You might also like
- MH Exam 2 Study GuideDocument24 pagesMH Exam 2 Study Guidewn4tb100% (1)
- RFH COVID-19 ICU Resource Pack FULL PDFDocument15 pagesRFH COVID-19 ICU Resource Pack FULL PDFQuique GarciaNo ratings yet
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
- HEALTH ASSESSMENT - BatteryDocument20 pagesHEALTH ASSESSMENT - BatteryJoana Grace Cortez100% (1)
- Ynhhs - Covid-19 Treatment Adult Algorithm 4.3.20Document10 pagesYnhhs - Covid-19 Treatment Adult Algorithm 4.3.20Ren SNo ratings yet
- COVID-19 TREATMENT ADULT Algorithm 4.3.20Document10 pagesCOVID-19 TREATMENT ADULT Algorithm 4.3.20luizfelipenobresc5492100% (1)
- YNHHS Adult Treatment Algorithm 05132020 - 382832 - 5 - v5Document20 pagesYNHHS Adult Treatment Algorithm 05132020 - 382832 - 5 - v5nuelitopNo ratings yet
- Clinical Guideline For Management of Acute Pancreatitis in AdultsDocument13 pagesClinical Guideline For Management of Acute Pancreatitis in AdultsrivaldiNo ratings yet
- COVID-19 Antiviral TX Guidance 4-22-2020Document23 pagesCOVID-19 Antiviral TX Guidance 4-22-2020Lydia IsaacNo ratings yet
- AIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaSomnath Das GuptaNo ratings yet
- ACLS ACS Algorithm NewDocument3 pagesACLS ACS Algorithm Newsambo100% (1)
- Kak Kar MintolDocument4 pagesKak Kar Mintoltrisna minNo ratings yet
- Febrile Neutropenia Care GuidelineDocument2 pagesFebrile Neutropenia Care GuidelinedenokayuMRNo ratings yet
- CCU HandoverDocument9 pagesCCU Handoverapi-192342497No ratings yet
- Clinical Guideline For Management of Acute Cholecystitis in AdultsDocument9 pagesClinical Guideline For Management of Acute Cholecystitis in AdultsPutria Rezki ArgathyaNo ratings yet
- Clinical Guideline For Management of Acute Cholecystitis in AdultsDocument9 pagesClinical Guideline For Management of Acute Cholecystitis in AdultsGaby D'LuneNo ratings yet
- Screenshot 2020-03-20 at 08.25.44 PDFDocument10 pagesScreenshot 2020-03-20 at 08.25.44 PDFMiguel Angel Palacios FloresNo ratings yet
- Clinical Pathway StrokeDocument8 pagesClinical Pathway StrokedjizhieeNo ratings yet
- Severe TBI 2017Document18 pagesSevere TBI 2017DM internaNo ratings yet
- Guidelines For First-Line Empirical Antibiotic Therapy in AdultsDocument1 pageGuidelines For First-Line Empirical Antibiotic Therapy in AdultsAnonymous s4yarxNo ratings yet
- FINAL COVID19 1 April 2021Document14 pagesFINAL COVID19 1 April 2021Wleed KhledNo ratings yet
- UH Treatment Protocol Edit 6 March 24 2020Document9 pagesUH Treatment Protocol Edit 6 March 24 2020zeeNo ratings yet
- OSCE EmergencyDocument26 pagesOSCE EmergencyXu PeihaoNo ratings yet
- 07 - 10 - 21 Treatment of Covid 19 InfectionDocument26 pages07 - 10 - 21 Treatment of Covid 19 InfectionStonefalconNo ratings yet
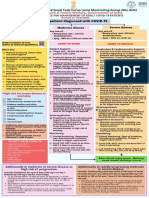
- Adult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAdult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of Indiapramodbankhele3845No ratings yet
- Emergency Laparotomy PDFDocument13 pagesEmergency Laparotomy PDFbushra mughalNo ratings yet
- Deep Vein Thrombosis - 2003Document34 pagesDeep Vein Thrombosis - 2003farmasi_hm100% (1)
- CovidDocument31 pagesCovidShaheen SultanNo ratings yet
- Management of Common Cases in Emergency MedicineDocument55 pagesManagement of Common Cases in Emergency MedicinemonpyitharNo ratings yet
- O&G TestDocument8 pagesO&G TestMilo PingNo ratings yet
- MIS C Algorithim Version 2Document8 pagesMIS C Algorithim Version 2Saima UmairNo ratings yet
- COVID19 Management Algorithm 22042021 v1Document1 pageCOVID19 Management Algorithm 22042021 v1shivani shindeNo ratings yet
- Pediatrics MS WordDocument13 pagesPediatrics MS WordSamhitha SharmaNo ratings yet
- Spontaneous Awakening Trial PDFDocument1 pageSpontaneous Awakening Trial PDFyonoNo ratings yet
- COVID MX BsmmuDocument2 pagesCOVID MX BsmmuNuhiat NahreenNo ratings yet
- Anesthetic ComplicationsDocument28 pagesAnesthetic ComplicationsSamuel RealesNo ratings yet
- Management of Status Epilepticus 2022Document8 pagesManagement of Status Epilepticus 2022albert siraitNo ratings yet
- AMI CP EnglishDocument1 pageAMI CP EnglishNovema AsharNo ratings yet
- Afib Protocol Exclusion CriteriaDocument3 pagesAfib Protocol Exclusion CriteriaJesse M. MassieNo ratings yet
- AIIMS Issues New Guidelines For Treatment of CovidDocument7 pagesAIIMS Issues New Guidelines For Treatment of Covidsenthil kumarNo ratings yet
- NRG Gy023Document7 pagesNRG Gy023Yagami SinNo ratings yet
- AIIMS Issues New Guidelines For Treatment of Covid-19 Cases: (Enter Post Title Here)Document7 pagesAIIMS Issues New Guidelines For Treatment of Covid-19 Cases: (Enter Post Title Here)senthil kumarNo ratings yet
- COPD Guideline Ver 1.8Document9 pagesCOPD Guideline Ver 1.8Dina AyupnNo ratings yet
- 7902-002 Investigators Meeting Material 08 Feb 2019Document39 pages7902-002 Investigators Meeting Material 08 Feb 2019FERNANDO BUSTAMANTE MORALESNo ratings yet
- Indications of ICU Admission and ICU Management of COVID 19 NEWDocument27 pagesIndications of ICU Admission and ICU Management of COVID 19 NEWMidhat FatmaNo ratings yet
- Asthma Clinical Care GuidelinesDocument17 pagesAsthma Clinical Care GuidelinesWalaa MoustafaNo ratings yet
- SCE Practicaldiabetes - ElzohryDocument251 pagesSCE Practicaldiabetes - ElzohryAE100% (1)
- 1614978209sampleDocument9 pages1614978209sampleReddyNo ratings yet
- 林奕廷 - perioperative management of TSSDocument15 pages林奕廷 - perioperative management of TSS林奕廷No ratings yet
- Antibiotic Pocket GuideDocument19 pagesAntibiotic Pocket GuideNaomi Liang100% (1)
- Sepsis: Nirav Mistry, MD and Adel Bassily-Marcus, MD, FCCP, FCCMDocument3 pagesSepsis: Nirav Mistry, MD and Adel Bassily-Marcus, MD, FCCP, FCCMAli AftabNo ratings yet
- GDL Fever OncologyDocument16 pagesGDL Fever OncologyZaini GhazaliNo ratings yet
- Traumatic Brain Injury 2023Document17 pagesTraumatic Brain Injury 2023Fernando Martinez AguilarNo ratings yet
- Just The Facts: Massive Hemorrhage Protocol: Clinical ScenarioDocument3 pagesJust The Facts: Massive Hemorrhage Protocol: Clinical ScenarioIsraelNo ratings yet
- Current Clinical Strategies: Handbook of AnesthesiologyDocument180 pagesCurrent Clinical Strategies: Handbook of AnesthesiologydramaganaNo ratings yet
- SurgeryDocument30 pagesSurgeryLuai Tuma KhouryNo ratings yet
- Acute ColitisDocument8 pagesAcute ColitisKhurram NadeemNo ratings yet
- Anaesthetic Management of PheochromocytomaDocument22 pagesAnaesthetic Management of PheochromocytomaZoelNo ratings yet
- NIV ProformaDocument10 pagesNIV ProformaWael N Sh GadallaNo ratings yet
- Pediatric Acute Sepsis: Physician'S OrdersDocument4 pagesPediatric Acute Sepsis: Physician'S OrdersSughosh MitraNo ratings yet
- International Journal of Surgery Case Reports: Unusual Esophageal Foreign Body in Neonates: A Case ReportDocument4 pagesInternational Journal of Surgery Case Reports: Unusual Esophageal Foreign Body in Neonates: A Case ReportmusdalifahNo ratings yet
- Continuous Renal Replacement Therapy Education PackDocument18 pagesContinuous Renal Replacement Therapy Education PacktsongtonsgNo ratings yet
- Vidradhi in B Hat-Trayī A Critical Review of LiteratureDocument8 pagesVidradhi in B Hat-Trayī A Critical Review of LiteratureInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- NACO ART Guidelines 2013Document122 pagesNACO ART Guidelines 2013RohitKumarNo ratings yet
- Be in Precision Medicine: Project CoordinatorDocument2 pagesBe in Precision Medicine: Project CoordinatorKirsten HartmanNo ratings yet
- SadsadDocument3 pagesSadsadDalo ZeronNo ratings yet
- BTS ILD Registry Annual Report 2021Document38 pagesBTS ILD Registry Annual Report 2021Rana Khaled AwwadNo ratings yet
- Edition 4.0: Please Input The Below Numbers : Subject-Wise Study Time CalculatorDocument2 pagesEdition 4.0: Please Input The Below Numbers : Subject-Wise Study Time CalculatorAnjela BaidyaNo ratings yet
- Type 2 Diabetes The Lancet 2022Document18 pagesType 2 Diabetes The Lancet 2022Valentina Kerguelen HernándezNo ratings yet
- Ultrasound in The Critically Ill - HGGDocument4 pagesUltrasound in The Critically Ill - HGGFranz MiguelNo ratings yet
- k2 Stom F EngDocument28 pagesk2 Stom F Engdmd1983aminNo ratings yet
- DRUG STUDY Cefu and Keto and SummaryDocument8 pagesDRUG STUDY Cefu and Keto and SummaryAmanie Usman AmanoddinNo ratings yet
- Clinical Practice Guidelines On Hepatitis Delta VirusDocument28 pagesClinical Practice Guidelines On Hepatitis Delta VirusRadu IonescuNo ratings yet
- Phaco / Lasik - Hands On Training in India: I Care ConsultantsDocument3 pagesPhaco / Lasik - Hands On Training in India: I Care ConsultantsicareconsultantsNo ratings yet
- Training Module For Management of Breast CancerDocument4 pagesTraining Module For Management of Breast CancerhakimahsNo ratings yet
- Mapeh Submitt Ed by Sophia Hailey T. Plaza: ScrapbookDocument8 pagesMapeh Submitt Ed by Sophia Hailey T. Plaza: ScrapbookNimfat PlazaNo ratings yet
- Mediplant PDFDocument58 pagesMediplant PDFDnyaneshwar Dattatraya Phadatare100% (1)
- University Grants CommissionDocument25 pagesUniversity Grants CommissionAvijit DebnathNo ratings yet
- Annals of XII International Symposium On Vasoactive PeptidesDocument99 pagesAnnals of XII International Symposium On Vasoactive PeptidesDaisy Motta SantosNo ratings yet
- Understanding Diabetes: Prevention Better Than CureDocument44 pagesUnderstanding Diabetes: Prevention Better Than CureJUANANo ratings yet
- 2019 - Health Promoting Lifestyle and Its Determinants Among FemaleDocument6 pages2019 - Health Promoting Lifestyle and Its Determinants Among FemaleSubhan AnsariNo ratings yet
- Intrauterine Growth RestrictionDocument5 pagesIntrauterine Growth RestrictionColleen MercadoNo ratings yet
- Breast FeedingDocument6 pagesBreast FeedingphobicmdNo ratings yet
- Regenerative Medicine From Protocol To PatientDocument257 pagesRegenerative Medicine From Protocol To PatientMandraludin0% (1)
- Paediatric Lecture Guide by Obasi Chinedu-1 PDFDocument390 pagesPaediatric Lecture Guide by Obasi Chinedu-1 PDFsamycoolqNo ratings yet
- Homeo-11 RrUBRICSDocument32 pagesHomeo-11 RrUBRICSRashid MahmoodNo ratings yet
- Chest TraumaDocument52 pagesChest TraumaSllavko K. KallfaNo ratings yet
- Navjyoti Suri 84-Herdwick Street Brampton, ON. L6S 6M1 (647) 287 2618Document4 pagesNavjyoti Suri 84-Herdwick Street Brampton, ON. L6S 6M1 (647) 287 2618api-314566363No ratings yet