You might also like
- Exercise IntensityDocument5 pagesExercise Intensitymr_n_manNo ratings yet
- 410 415 PDFDocument6 pages410 415 PDFsportrecifeonusaNo ratings yet
- Kanaley Aerobico SustratosDocument6 pagesKanaley Aerobico SustratosMartinVertolazNo ratings yet
- Análise Crítica de Um Artigo Científico - CópiaDocument10 pagesAnálise Crítica de Um Artigo Científico - CópiaJoao MartinsNo ratings yet
- Sex Differences in The Effects of 12 Weeks Sprint Interval Training On Body Fat Mass - Bagley Et Al 2016Document8 pagesSex Differences in The Effects of 12 Weeks Sprint Interval Training On Body Fat Mass - Bagley Et Al 2016Bumbum AtaunNo ratings yet
- Two Weeks of High-Intensity Aerobic Interval Training Increases The Capacity For Fat Oxidation During Exercise in Women. Journal of ADocument9 pagesTwo Weeks of High-Intensity Aerobic Interval Training Increases The Capacity For Fat Oxidation During Exercise in Women. Journal of AFrancisco EspinozaNo ratings yet
- Weight Loss Improves Walking in Obese WomenDocument7 pagesWeight Loss Improves Walking in Obese WomenfannyNo ratings yet
- Hunter 2008Document7 pagesHunter 2008volmedo28No ratings yet
- Repeated Plyometric Exercise Attenuates Blood Glucose in Healthy AdultsDocument9 pagesRepeated Plyometric Exercise Attenuates Blood Glucose in Healthy AdultsBlake d souzaNo ratings yet
- JSSM 11 495Document7 pagesJSSM 11 495Tahira RajputNo ratings yet
- Fact #1: Wellness & Fitness-Body OptimizationDocument13 pagesFact #1: Wellness & Fitness-Body OptimizationCheeken CharliNo ratings yet
- Functional High Intensity Exercise Training Ameliorates Insulin Resistance and Cardiometabolic Risk Factors in Type 2 DiabetesDocument22 pagesFunctional High Intensity Exercise Training Ameliorates Insulin Resistance and Cardiometabolic Risk Factors in Type 2 DiabetesDavid Ruiz GonzalezNo ratings yet
- Effects of Step Aerobics on Weight Loss & Body CompositionDocument9 pagesEffects of Step Aerobics on Weight Loss & Body CompositionNíí PereiraNo ratings yet
- Acute Interval Exercise Intensity Does Not Affect Appetite and Nutrient Preferences in Overweight and Obese MalesDocument7 pagesAcute Interval Exercise Intensity Does Not Affect Appetite and Nutrient Preferences in Overweight and Obese MalesDavid HaluliNo ratings yet
- Research ArticleDocument9 pagesResearch ArticleLISTIA NURBAETINo ratings yet
- Adaptations To Skeletal Muscle With Endurance Exercise TrainingDocument5 pagesAdaptations To Skeletal Muscle With Endurance Exercise TrainingYo Vivo Fit Pablo y KarlaNo ratings yet
- Kidney Paper - 2017Document9 pagesKidney Paper - 2017samah hossnyNo ratings yet
- Effects of Aerobic and Resistance Training On Hemoglobin A Levels in Patients With Type 2 DiabetesDocument10 pagesEffects of Aerobic and Resistance Training On Hemoglobin A Levels in Patients With Type 2 DiabetesTaufik JeboEdNo ratings yet
- Simple Bodyweight Training Improves Cardiorespiratory Fitness With Minimal Time Commitment: A Contemporary Application of The 5BX ApproachDocument8 pagesSimple Bodyweight Training Improves Cardiorespiratory Fitness With Minimal Time Commitment: A Contemporary Application of The 5BX ApproachROBERTANo ratings yet
- JPES Chenetal 2016 PDFDocument7 pagesJPES Chenetal 2016 PDFRizqiAnnisaPermatasariNo ratings yet
- Low-Volume High-Intensity Interval Training Reduces Hyperglycemia and Increases Muscle Mitochondrial Capacity in Patients With Type 2 DiabetesDocument7 pagesLow-Volume High-Intensity Interval Training Reduces Hyperglycemia and Increases Muscle Mitochondrial Capacity in Patients With Type 2 DiabetesSafira Ridha UlyaNo ratings yet
- Lipid Oxidation and Perceived Exertion Level During Exercise in Obese: Effect of The Exercise FormDocument6 pagesLipid Oxidation and Perceived Exertion Level During Exercise in Obese: Effect of The Exercise FormInternational Organization of Scientific Research (IOSR)No ratings yet
- Análise Crítica de Um Artigo Científico - Cópia - CópiaDocument11 pagesAnálise Crítica de Um Artigo Científico - Cópia - CópiaJoao MartinsNo ratings yet
- Postprandial Light Physical Activity Blunts The Blood Glucose IncreaseDocument3 pagesPostprandial Light Physical Activity Blunts The Blood Glucose IncreaseRemusLupinnNo ratings yet
- Apnm 2014 0357Document8 pagesApnm 2014 0357adri20121989No ratings yet
- Faster onset of glulisine vs lisproDocument8 pagesFaster onset of glulisine vs lisproAbdulrhman FadhilNo ratings yet
- Pre-Exercise Arginine Supplementation Increases Time To Exhaustion in Elite Male WrestlersDocument5 pagesPre-Exercise Arginine Supplementation Increases Time To Exhaustion in Elite Male WrestlersAndrei ChirilaNo ratings yet
- Physiotherapy 3 1 2Document4 pagesPhysiotherapy 3 1 2AjiNo ratings yet
- SlabireDocument4 pagesSlabireCristi CapetisNo ratings yet
- Effects of High-Intensity Intermittent Exercise Training On Appetite RegulationDocument9 pagesEffects of High-Intensity Intermittent Exercise Training On Appetite RegulationIrene Chrysovalanto ThemistocleousNo ratings yet
- Effects of Hyperoxia On Skeletal Muscle Carbohydrate Metabolism During Transient and Steady-State ExerciseDocument7 pagesEffects of Hyperoxia On Skeletal Muscle Carbohydrate Metabolism During Transient and Steady-State ExerciseNdelooDOnkNo ratings yet
- Research PosterDocument1 pageResearch Posterapi-351191501No ratings yet
- Effect of An Acute Period of Resistance Exercise On Excess Post-Exercise Oxygen ConsumptionDocument7 pagesEffect of An Acute Period of Resistance Exercise On Excess Post-Exercise Oxygen ConsumptionaxkielyNo ratings yet
- Exercise Training Induced Visceral Fat Loss in Obese Women The RoleDocument14 pagesExercise Training Induced Visceral Fat Loss in Obese Women The RolepauloNo ratings yet
- Artigo 1Document7 pagesArtigo 1MATHEUS RODRIGUES DO NASCIMENTONo ratings yet
- Comparison of High-Intensity IDocument17 pagesComparison of High-Intensity IIulian-Stefan HOLUBIACNo ratings yet
- The Combined Effects of Physical Exercise Training and Detraining On Adiponectin in Overweight and Obese ChildrenDocument6 pagesThe Combined Effects of Physical Exercise Training and Detraining On Adiponectin in Overweight and Obese ChildrenFatimatus Zahroh IchsanNo ratings yet
- Concurrent Resistance and Endurance Training Influence Basal Metabolic Rate in Nondieting IndividualsDocument6 pagesConcurrent Resistance and Endurance Training Influence Basal Metabolic Rate in Nondieting IndividualsRui CunhaNo ratings yet
- DANTAS 2020 Exercise-Induced Increases in Insulin Sensitivity After Bariatric Surgery Are Mediated by Muscle Extracellular Matrix RemodelingDocument17 pagesDANTAS 2020 Exercise-Induced Increases in Insulin Sensitivity After Bariatric Surgery Are Mediated by Muscle Extracellular Matrix RemodelingCris AquinoNo ratings yet
- Pengaruh Latihan Zumba Terhadap Kadar Kolesterol High Density Lipoprotein DarahDocument5 pagesPengaruh Latihan Zumba Terhadap Kadar Kolesterol High Density Lipoprotein DarahMarshella ChandraNo ratings yet
- Acute effects of microcurrent and exercise on abdominal fatDocument7 pagesAcute effects of microcurrent and exercise on abdominal fatNatalia Franco PérezNo ratings yet
- Physical Activity Reduces Metabolic Syndrome RiskDocument9 pagesPhysical Activity Reduces Metabolic Syndrome RiskEsteban Avila IraguenNo ratings yet
- Dietary Re-Education, Exercise Program, Performance and Body Indexes Associated With Risk Factors in Overweight/Obese WomenDocument9 pagesDietary Re-Education, Exercise Program, Performance and Body Indexes Associated With Risk Factors in Overweight/Obese WomenLuciNo ratings yet
- Acute Effect of Different Orders of Concurrent Training On GlycemiaDocument8 pagesAcute Effect of Different Orders of Concurrent Training On GlycemiaAlexandre VizzoniNo ratings yet
- Journal Club - LRDocument39 pagesJournal Club - LRkaligithi deepshaNo ratings yet
- Bachman 2016 Exercising in The Fasted State Reduced 24-Hour EnergyDocument7 pagesBachman 2016 Exercising in The Fasted State Reduced 24-Hour EnergyvictorsainzvegaNo ratings yet
- Reducing The Intensity and Volume of Interval Training 1min X 1 MinDocument8 pagesReducing The Intensity and Volume of Interval Training 1min X 1 MinEduardo VieyraNo ratings yet
- Exercise Guidelines in Pregnancy: New PerspectivesDocument17 pagesExercise Guidelines in Pregnancy: New PerspectivesHeidy Bravo RamosNo ratings yet
- HIIT - Different Methods ComparisonDocument7 pagesHIIT - Different Methods Comparisonbonifax1No ratings yet
- Jurnal NataDocument9 pagesJurnal Natadr. siti alfiana RS PELNINo ratings yet
- Fatone 2010Document7 pagesFatone 2010Blake d souzaNo ratings yet
- KhamaDocument7 pagesKhamaWaren SharonNo ratings yet
- Experimental Study of Aerobic Exercise On The Weight Loss Effect of Obese Female College StudentsDocument4 pagesExperimental Study of Aerobic Exercise On The Weight Loss Effect of Obese Female College StudentsPaula DueñasNo ratings yet
- Camacho-Cardenosa Et Al., 2019Document25 pagesCamacho-Cardenosa Et Al., 2019Irene Chrysovalanto ThemistocleousNo ratings yet
- The Effect of Postprandial Exercise On MealrelatedDocument7 pagesThe Effect of Postprandial Exercise On MealrelatedLeonardoValenzuelaNo ratings yet
- Strasser 2007Document5 pagesStrasser 2007pablo.s4672No ratings yet
- Epoc 2021 Resistido X HitDocument9 pagesEpoc 2021 Resistido X HitClaudia BarcellarNo ratings yet
- How a High-Fat Diet Affects Skeletal Muscle and Insulin Sensitivity in HumansDocument5 pagesHow a High-Fat Diet Affects Skeletal Muscle and Insulin Sensitivity in HumansstarmittNo ratings yet
- High-Intensity Intermittent Exercise and Fat LossDocument10 pagesHigh-Intensity Intermittent Exercise and Fat Lossalekad65No ratings yet
- Online First Online First: Proprioceptive Training For The Prevention of Ankle Sprains: An Evidence-Based ReviewDocument3 pagesOnline First Online First: Proprioceptive Training For The Prevention of Ankle Sprains: An Evidence-Based ReviewNICOLÁS ANDRÉS AYELEF PARRAGUEZNo ratings yet
- Bradshaw 2008Document7 pagesBradshaw 2008GorkaBuesaNo ratings yet
- Kloskowska 2016Document21 pagesKloskowska 2016GorkaBuesaNo ratings yet
- Kachingwe 2008Document14 pagesKachingwe 2008GorkaBuesaNo ratings yet
- Effects of Creatine Supplementation and Resistance Training On Muscle Strength and Weightlifting PerformanceDocument10 pagesEffects of Creatine Supplementation and Resistance Training On Muscle Strength and Weightlifting Performanceانجمن بدنسازی ایرانNo ratings yet
- Abe 2017 PDFDocument6 pagesAbe 2017 PDFJavier Estelles MuñozNo ratings yet
- Rodr ́ıguez-Rosell 2016Document16 pagesRodr ́ıguez-Rosell 2016GorkaBuesaNo ratings yet
- Balance-And Strength-Training Protocols To Improve Chronic Ankle Instability Deficits, Part I: Assessing Clinical Outcome MeasuresDocument10 pagesBalance-And Strength-Training Protocols To Improve Chronic Ankle Instability Deficits, Part I: Assessing Clinical Outcome MeasuresGorkaBuesaNo ratings yet
- Understanding Athletic Pubalgia: A ReviewDocument5 pagesUnderstanding Athletic Pubalgia: A ReviewMikeNo ratings yet
- Rehabilitation of The Ankle After Acute Sprain or Chronic InstabilityDocument17 pagesRehabilitation of The Ankle After Acute Sprain or Chronic InstabilityAndres Ignacio Lastra MillanNo ratings yet
- Hoff Helgerud SMsoccerreview 04Document16 pagesHoff Helgerud SMsoccerreview 04pepdormanceNo ratings yet
- Diagnosis, Treatment and Prevention of Ankle Sprains: An Evidence-Based Clinical GuidelineDocument7 pagesDiagnosis, Treatment and Prevention of Ankle Sprains: An Evidence-Based Clinical GuidelineBunga PermataNo ratings yet
- Wisløff 2004Document5 pagesWisløff 2004GorkaBuesaNo ratings yet
- R B S, S, J P W - T Y S P: Elationships Etween Trength Print AND UMP Erformance in ELL Rained Outh Occer LayersDocument5 pagesR B S, S, J P W - T Y S P: Elationships Etween Trength Print AND UMP Erformance in ELL Rained Outh Occer LayersGorkaBuesaNo ratings yet
- Wing 2018Document28 pagesWing 2018GorkaBuesaNo ratings yet
- Rodr ́ıguez-Rosell 2016Document16 pagesRodr ́ıguez-Rosell 2016GorkaBuesaNo ratings yet
- The Flywheel Leg-Curl Machine: Offering Eccentric Overload For Hamstring DevelopmentDocument6 pagesThe Flywheel Leg-Curl Machine: Offering Eccentric Overload For Hamstring DevelopmentGorkaBuesaNo ratings yet
- Enhancing Change-of-Direction Speed in Soccer Players by Functional Inertial Eccentric Overload and Vibration TrainingDocument8 pagesEnhancing Change-of-Direction Speed in Soccer Players by Functional Inertial Eccentric Overload and Vibration TrainingGorkaBuesaNo ratings yet
- Rønnestad 2011Document28 pagesRønnestad 2011GorkaBuesaNo ratings yet
- Yong-Hyun 2011Document7 pagesYong-Hyun 2011GorkaBuesaNo ratings yet
- Factors Influencing Physiological Responses to Small-Sided Soccer GamesDocument9 pagesFactors Influencing Physiological Responses to Small-Sided Soccer GamesGorkaBuesaNo ratings yet
- Hackney 2008Document8 pagesHackney 2008GorkaBuesaNo ratings yet
- Titin and Nebulin Content in Human Skeletal Muscle Following Eccentric Resistance ExerciseDocument4 pagesTitin and Nebulin Content in Human Skeletal Muscle Following Eccentric Resistance ExerciseGorkaBuesaNo ratings yet
- Goodall, 2016Document15 pagesGoodall, 2016GorkaBuesaNo ratings yet
- Douglas (2016) Eccentric Exercise Physiological CharacteristicsDocument14 pagesDouglas (2016) Eccentric Exercise Physiological CharacteristicsNicolás BastarricaNo ratings yet
- M D A R F I M D: Ovement Emands in Ustralian Ules Ootball As Ndicators of Uscle AmageDocument5 pagesM D A R F I M D: Ovement Emands in Ustralian Ules Ootball As Ndicators of Uscle AmageGorkaBuesaNo ratings yet
- Interleukin-6 Expression After Repeated Bouts of Eccentric ExerciseDocument7 pagesInterleukin-6 Expression After Repeated Bouts of Eccentric ExerciseGorkaBuesaNo ratings yet
- Chronic Adaptations To Eccentric Training A Systematic Review PDFDocument25 pagesChronic Adaptations To Eccentric Training A Systematic Review PDFThiago LealNo ratings yet
- Satellite Cell Numbers in Young and Older Men 24 Hours After Eccentric ExerciseDocument12 pagesSatellite Cell Numbers in Young and Older Men 24 Hours After Eccentric ExerciseGorkaBuesaNo ratings yet
- Effects of 10-Week Eccentric Overload Training On Kinetic Parameters During Change of Direction in Football PlayersDocument9 pagesEffects of 10-Week Eccentric Overload Training On Kinetic Parameters During Change of Direction in Football PlayersGorkaBuesaNo ratings yet
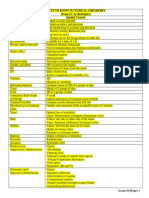
- MUST To KNOW in Clinical ChemistryDocument53 pagesMUST To KNOW in Clinical ChemistryTristan Jay CalabiaNo ratings yet
- Stevia A Promising Herbal SweetenersDocument2 pagesStevia A Promising Herbal SweetenersGustavo RuizNo ratings yet
- What Is A Diet Window?: A Diet Based On A Nobel Prize Winning Idea Can Help You Lose Weight and Slow Down AgingDocument4 pagesWhat Is A Diet Window?: A Diet Based On A Nobel Prize Winning Idea Can Help You Lose Weight and Slow Down Agingcatalin_croitoruNo ratings yet
- Moderate-Intensity Oxygen Uptake Kinetics: Is A Mono-Exponential Function Always Appropriate To Model The Response?Document13 pagesModerate-Intensity Oxygen Uptake Kinetics: Is A Mono-Exponential Function Always Appropriate To Model The Response?Paulo PiresNo ratings yet
- Task 2: Prepare 2 Questions of Each Level of Barrett's TaxonomyDocument6 pagesTask 2: Prepare 2 Questions of Each Level of Barrett's TaxonomyPavithra RangasamyNo ratings yet
- Harvard Guide HealthyDocument12 pagesHarvard Guide Healthyapkarthick100% (3)
- The Analytics Edge SlidesDocument651 pagesThe Analytics Edge Slides陳俊佑100% (1)
- The Importance of MilkDocument19 pagesThe Importance of MilkEsteban GaravitoNo ratings yet
- Risk Factors of Stroke PDFDocument2 pagesRisk Factors of Stroke PDFZulfiqarMuchsinNo ratings yet
- Anatomy of the Posterior MediastinumDocument6 pagesAnatomy of the Posterior MediastinumYheng GaosaiiNo ratings yet
- Assignment 03: Computer Programming and Application (ME-214)Document9 pagesAssignment 03: Computer Programming and Application (ME-214)Asad MirzaNo ratings yet
- Government Intervention Will Not Solve Our Obesity ProblemDocument4 pagesGovernment Intervention Will Not Solve Our Obesity ProblemJulian BeardNo ratings yet
- Abstrac Bahasa InggrisDocument1 pageAbstrac Bahasa Inggrispkm sobangNo ratings yet
- Navy EOD Physical Prep GuideDocument6 pagesNavy EOD Physical Prep Guidequarkshooter849No ratings yet
- NutritionCalc Plus ReportDocument13 pagesNutritionCalc Plus Reportpcrutsin100% (1)
- Level One Rookie Workout GuideDocument32 pagesLevel One Rookie Workout Guidedanesco100% (2)
- Ece 2010 AbstractsDocument316 pagesEce 2010 AbstractsClaudia IrimieNo ratings yet
- FAQ Updated Must Read For Apple Therapy-9Document23 pagesFAQ Updated Must Read For Apple Therapy-9dpparkheNo ratings yet
- Bill Starr Mad Cow 5x5 Logbook CalculatorDocument7 pagesBill Starr Mad Cow 5x5 Logbook CalculatorTerrare93No ratings yet
- Cardiovascular Risk Factors of Hypertension, Smoking and Obesity: Emerging Concerns Among Pathan and Persian Young Adults?Document5 pagesCardiovascular Risk Factors of Hypertension, Smoking and Obesity: Emerging Concerns Among Pathan and Persian Young Adults?-No ratings yet
- MRCP 1 TestDocument261 pagesMRCP 1 TestMohamed Amr Salama100% (2)
- Department of Education School Form 8 Learner's Basic Health and Nutrition Report (SF8)Document4 pagesDepartment of Education School Form 8 Learner's Basic Health and Nutrition Report (SF8)Roxan DosdosNo ratings yet
- ADOLESCENT Obesity MXDocument55 pagesADOLESCENT Obesity MXNor HidayahNo ratings yet
- Patient Education Gout The Basics - UptodateDocument3 pagesPatient Education Gout The Basics - Uptodateapi-347602513No ratings yet
- Obesity Powerpoint G-5Document14 pagesObesity Powerpoint G-5cheryl tubliganNo ratings yet
- Gestational Diabetes AssignmentDocument10 pagesGestational Diabetes Assignmentapi-711118154No ratings yet
- Capstone PosterDocument1 pageCapstone Posterapi-273438577No ratings yet
- CYL456: Chemistry of Life - An Introduction Biomolecules: LipidsDocument45 pagesCYL456: Chemistry of Life - An Introduction Biomolecules: LipidsMegraj MeenaNo ratings yet
- Why Mortality Rate Drops When Doctors Go On StrikeDocument122 pagesWhy Mortality Rate Drops When Doctors Go On StrikeShrija DevendranNo ratings yet
- Army Fitness ManualDocument118 pagesArmy Fitness ManualPaula50% (2)