You might also like
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
- Appendix 4b - NIV Algorithm (ICHT)Document1 pageAppendix 4b - NIV Algorithm (ICHT)Josi JeremiaNo ratings yet
- BipapDocument26 pagesBipapTnem NatNo ratings yet
- RFH COVID-19 ICU Resource Pack FULL PDFDocument15 pagesRFH COVID-19 ICU Resource Pack FULL PDFQuique GarciaNo ratings yet
- NIV Algorithm Final Version Jan 2020Document3 pagesNIV Algorithm Final Version Jan 2020AmalNo ratings yet
- AIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaSomnath Das GuptaNo ratings yet
- COVID-19 Management ProtocolDocument13 pagesCOVID-19 Management ProtocolajiNo ratings yet
- Niv in CopdDocument54 pagesNiv in Copdmahmod omerNo ratings yet
- Management of Acute Respiratory Failure in COVID-PUI Patient - Updated Feb. 2021Document7 pagesManagement of Acute Respiratory Failure in COVID-PUI Patient - Updated Feb. 2021Abhishek GoelNo ratings yet
- NIV and HFNCDocument16 pagesNIV and HFNCMarceline GarciaNo ratings yet
- BiPAP ManyDocument47 pagesBiPAP ManyHarshit RastogiNo ratings yet
- DR - Rajalakshmi.C: Emergency Physician MMHRC Institute of Emergency MedicineDocument22 pagesDR - Rajalakshmi.C: Emergency Physician MMHRC Institute of Emergency MedicineP Vinod KumarNo ratings yet
- COVID-19 Guidelines for Management of PatientsDocument2 pagesCOVID-19 Guidelines for Management of PatientsSpecial OPD SVMCHRCNo ratings yet
- Ventilator Management ProtocolDocument15 pagesVentilator Management Protocolihtisham1No ratings yet
- COVID-19 Protocol KGMU Version 6.0 17-4-21Document34 pagesCOVID-19 Protocol KGMU Version 6.0 17-4-21Kirtivaan MishraNo ratings yet
- Asthma Clinical Care GuidelinesDocument17 pagesAsthma Clinical Care GuidelinesWalaa MoustafaNo ratings yet
- Peds Clinical Cases (Egypt) 3-09 (Final Version)Document57 pagesPeds Clinical Cases (Egypt) 3-09 (Final Version)asupicuNo ratings yet
- FINAL COVID19 1 April 2021Document14 pagesFINAL COVID19 1 April 2021Wleed KhledNo ratings yet
- COVID-19 Management of Critical Care Cases PDFDocument6 pagesCOVID-19 Management of Critical Care Cases PDFLubna AliNo ratings yet
- AIIMS issues new guidelines for treatment of Covid-19 casesDocument7 pagesAIIMS issues new guidelines for treatment of Covid-19 casessenthil kumarNo ratings yet
- AIIMS Issues New Guidelines For Treatment of CovidDocument7 pagesAIIMS Issues New Guidelines For Treatment of Covidsenthil kumarNo ratings yet
- Bipap Ventilation Basic and MonitoringDocument33 pagesBipap Ventilation Basic and MonitoringPradip ChougaleNo ratings yet
- Weaning ProtocolDocument6 pagesWeaning ProtocolerwanNo ratings yet
- COVID19 Management Algorithm 22042021 v1Document1 pageCOVID19 Management Algorithm 22042021 v1shivani shindeNo ratings yet
- SOP COVID ManagementDocument10 pagesSOP COVID ManagementJerryNo ratings yet
- Vincent Brody Care PlanDocument10 pagesVincent Brody Care PlanKarina Rodriguez50% (2)
- Documentation in Your 3 Year and Beyond: Summer Quarter 2010Document32 pagesDocumentation in Your 3 Year and Beyond: Summer Quarter 2010Roberto ParedesNo ratings yet
- HFNC Guidelines AustraliaDocument13 pagesHFNC Guidelines AustraliaMASIEL AMELIA BARRANTES ARCENo ratings yet
- BipapDocument26 pagesBipapالغائب الحاضرNo ratings yet
- Sedation in Critically IllDocument32 pagesSedation in Critically IllSamantha Deshapriya100% (1)
- NPPVDocument29 pagesNPPVStephanie SusavageNo ratings yet
- Guideline For Management Protocol of Children With Fever and Respiratory SymptomsDocument44 pagesGuideline For Management Protocol of Children With Fever and Respiratory SymptomsKushagr GautamNo ratings yet
- 01 - Bronchial AsthmaDocument6 pages01 - Bronchial AsthmaFrank VaronaNo ratings yet
- AnswersDocument4 pagesAnswersKhadijah AhmedNo ratings yet
- COPD Guideline Ver 1.8Document9 pagesCOPD Guideline Ver 1.8Dina AyupnNo ratings yet
- COVID-19 Antiviral TX Guidance 4-22-2020Document23 pagesCOVID-19 Antiviral TX Guidance 4-22-2020Lydia IsaacNo ratings yet
- Doctors OrderDocument9 pagesDoctors OrderReal TetisoraNo ratings yet
- Asthma v.3.0: Criteria and Respiratory ScoreDocument36 pagesAsthma v.3.0: Criteria and Respiratory ScoreYudha Astipamara PanjayaNo ratings yet
- 4 Weaning Ventilator-NIADocument31 pages4 Weaning Ventilator-NIAResyana Widyayani100% (1)
- Influenza A H1N1 Clinical Management Protocol: Public Health Department, MaharashtraDocument23 pagesInfluenza A H1N1 Clinical Management Protocol: Public Health Department, MaharashtraRajeev PareekNo ratings yet
- NIV (Non-Invasive Ventilation) : Dr.S.MagimaiguberanDocument38 pagesNIV (Non-Invasive Ventilation) : Dr.S.MagimaiguberanDr mahi sNo ratings yet
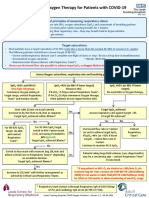
- Guidance on Oxygen Therapy for COVID-19 PatientsDocument1 pageGuidance on Oxygen Therapy for COVID-19 PatientsAsh mohamedNo ratings yet
- AECOPD GuidelineDocument1 pageAECOPD GuidelineOperations Manager - CMCNo ratings yet
- COVID-19 Therapeutics for Healthcare WorkersDocument9 pagesCOVID-19 Therapeutics for Healthcare Workers[JC]No ratings yet
- Sepsis Team Protocol2012Document4 pagesSepsis Team Protocol2012ratmanNo ratings yet
- Barnet Primary Care Covid-19 Guide V7.1Document32 pagesBarnet Primary Care Covid-19 Guide V7.1Greta Tanushi KukaNo ratings yet
- Sample Standardized Oral Exam Questions: Session 1 - 35 MinutesDocument4 pagesSample Standardized Oral Exam Questions: Session 1 - 35 MinutesManuela CormioNo ratings yet
- Spontaneous Awakening Trial PDFDocument1 pageSpontaneous Awakening Trial PDFyonoNo ratings yet
- Sellar Lesions Treatment OutcomesDocument15 pagesSellar Lesions Treatment Outcomes林奕廷No ratings yet
- Case For Study Hypertensive CrisisDocument2 pagesCase For Study Hypertensive CrisisRenarose SocitoNo ratings yet
- MANAGEMENT OF ACUTE ASTHMA ATTACKS IN ADULTSDocument1 pageMANAGEMENT OF ACUTE ASTHMA ATTACKS IN ADULTSMassimo Di BenedettoNo ratings yet
- Prone StudyDocument13 pagesProne StudySanketNandaniNo ratings yet
- Asthma PathwayDocument42 pagesAsthma PathwayVhony Purnamasari HNo ratings yet
- ICU Case: Septic Shock from Hospital-Acquired PneumoniaDocument13 pagesICU Case: Septic Shock from Hospital-Acquired PneumoniaHana FauziNo ratings yet
- CPAPDocument5 pagesCPAPraul gutierrezNo ratings yet
- Mechanical Vent in Covid 19 - DR BernadettDocument14 pagesMechanical Vent in Covid 19 - DR BernadettRajanNo ratings yet
- Important Notes V1.0Document4 pagesImportant Notes V1.0Dr.Abdirahman DahirNo ratings yet
- Cem6834 SobDocument2 pagesCem6834 SobimperiallightNo ratings yet
- Deonne Thaddeus V Gauiran PhilippinesDocument25 pagesDeonne Thaddeus V Gauiran PhilippinesKathrine Ann FavoritoNo ratings yet
- Patient Management Flow Chart: Appt W/ Bronchoscopist PFT/ P&H/StabilityDocument7 pagesPatient Management Flow Chart: Appt W/ Bronchoscopist PFT/ P&H/StabilityKinnari PatelNo ratings yet
- Transmitting AKI Warning Stage Data To The UKRR FinalDocument8 pagesTransmitting AKI Warning Stage Data To The UKRR FinalWael N Sh GadallaNo ratings yet
- Psa Aki AlgDocument2 pagesPsa Aki AlgWael N Sh GadallaNo ratings yet
- Sheffield Hospital Surgical Care Guidelines For AKIDocument53 pagesSheffield Hospital Surgical Care Guidelines For AKIWael N Sh GadallaNo ratings yet
- 19 October 2022 IMT Skills 3.0Document2 pages19 October 2022 IMT Skills 3.0Wael N Sh GadallaNo ratings yet
- Family Medicine FinalDocument35 pagesFamily Medicine Finalzdfdgsdgsh sggaesgs0% (1)
- SBA Questions Revision Cardiovascular PhysiologyDocument65 pagesSBA Questions Revision Cardiovascular PhysiologyminayokiNo ratings yet
- Respiratory SystemDocument19 pagesRespiratory SystemayuNo ratings yet
- Pulmonary Diseases & Respiratory System AnatomyDocument6 pagesPulmonary Diseases & Respiratory System AnatomyJada NovakNo ratings yet
- Dutch COPD Physiotherapy Guidelines PDFDocument64 pagesDutch COPD Physiotherapy Guidelines PDFyohanNo ratings yet
- SpiroCard BrochureDocument2 pagesSpiroCard BrochureEdward Gustavo González MotavitaNo ratings yet
- Troubleshooting Problem SolvingDocument22 pagesTroubleshooting Problem SolvingM Agung Fatahillah100% (1)
- PFT Final Exam Study Guide & Practice QuestionsDocument38 pagesPFT Final Exam Study Guide & Practice QuestionsJade Louise FkshmNo ratings yet
- COPD NEW GuidelinesDocument45 pagesCOPD NEW GuidelinesMuhammad HaneefNo ratings yet
- Aerodynamic Measurements in Dysarthria: Dr. SwapnaDocument45 pagesAerodynamic Measurements in Dysarthria: Dr. SwapnaAppas SahaNo ratings yet
- PEBC Evaluating Exam Mustpass Misbah 2016 PDFDocument437 pagesPEBC Evaluating Exam Mustpass Misbah 2016 PDFKathryn Mitchell100% (3)
- Managing and Preventing Asthma in ChildrenDocument30 pagesManaging and Preventing Asthma in ChildrenJavier SaadNo ratings yet
- 1 - Spirometry Simplified With CRF's PEFR PDFDocument80 pages1 - Spirometry Simplified With CRF's PEFR PDFyayatiNo ratings yet
- Pulmonary Function TestsDocument57 pagesPulmonary Function Testsmerin sunilNo ratings yet
- Depression, lung function, and BODE index in COPDDocument16 pagesDepression, lung function, and BODE index in COPDHera HeraNo ratings yet
- Anaesthesia For Thoracic Surgery: DR Fazal H KhanDocument4 pagesAnaesthesia For Thoracic Surgery: DR Fazal H KhanAdeebMutawaNo ratings yet
- TaniaDocument14 pagesTaniaOm SharmaNo ratings yet
- Calibration Vs AccuracyDocument2 pagesCalibration Vs AccuracyMihai PetrescuNo ratings yet
- Spiro 7Document17 pagesSpiro 7Bulborea MihaelaNo ratings yet
- Wisloff, U. & Cols. (2005)Document5 pagesWisloff, U. & Cols. (2005)Mario0405No ratings yet
- เฉลยข้อสอบ MCQ R2ครั้งที่2Document362 pagesเฉลยข้อสอบ MCQ R2ครั้งที่2Kareem Sukwihan100% (2)
- E DAR Filter CatalogDocument38 pagesE DAR Filter CatalogJittiya WatcharotayangulNo ratings yet
- Hyperbaric Oxygen Therapy Effects On Pulmonary FunDocument6 pagesHyperbaric Oxygen Therapy Effects On Pulmonary Funvalensia melinaNo ratings yet
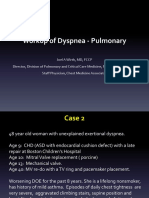
- DyspneaDocument35 pagesDyspneaEnvhy AmaliaNo ratings yet
- Effects of Smoking on Lung CapacityDocument9 pagesEffects of Smoking on Lung CapacityMohammad MashhoodNo ratings yet
- MGC Diagnostics Platinum Elite Service ManualDocument165 pagesMGC Diagnostics Platinum Elite Service ManualJovanović DunjaNo ratings yet
- Respiratory System Upper Respiratory DiseasesDocument32 pagesRespiratory System Upper Respiratory DiseasesPrince Rener Velasco Pera100% (1)
- A-Level: Biology (7402/1)Document24 pagesA-Level: Biology (7402/1)Ronald WalburnNo ratings yet
- Welch Allyn CP-200 Spirometer - User ManualDocument92 pagesWelch Allyn CP-200 Spirometer - User ManualAhmad ShahNo ratings yet