You might also like
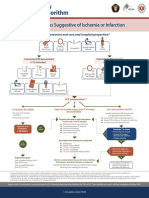
- Syndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionDocument1 pageSyndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionAnonymous CKAborxxwNo ratings yet
- ACLS Advanced Cardiovascular Life Support Provider Manual 2023From EverandACLS Advanced Cardiovascular Life Support Provider Manual 2023No ratings yet
- Acut Coronary SyndromesDocument1 pageAcut Coronary SyndromesMuhittin Selçuk ÖzkanNo ratings yet
- Algo Acs PDFDocument1 pageAlgo Acs PDFJim Christian EllaserNo ratings yet
- Algo Acs PDFDocument1 pageAlgo Acs PDFNety Pandung SalembanNo ratings yet
- Syndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PreparationDocument1 pageSyndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PreparationIGOR SHEYNINNo ratings yet
- Syndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PreparationDocument1 pageSyndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital Preparationgusti angri angalanNo ratings yet
- Posters For ClinicDocument80 pagesPosters For ClinicdenzkissaieNo ratings yet
- Acute Coronary Syndromes Algorithm: Patient Has Signs Suggestive of Ischemia or InfarctionDocument1 pageAcute Coronary Syndromes Algorithm: Patient Has Signs Suggestive of Ischemia or Infarctionjohndoe1995No ratings yet
- Acs PDFDocument1 pageAcs PDFPowool LalaNo ratings yet
- Reanimacion CardiopulmonarDocument15 pagesReanimacion CardiopulmonarVictoriano ValienteNo ratings yet
- Algorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSDocument6 pagesAlgorithm 1: Initial Evaluation and Management: Symptoms of Possible ACSNenyNo ratings yet
- Emergency Department STEMI Algorithm GuideDocument1 pageEmergency Department STEMI Algorithm GuideOgizWaraNo ratings yet
- Tachycardia AlgorithmDocument1 pageTachycardia AlgorithmGideon BahuleNo ratings yet
- Tachycardia With A Pulse Algorithm: Assess Appropriateness For Clinical ConditionDocument1 pageTachycardia With A Pulse Algorithm: Assess Appropriateness For Clinical ConditionDendy Frannuzul RamadhanNo ratings yet
- AlgorithmACLStachycardiawithapulse PDFDocument1 pageAlgorithmACLStachycardiawithapulse PDFDendy Frannuzul RamadhanNo ratings yet
- Stemi NSTEMI or Unstable Angina: Offer AspirinDocument1 pageStemi NSTEMI or Unstable Angina: Offer AspirinVemuri SrinivasNo ratings yet
- Pediatric Bradycardia With A Pulse and Poor Perfusion AlgorithmDocument1 pagePediatric Bradycardia With A Pulse and Poor Perfusion AlgorithmRadhiatul MardhiahNo ratings yet
- ACLS Simplify AlgorithmDocument6 pagesACLS Simplify AlgorithmKristine Monforte Coma UritaNo ratings yet
- ACLS ReportDocument58 pagesACLS ReportCamille Honeyleith FernandoNo ratings yet
- EMS Chest Pain ACS GuidelinesDocument1 pageEMS Chest Pain ACS GuidelinesJuanaly BadiolaNo ratings yet
- Adult Tachycardia (With Pulse) AlgorithmDocument1 pageAdult Tachycardia (With Pulse) AlgorithmJames ChoiNo ratings yet
- Algoritma Ambulance - PHCDocument11 pagesAlgoritma Ambulance - PHCYassarNo ratings yet
- UNC ED Code Stroke Pathway 9 2016 FINALDocument2 pagesUNC ED Code Stroke Pathway 9 2016 FINALJackNo ratings yet
- Assess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaDocument1 pageAssess Appropriateness For Clinical Condition. Heart Rate Typically 150/min If TachyarrhythmiaSiti Nur R Firda FauziyahNo ratings yet
- Peri-Arrest ArrythmiaDocument14 pagesPeri-Arrest Arrythmiamohamed mowafeyNo ratings yet
- Algorithm of Resuscitation CareDocument1 pageAlgorithm of Resuscitation CarejyothiNo ratings yet
- AiepiDocument12 pagesAiepiRenzo Iván Marín DávalosNo ratings yet
- ACLS 2015 Algorithm and Anesthesia ACLS PDFDocument14 pagesACLS 2015 Algorithm and Anesthesia ACLS PDFTaufiqurrahman RizkiNo ratings yet
- Algo ArrestDocument2 pagesAlgo ArrestLocomotorica FK UkiNo ratings yet
- ACS Algorithm 2016 PDFDocument1 pageACS Algorithm 2016 PDFrabin1994No ratings yet
- AlgorithmACLS Tachycardia 200612Document1 pageAlgorithmACLS Tachycardia 200612YassarNo ratings yet
- Acute Coronary SyndromeDocument7 pagesAcute Coronary SyndromePuskesmas Pinang JayaNo ratings yet
- Acute Coronary SyndromeDocument5 pagesAcute Coronary Syndromecotten joeNo ratings yet
- ACLS ACS Algorithm NewDocument3 pagesACLS ACS Algorithm Newsambo100% (1)
- Cardiac Arrest Circular AlgorithmDocument2 pagesCardiac Arrest Circular AlgorithmJunius SimarmataNo ratings yet
- Ecg ReadingsDocument11 pagesEcg ReadingsAnton Laurenciana100% (5)
- AdultTachycardiaWithPulse AlgorithmDocument1 pageAdultTachycardiaWithPulse AlgorithmIsmail SlimNo ratings yet
- Acute Coronary Syndromes - HandoutDocument4 pagesAcute Coronary Syndromes - Handoutapi-641524095No ratings yet
- Advanced Life Support Algorithm: Learning OutcomesDocument8 pagesAdvanced Life Support Algorithm: Learning OutcomesParvathy R NairNo ratings yet
- Inpatientpathway PDFDocument2 pagesInpatientpathway PDFLuis Fernando SaraviaNo ratings yet
- Start CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorDocument2 pagesStart CPR Shout For Help/Activate Emergency Response: Give Oxygen Attach Monitor/DefibrillatorFelicia ErikaNo ratings yet
- G2015 Adult Tachycardia PDFDocument1 pageG2015 Adult Tachycardia PDFibbs91No ratings yet
- G2015 Adult Tachycardia PDFDocument1 pageG2015 Adult Tachycardia PDFPlabber JuneNo ratings yet
- Acs With New Stemi GuidelineDocument35 pagesAcs With New Stemi Guidelinematmin07No ratings yet
- Algorithm-ACLS ACS 200806 1Document1 pageAlgorithm-ACLS ACS 200806 1Kavya Shree100% (1)
- Algo Tachycardia PDFDocument1 pageAlgo Tachycardia PDFYudhistira AdiNo ratings yet
- Chest Pain System - DisorderDocument1 pageChest Pain System - DisorderAA DDNo ratings yet
- Onlinemeded Notes CardioDocument1 pageOnlinemeded Notes CardioCourtney HolbrookNo ratings yet
- Nursing CS Treatment-Of-Atrial-Dysrhythmias 02Document1 pageNursing CS Treatment-Of-Atrial-Dysrhythmias 02frankshro156No ratings yet
- Cardiac Arrest Circular AlgorhythmDocument4 pagesCardiac Arrest Circular AlgorhythmAisyah Nur KarimahNo ratings yet
- Diagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineDocument62 pagesDiagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineIrsyah Dwi RNo ratings yet
- Diagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineDocument71 pagesDiagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineRosyid PrasetyoNo ratings yet
- AngiographyDocument15 pagesAngiographyCrystal AdnalacNo ratings yet
- Jyane ReubenDocument35 pagesJyane ReubenAmr El-RefaeyNo ratings yet
- Nursing Lesson Plan on Pre-EclampsiaDocument13 pagesNursing Lesson Plan on Pre-EclampsiaSheena SharmaNo ratings yet
- Cardiovascular - Anatomy & PhysiologyDocument23 pagesCardiovascular - Anatomy & PhysiologySanthoshi Sadhanaa Sankar100% (1)
- Pedia Notes Print2Document5 pagesPedia Notes Print2John Christopher LucesNo ratings yet
- 2002 Sung-Gyu Lee - Adult-To-Adult LDLT at ASAN Medical CenterDocument8 pages2002 Sung-Gyu Lee - Adult-To-Adult LDLT at ASAN Medical CenterPhu PhamHongNo ratings yet
- GAS EXCHANGE AND THE RESPIRATORY SYSTEMDocument7 pagesGAS EXCHANGE AND THE RESPIRATORY SYSTEMChenul WickramasingheNo ratings yet
- The PancreasDocument31 pagesThe PancreasAryan DesaiNo ratings yet
- The Effect of Cilostazol On Right Heart FunctionDocument43 pagesThe Effect of Cilostazol On Right Heart FunctionGunawan YogaNo ratings yet
- Grand Rounds PresentationDocument40 pagesGrand Rounds Presentationapi-610941700No ratings yet
- Animaltissues 180604115637Document40 pagesAnimaltissues 180604115637proud.student2023No ratings yet
- Certified Ecg Tchnician Syllabus 2021Document5 pagesCertified Ecg Tchnician Syllabus 2021Whiteboard DiscoveryNo ratings yet
- NUR 146 MCN2 RLE P2 ExamDocument22 pagesNUR 146 MCN2 RLE P2 ExamMarga WreatheNo ratings yet
- Management of Splenic Injury in The Adult Trauma PatientDocument17 pagesManagement of Splenic Injury in The Adult Trauma PatientArnaldo Santizo SáenzNo ratings yet
- Hypertensive Heart DiseaseDocument13 pagesHypertensive Heart Diseasemariephynn100% (1)
- Lymphatic SystemDocument3 pagesLymphatic Systempierre TritzNo ratings yet
- Copd Case StudyDocument6 pagesCopd Case StudyChrischia Yvonne GualbertoNo ratings yet
- Serial Comparison Algorithm ReferenceDocument28 pagesSerial Comparison Algorithm ReferenceHoàng Anh NguyễnNo ratings yet
- The Cardiovascular System: Gerard Mark C. SantosDocument31 pagesThe Cardiovascular System: Gerard Mark C. SantosRamon T. De Vera100% (1)
- CONCEPT - QuestionsDocument2 pagesCONCEPT - Questionsgreen_archerNo ratings yet
- Contoh Soal FetomaternalDocument10 pagesContoh Soal FetomaternalBella AgustinNo ratings yet
- Unstable Angina PectorisDocument34 pagesUnstable Angina PectoriserinmowokaNo ratings yet
- Circulatory System PPT 1Document47 pagesCirculatory System PPT 1Czarae VillanuevaNo ratings yet
- Magdy El-Masry Prof. of Cardiology Tanta UniversityDocument55 pagesMagdy El-Masry Prof. of Cardiology Tanta UniversityPrabJot SinGhNo ratings yet
- Cardiotonics & Inotropic Drugs PDFDocument10 pagesCardiotonics & Inotropic Drugs PDFZehra AmirNo ratings yet
- Underwriting Cheat Sheet For WMDocument106 pagesUnderwriting Cheat Sheet For WMAleah DatukonNo ratings yet
- SIRSDocument8 pagesSIRSʕ•ᴥ•ʔNo ratings yet
- Obs JauDocument22 pagesObs JauRavi GuptaNo ratings yet
- Hemolytic Anemia IntrinsicDocument14 pagesHemolytic Anemia IntrinsicSophia Gail ChingNo ratings yet
- Centrimag Pre-Connected PackDocument17 pagesCentrimag Pre-Connected PackShuhengNo ratings yet