 100 Million Years of Food by Stephen LeDocument9 pages100 Million Years of Food by Stephen Lesimas0% (1)
- MedEntry HPAT Practice Exam Questions With Worked SolutionsDocument82 pagesMedEntry HPAT Practice Exam Questions With Worked SolutionsjewndwdbNo ratings yet
- E4803 DeMarzo Final PgsDocument120 pagesE4803 DeMarzo Final PgsJovana Ognenovska BakalovskaNo ratings yet
- Prospective Study of Major Dietary Patterns and Risk of CoronaryDocument10 pagesProspective Study of Major Dietary Patterns and Risk of CoronaryJohn SammutNo ratings yet
- The Influence of Meal Frequency and Timing On Health in Humans: The Role of FastingDocument19 pagesThe Influence of Meal Frequency and Timing On Health in Humans: The Role of FastingJosé Eduardo Zaragoza LópezNo ratings yet
- Late Eating Is Associated With Cardiometabolic Risk Traits, Obesogenic Behaviors, and Impaired Weight LossDocument8 pagesLate Eating Is Associated With Cardiometabolic Risk Traits, Obesogenic Behaviors, and Impaired Weight LossSukma DewiNo ratings yet
- Case study 1.2. Experimental studyDocument8 pagesCase study 1.2. Experimental studyvulediemkhanhNo ratings yet
- REDALYGDocument8 pagesREDALYGjoel cedeño SánchezNo ratings yet
- Nutritional Epidemiology-Past, Present, Future: EditorialDocument3 pagesNutritional Epidemiology-Past, Present, Future: Editorialisabel sedanoNo ratings yet
- Ultraprocessed Foods and Excess Heart Age Among Us AdultsDocument10 pagesUltraprocessed Foods and Excess Heart Age Among Us AdultsSaionara FranciscoNo ratings yet
- Gosby2013 - Protein Leverage and Energy IntakeDocument9 pagesGosby2013 - Protein Leverage and Energy IntakeDiego TenorioNo ratings yet
- Comparison of Weight-Loss Diets With Different Compositions of Fat, Protein, and CarbohydratesDocument15 pagesComparison of Weight-Loss Diets With Different Compositions of Fat, Protein, and CarbohydratesMichael HubbertNo ratings yet
- Shortreport Open Access: Heather A Hoertel, Matthew J Will and Heather J LeidyDocument8 pagesShortreport Open Access: Heather A Hoertel, Matthew J Will and Heather J LeidyT M Santhosh KumarNo ratings yet
- Artículo de La EpidemiologiaDocument3 pagesArtículo de La EpidemiologiaPaulaNo ratings yet
- Aula 1 - Comparison of Weight-Loss Diets With Different Compositions of Fat, Protein, and CarbohydrateDocument15 pagesAula 1 - Comparison of Weight-Loss Diets With Different Compositions of Fat, Protein, and CarbohydrateRayane SilvaNo ratings yet
- 1 s2.0 S0002916523463034 MainDocument13 pages1 s2.0 S0002916523463034 Maincarlos santamariaNo ratings yet
- Dietary Patterns Exhibit Sex-Specific 3Document9 pagesDietary Patterns Exhibit Sex-Specific 3Luiz Eduardo RodriguezNo ratings yet
- PDF1 A Prospective Study of Healthful and Unhealthful Plant-Based Diet and Risk of Overall and Cause-Specific Mortality.Document13 pagesPDF1 A Prospective Study of Healthful and Unhealthful Plant-Based Diet and Risk of Overall and Cause-Specific Mortality.Jackson0No ratings yet
- Meal Frequency PDFDocument12 pagesMeal Frequency PDFFabi RamosNo ratings yet
- Snack Food, Satiety, and WeightDocument13 pagesSnack Food, Satiety, and WeightEnik guntyastutik100% (1)
- Alimentacion Basada en PlantasDocument9 pagesAlimentacion Basada en PlantasMaria Luz KraanNo ratings yet
- Dietary GeriatricDocument16 pagesDietary GeriatricIndra Setya PermanaNo ratings yet
- On The Importance of Balanced Nutrition: Editorial Comments: July 2019Document4 pagesOn The Importance of Balanced Nutrition: Editorial Comments: July 2019CruxaderNo ratings yet
- Popular Diets: A Scientific Review: Obesity Research March 2001Document41 pagesPopular Diets: A Scientific Review: Obesity Research March 2001Akash.SNo ratings yet
- Temporal Eating Patterns: Associations With Nutrient Intakes, Diet Quality, and Measures of AdiposityDocument10 pagesTemporal Eating Patterns: Associations With Nutrient Intakes, Diet Quality, and Measures of Adipositywilly yashilvaNo ratings yet
- Snack Food, Satiety, and Weight: Advances in Nutrition September 2016Document14 pagesSnack Food, Satiety, and Weight: Advances in Nutrition September 2016fetty hadiastutiNo ratings yet
- Diet Quality of US Adolescents During The Transition To Adulthood: Changes and PredictorsDocument9 pagesDiet Quality of US Adolescents During The Transition To Adulthood: Changes and PredictorsmiraandrianiNo ratings yet
- 2020 - Anguah ET ALDocument12 pages2020 - Anguah ET ALiaiafgdoNo ratings yet
- Article 1 - FFQs Comparative Validation - Subar AF - Am J Epid 2001Document11 pagesArticle 1 - FFQs Comparative Validation - Subar AF - Am J Epid 2001Prajna AdityaraniNo ratings yet
- Am J Clin Nutr 2015 Cespedes Ajcn.Document4 pagesAm J Clin Nutr 2015 Cespedes Ajcn.Jhon Sahatma SinagaNo ratings yet
- Pilichiewicz 2009Document6 pagesPilichiewicz 2009Stella KwanNo ratings yet
- High Energy Lunch Benefits Weight Loss More Than DinnerDocument8 pagesHigh Energy Lunch Benefits Weight Loss More Than DinnerRachmania BudiatiNo ratings yet
- Dietary Fiber Intake and Glycemic Control: Coronary Artery Calcification in Type 1 Diabetes (CACTI) StudyDocument8 pagesDietary Fiber Intake and Glycemic Control: Coronary Artery Calcification in Type 1 Diabetes (CACTI) StudyLeonardo AzevedoNo ratings yet
- Vegetarian Pescatarian and Flexitarian Diets Sociodemographic Determinants and Association With Cardiovascular Risk Factors in A Swiss Urban PopulationDocument9 pagesVegetarian Pescatarian and Flexitarian Diets Sociodemographic Determinants and Association With Cardiovascular Risk Factors in A Swiss Urban PopulationSyahriphona FitrianiNo ratings yet
- Raw Food Diets and Their Effects on Disease and IllnessDocument10 pagesRaw Food Diets and Their Effects on Disease and IllnessKranthi Kumar Chowdary ManamNo ratings yet
- Nutrition Students' Eating HabitsDocument6 pagesNutrition Students' Eating HabitsIka NurhalifahNo ratings yet
- METAANALISISDocument15 pagesMETAANALISISjotame87No ratings yet
- Food Label Use and Awareness of Nutritional Information and Recommendations Among Persons With Chronic DiseaseDocument8 pagesFood Label Use and Awareness of Nutritional Information and Recommendations Among Persons With Chronic DiseaseMohammed OmarNo ratings yet
- Dietary Intakes Associated With Successful Weight Loss and Maintenance During The Weight Loss Maintenance TrialDocument10 pagesDietary Intakes Associated With Successful Weight Loss and Maintenance During The Weight Loss Maintenance TrialParth LalNo ratings yet
- The UK Women's Cohort Study: Comparison of Vegetarians, Fish-Eaters and Meat-EatersDocument8 pagesThe UK Women's Cohort Study: Comparison of Vegetarians, Fish-Eaters and Meat-EatersNina TuilomaNo ratings yet
- Ea 55 Pustaka 13 Protein J. Nutr.-2005-Merchant-1196-201Document6 pagesEa 55 Pustaka 13 Protein J. Nutr.-2005-Merchant-1196-201fathimzahroNo ratings yet
- Evaluation of Nutritional Status of Patients WithDocument9 pagesEvaluation of Nutritional Status of Patients WithTupperware NeenaNo ratings yet
- Fibrele Alimentare in ObezitateDocument6 pagesFibrele Alimentare in ObezitateCatalina CostacheNo ratings yet
- Obesity and Inflammation Associated Insulin Resistance: A ReviewDocument13 pagesObesity and Inflammation Associated Insulin Resistance: A Reviewindex PubNo ratings yet
- 3 - (Ler) Estilos de Vida, Consequencias ObesidadeDocument7 pages3 - (Ler) Estilos de Vida, Consequencias ObesidadeMateus CarvalhoNo ratings yet
- Dietary counselling and food fortification improves outcomes in COPDDocument7 pagesDietary counselling and food fortification improves outcomes in COPDJames Cojab SacalNo ratings yet
- Nutrigenomics and Nutrigenetics in Obesity and CVDsDocument50 pagesNutrigenomics and Nutrigenetics in Obesity and CVDsYair BuenrostroNo ratings yet
- Efectos de La Fibra en ObDocument15 pagesEfectos de La Fibra en ObFabiola Polo ToledoNo ratings yet
- Afifi Et Al, 2017. Dietary Behaviors in Psoriasis Patient-Reported PDFDocument16 pagesAfifi Et Al, 2017. Dietary Behaviors in Psoriasis Patient-Reported PDFPaola StarioloNo ratings yet
- TMP ABB8Document10 pagesTMP ABB8FrontiersNo ratings yet
- SeratDocument8 pagesSeratWilda Putri SariNo ratings yet
- Fast food consumption and BMI status of adolescent girlsDocument5 pagesFast food consumption and BMI status of adolescent girlsm zulNo ratings yet
- Ultra-Processed Foods and Binge EatingDocument13 pagesUltra-Processed Foods and Binge EatingNeil Patrick AngelesNo ratings yet
- Am. J. Epidemiol.-2003-Ma-85-92Document8 pagesAm. J. Epidemiol.-2003-Ma-85-92Eima Siti NurimahNo ratings yet
- Worksheet2 NDTDocument5 pagesWorksheet2 NDTaudsNo ratings yet
- DASH Diet 2020Document7 pagesDASH Diet 2020musyayyadahNo ratings yet
- Assessment of Questionnaire Validity For Measuring Total Fat Intake Using Plasma Lipid Levels As CriteriaDocument6 pagesAssessment of Questionnaire Validity For Measuring Total Fat Intake Using Plasma Lipid Levels As CriteriaRini IrantikaNo ratings yet
- Spirulina ObesidadeDocument10 pagesSpirulina ObesidadeIsabela CastroNo ratings yet
- Dietary Protein and Risk of Ischemic Heart Disease in Middle-Aged Men1-3 Sarah Rosner PDocument8 pagesDietary Protein and Risk of Ischemic Heart Disease in Middle-Aged Men1-3 Sarah Rosner Ppaulobrasil.ortopedistaNo ratings yet
- Changes To The General Nutrition QuestionnaireDocument3 pagesChanges To The General Nutrition QuestionnaireBushra KainaatNo ratings yet
- Jurnal PeanutDocument9 pagesJurnal PeanutLilaaNo ratings yet
- Decades of Diet Deception and the Spread of Non-Communicable Chronic DiseasesFrom EverandDecades of Diet Deception and the Spread of Non-Communicable Chronic DiseasesNo ratings yet
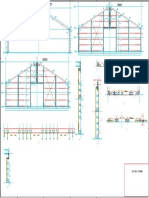
- Gevels en SpantenDocument1 pageGevels en SpantenCristi CapetisNo ratings yet
- SlabireDocument4 pagesSlabireCristi CapetisNo ratings yet
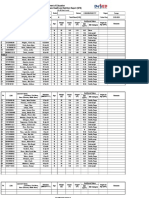
- Staaloverzicht 2 TWDocument1 pageStaaloverzicht 2 TWCristi CapetisNo ratings yet
- Ankerplan TWDocument1 pageAnkerplan TWCristi CapetisNo ratings yet
- Knowledge Acquisition For An Expert System For Diabetic Type-2 DietDocument6 pagesKnowledge Acquisition For An Expert System For Diabetic Type-2 DietFund Inv ItsavNo ratings yet
- Fast Food Addiction ReportDocument12 pagesFast Food Addiction ReportGarry QuezonNo ratings yet
- A Clinical Profile of Metabolic Syndrome and Its Determinants Among Police Officers in BaliDocument5 pagesA Clinical Profile of Metabolic Syndrome and Its Determinants Among Police Officers in BaliDokter FebyanNo ratings yet
- 12 Neoreviews - December2011Document77 pages12 Neoreviews - December2011Mauricio MenaNo ratings yet
- Cardiac Self-Efficacy and Quality of Life in Patients With Coronary Heart Disease: A Cross-Sectional Study From PalestineDocument13 pagesCardiac Self-Efficacy and Quality of Life in Patients With Coronary Heart Disease: A Cross-Sectional Study From Palestineشبلي غرايبهNo ratings yet
- Obesity Prevention and Education For School Nurses Community Health NursingDocument66 pagesObesity Prevention and Education For School Nurses Community Health NursingGabrielaNo ratings yet
- Chair Master-Exercise-Instructor-Manual-with-pictures PDFDocument64 pagesChair Master-Exercise-Instructor-Manual-with-pictures PDFonix2000100% (1)
- 3 Health LM Q1Document32 pages3 Health LM Q1Daisy MendiolaNo ratings yet
- Eating Disorders in Primary CareDocument13 pagesEating Disorders in Primary Caresorin.morosan64No ratings yet
- The Prevalence of Obesity Among Health Staffs in Muar Health District Office in 2018: A Cross Sectional StudyDocument14 pagesThe Prevalence of Obesity Among Health Staffs in Muar Health District Office in 2018: A Cross Sectional StudyPBR NOR HAZWANI BINTI ABDULLAHNo ratings yet
- Healthy Diet: Key FactsDocument6 pagesHealthy Diet: Key FactsYuni NilamsariNo ratings yet
- Consumption Pattern, Attitudes and Nutrition Knowledge On Soft Drinks Among Belgian AdultsDocument12 pagesConsumption Pattern, Attitudes and Nutrition Knowledge On Soft Drinks Among Belgian AdultsdrafthNo ratings yet
- Catanduanes State University Nutrition Exam Provides Diet PrescriptionsDocument4 pagesCatanduanes State University Nutrition Exam Provides Diet PrescriptionsVin Mark GiananNo ratings yet
- Pe 10 Strategies 2ND GRADINGDocument8 pagesPe 10 Strategies 2ND GRADINGMarissa C AustriaNo ratings yet
- 7 Reasons To Eat BreakfastDocument4 pages7 Reasons To Eat BreakfastIvan Kulev100% (1)
- TES Harian: Bahasa InggrisDocument3 pagesTES Harian: Bahasa Inggris07 - Faizah Atiqah Maharani - 092No ratings yet
- A Plant Based Diet For The Treatment and Prevention of Type 2 DiabetesDocument84 pagesA Plant Based Diet For The Treatment and Prevention of Type 2 DiabetesAndreea DumitrescuNo ratings yet
- "More Than A Diet": A Qualitative Investigation of Young Vegan Women's Relationship To FoodDocument34 pages"More Than A Diet": A Qualitative Investigation of Young Vegan Women's Relationship To FoodIHLIHLNo ratings yet
- Best Practice & Research Clinical Rheumatology: Kim L. Bennell, Fiona Dobson, Rana S. HinmanDocument25 pagesBest Practice & Research Clinical Rheumatology: Kim L. Bennell, Fiona Dobson, Rana S. HinmanPablo Fuentes LaraNo ratings yet
- SOP Nirjhar Ruth GhoshDocument2 pagesSOP Nirjhar Ruth GhoshGazi MahfujNo ratings yet
- 1 s2.0 S0883540321005842 MainDocument6 pages1 s2.0 S0883540321005842 MainSavNo ratings yet
- 28 Days Weight Loss Program PDFDocument21 pages28 Days Weight Loss Program PDFkiseNo ratings yet
- Shahad 4Document15 pagesShahad 4Mohammed OmarNo ratings yet
- Child ObesityDocument5 pagesChild ObesitySean ShaNo ratings yet
- School Form 8 GREENDocument3 pagesSchool Form 8 GREENHazel Anne Alcala CompocNo ratings yet
- Don Mariano Marcos Memorial State University Campus Film Reveals Sugar's EffectsDocument3 pagesDon Mariano Marcos Memorial State University Campus Film Reveals Sugar's EffectsJinky FernandezNo ratings yet
- Feeding Disorders - Blok 16Document65 pagesFeeding Disorders - Blok 16Kahfi Rakhmadian KiraNo ratings yet