You might also like
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
- Acute Chest Pain STEMI PathwayDocument1 pageAcute Chest Pain STEMI PathwayAnonymous M0GIIEzFENo ratings yet
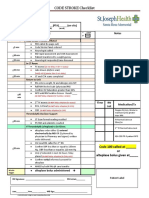
- CODE STROKE Checklist:: NotesDocument1 pageCODE STROKE Checklist:: NotesAdam MochtarNo ratings yet
- Algo Acs PDFDocument1 pageAlgo Acs PDFJim Christian EllaserNo ratings yet
- Algo Acs PDFDocument1 pageAlgo Acs PDFNety Pandung SalembanNo ratings yet
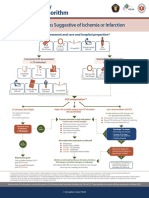
- Syndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionDocument8 pagesSyndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionNugroho TeguhNo ratings yet
- Syndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionDocument1 pageSyndroms Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PrepartionAnonymous CKAborxxwNo ratings yet
- Acut Coronary SyndromesDocument1 pageAcut Coronary SyndromesMuhittin Selçuk ÖzkanNo ratings yet
- Expanding The Therapeutic Window For Acute Ischemic Stroke:: New Agents, New ApproachesDocument29 pagesExpanding The Therapeutic Window For Acute Ischemic Stroke:: New Agents, New ApproachesDr. RajibNo ratings yet
- Truspected Stroke AlgorithmDocument4 pagesTruspected Stroke Algorithmtri wahyunoNo ratings yet
- Rehab CIWDocument10 pagesRehab CIWMark Allan Linco RezagaNo ratings yet
- Acs PDFDocument1 pageAcs PDFPowool LalaNo ratings yet
- Emergency Renal Referral PathwayDocument3 pagesEmergency Renal Referral PathwayYadi SupriyadiNo ratings yet
- Dat e Physicians Order RationaleDocument4 pagesDat e Physicians Order Rationaleember parkNo ratings yet
- Suspected Stroke Algorithm: NINDS Time GoalsDocument1 pageSuspected Stroke Algorithm: NINDS Time Goalsjohndoe1995No ratings yet
- Estatus EpilépticoDocument16 pagesEstatus EpilépticoLizbeth PalomecNo ratings yet
- PROBLEM ORIENTED MEDICAL RECORD FOR ACUTE KIDNEY INJURY MANAGEMENTDocument1 pagePROBLEM ORIENTED MEDICAL RECORD FOR ACUTE KIDNEY INJURY MANAGEMENTFirdha RositaNo ratings yet
- Diagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineDocument71 pagesDiagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineRosyid PrasetyoNo ratings yet
- Diagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineDocument62 pagesDiagnosis and Initial Treatment of Ischemic Stroke: Health Care GuidelineIrsyah Dwi RNo ratings yet
- ICSI Stroke June2019 v2Document55 pagesICSI Stroke June2019 v2PerwiraNo ratings yet
- Stroke Guidelines: Cva Critical Pathway Department of NeurologyDocument5 pagesStroke Guidelines: Cva Critical Pathway Department of NeurologyplethoraldorkNo ratings yet
- Syndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PreparationDocument1 pageSyndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PreparationIGOR SHEYNINNo ratings yet
- COVID-19 TREATMENT ADULT Algorithm 4.3.20Document10 pagesCOVID-19 TREATMENT ADULT Algorithm 4.3.20luizfelipenobresc5492100% (1)
- Management of Acute Coronary Syndrome / NSTEMI: Purpose of The GuidelineDocument7 pagesManagement of Acute Coronary Syndrome / NSTEMI: Purpose of The GuidelineSahera Nurhidayah NasutionNo ratings yet
- 2021 ACLS Study GuideDocument20 pages2021 ACLS Study GuideShane Brown83% (12)
- Ynhhs - Covid-19 Treatment Adult Algorithm 4.3.20Document10 pagesYnhhs - Covid-19 Treatment Adult Algorithm 4.3.20Ren SNo ratings yet
- Neurology Eccles AVT Cheat SheetDocument2 pagesNeurology Eccles AVT Cheat SheetAlbatros LunaNo ratings yet
- Greyzones 2023 V7.1Document12 pagesGreyzones 2023 V7.1Abdel-hafiz MamounNo ratings yet
- Troponin PathwayDocument1 pageTroponin PathwayAllana AngelesNo ratings yet
- Reanimacion CardiopulmonarDocument15 pagesReanimacion CardiopulmonarVictoriano ValienteNo ratings yet
- Acute Medicine: Shock: Inadequate Tissue and Organ PerfusionDocument3 pagesAcute Medicine: Shock: Inadequate Tissue and Organ Perfusionmyat252No ratings yet
- Code Stroke AlgorithmDocument1 pageCode Stroke AlgorithmZharifah Fauziyyah NafisahNo ratings yet
- Acute Coronary Syndromes Algorithm: Patient Has Signs Suggestive of Ischemia or InfarctionDocument1 pageAcute Coronary Syndromes Algorithm: Patient Has Signs Suggestive of Ischemia or Infarctionjohndoe1995No ratings yet
- YNHHS Adult Treatment Algorithm 05132020 - 382832 - 5 - v5Document20 pagesYNHHS Adult Treatment Algorithm 05132020 - 382832 - 5 - v5nuelitopNo ratings yet
- NCP - PreeclampsiaDocument3 pagesNCP - PreeclampsiaRap De la Cruz50% (2)
- Cardiac Arrest Circular AlgorhythmDocument4 pagesCardiac Arrest Circular AlgorhythmAisyah Nur KarimahNo ratings yet
- Anesthesia Pocket Guide 2020 PDFDocument2 pagesAnesthesia Pocket Guide 2020 PDFMaksym DemianchukNo ratings yet
- Clinical Pathway Peds Appendicitis 2012Document3 pagesClinical Pathway Peds Appendicitis 2012DivaraNo ratings yet
- Tto COVID-19 TREATMENT ADULT AlgorithmDocument13 pagesTto COVID-19 TREATMENT ADULT Algorithmmissbear100% (1)
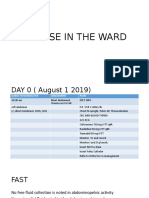
- Nursing NotesDocument7 pagesNursing NotesJayNo ratings yet
- Algorithm-ACLS ACS 200806 1Document1 pageAlgorithm-ACLS ACS 200806 1Kavya Shree100% (1)
- Medical Surgical ATI Review Flashcards - QuizletDocument27 pagesMedical Surgical ATI Review Flashcards - QuizletNursyNurseNo ratings yet
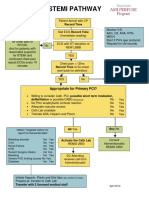
- STEMI Pathway FlowchartDocument2 pagesSTEMI Pathway FlowchartOlga Jadha CasmiraNo ratings yet
- Spinal Cord Injury Pathway AlgorithmDocument13 pagesSpinal Cord Injury Pathway Algorithmnurul ismaniaNo ratings yet
- Hydrocephalus Clinical PathwayDocument6 pagesHydrocephalus Clinical PathwayJayson OlileNo ratings yet
- Posters For ClinicDocument80 pagesPosters For ClinicdenzkissaieNo ratings yet
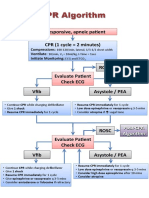
- CPR Algorithm3Document1 pageCPR Algorithm3MarinaJiménezNo ratings yet
- CPR Algorithm GuideDocument1 pageCPR Algorithm GuideTiago RodriguesNo ratings yet
- Syndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital PreparationDocument1 pageSyndromes Suggestive of Ischemia or Infarction: EMS Assessment and Care and Hospital Preparationgusti angri angalanNo ratings yet
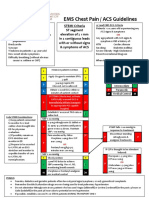
- EMS Chest Pain ACS GuidelinesDocument1 pageEMS Chest Pain ACS GuidelinesJuanaly BadiolaNo ratings yet
- CHD Care Guideline With Extended Version and PfeDocument12 pagesCHD Care Guideline With Extended Version and PfeSorin IordacheNo ratings yet
- PMLS 2 Unit 5.2Document1 pagePMLS 2 Unit 5.2Elyon Jirehel AlvarezNo ratings yet
- SVN 2021 001321Document5 pagesSVN 2021 001321viva dialysisNo ratings yet
- Resume: Hyperthyroid Perioperative ManagementDocument4 pagesResume: Hyperthyroid Perioperative ManagementWilujeng AnggrainiNo ratings yet
- INHALATION ANESTHETIC DRUG ORDER, MODE OF ACTION, INDICATIONS AND CONTRAINDICATIONSDocument2 pagesINHALATION ANESTHETIC DRUG ORDER, MODE OF ACTION, INDICATIONS AND CONTRAINDICATIONSGil GanibanNo ratings yet
- EHC ED Critical Care Induced Hypothermia ProtocolDocument4 pagesEHC ED Critical Care Induced Hypothermia ProtocolmaddythedocNo ratings yet
- Case-Based Device Therapy for Heart FailureFrom EverandCase-Based Device Therapy for Heart FailureUlrika Birgersdotter-GreenNo ratings yet
- Food and Beverages Shoes and Clothes Beauty Products Services EntertainmentDocument5 pagesFood and Beverages Shoes and Clothes Beauty Products Services EntertainmentRonibeMalinginNo ratings yet
- Cystocentesis K4Document24 pagesCystocentesis K4Sze KhayNo ratings yet
- Echo - Medical Supplies and Equipment For Primary Health CareDocument192 pagesEcho - Medical Supplies and Equipment For Primary Health CareKing Solomon CatralNo ratings yet
- Revision 2Document7 pagesRevision 2Maina JonnNo ratings yet
- Coe, & Vandegrift. 2015 (Youth Politics and Culture in Contemporary LA A Review)Document23 pagesCoe, & Vandegrift. 2015 (Youth Politics and Culture in Contemporary LA A Review)Alejandro MolinaNo ratings yet
- Flow RateDocument2 pagesFlow Rateفيرمان ريشادNo ratings yet
- Flow rate uniformity of TARAL 200 PITON TURBO sprayer for pest controlDocument4 pagesFlow rate uniformity of TARAL 200 PITON TURBO sprayer for pest controlAndreea DiaconuNo ratings yet
- NPCC Newsletter Nov 2016Document38 pagesNPCC Newsletter Nov 2016sarvesh14111984No ratings yet
- Soal Analytical ExpositionDocument17 pagesSoal Analytical ExpositionHilmi Muhammad AbduhNo ratings yet
- How To Know If U Need Ortho TTDocument3 pagesHow To Know If U Need Ortho TTSubhajit SahaNo ratings yet
- Neurodegenerative Disease Among Male Elite Football (Soccer) Players in Sweden: A Cohort Study - TheDocument3 pagesNeurodegenerative Disease Among Male Elite Football (Soccer) Players in Sweden: A Cohort Study - Thepitufi11No ratings yet
- CBT therapy overview: strengths, sessions, evidenceDocument1 pageCBT therapy overview: strengths, sessions, evidencezulkaberNo ratings yet
- National Polio Lab ChecklistDocument12 pagesNational Polio Lab ChecklistSelaina NawadraNo ratings yet
- HKGC Booklet FinalDocument95 pagesHKGC Booklet FinalAtik Badshah SHAIKHNo ratings yet
- Chapter 6 - Adipose TissueDocument13 pagesChapter 6 - Adipose TissueREMAN ALINGASANo ratings yet
- Anju Jose CV LatestDocument3 pagesAnju Jose CV LatestRafi Pk0% (1)
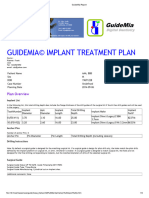
- GuideMia Sample Report - EnglishDocument9 pagesGuideMia Sample Report - Englishzhiao liuNo ratings yet
- How to Don and Doff Sterile Gloves SafelyDocument32 pagesHow to Don and Doff Sterile Gloves SafelyCoreen Mangaoang83% (6)
- Cataract Case GuideDocument3 pagesCataract Case GuideVetrivel Tamizh100% (1)
- Position PaperDocument2 pagesPosition Paperapi-340817333No ratings yet
- Oum Business School: Matriculation No: Identity Card No.: Telephone No.: E-Mail: Learning CentreDocument6 pagesOum Business School: Matriculation No: Identity Card No.: Telephone No.: E-Mail: Learning CentreInspire28No ratings yet
- Two Factor Theory Motivation-Hygiene Theory: Dual-Factor Theory/ Theory of Work Behavior byDocument16 pagesTwo Factor Theory Motivation-Hygiene Theory: Dual-Factor Theory/ Theory of Work Behavior byAngha0% (1)
- Phase III CT in Alzheimer's DiseaseDocument13 pagesPhase III CT in Alzheimer's DiseaseKlesta Durović100% (1)
- R-07 Behaviour Policy (1536) PDFDocument1 pageR-07 Behaviour Policy (1536) PDFAmerNo ratings yet
- Quick RemapDocument32 pagesQuick RemapmollitonyNo ratings yet
- Acute Pain Questions - LathaDocument5 pagesAcute Pain Questions - LathaNishanth yedavalliNo ratings yet
- ISCO-08 Part 4: Correspondence TablesDocument75 pagesISCO-08 Part 4: Correspondence TableslivelongerNo ratings yet
- Project SarvodayaDocument21 pagesProject SarvodayaArun Kumar PNo ratings yet
- And Netflix Show, Ask The Storybots, Now Star in Their Own Board Books!Document2 pagesAnd Netflix Show, Ask The Storybots, Now Star in Their Own Board Books!kagnejukkeNo ratings yet
- Lembar Jawaban Skill Lab Evidence Based Medicine (Ebm) Nama: Muhammad Fadill Akbar NIM: 04011281621080Document20 pagesLembar Jawaban Skill Lab Evidence Based Medicine (Ebm) Nama: Muhammad Fadill Akbar NIM: 04011281621080Ya'kubNo ratings yet