You might also like
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
- Ynhhs - Covid-19 Treatment Adult Algorithm 4.3.20Document10 pagesYnhhs - Covid-19 Treatment Adult Algorithm 4.3.20Ren SNo ratings yet
- Tto COVID-19 TREATMENT ADULT AlgorithmDocument13 pagesTto COVID-19 TREATMENT ADULT Algorithmmissbear100% (1)
- YNHHS Adult Treatment Algorithm 05132020 - 382832 - 5 - v5Document20 pagesYNHHS Adult Treatment Algorithm 05132020 - 382832 - 5 - v5nuelitopNo ratings yet
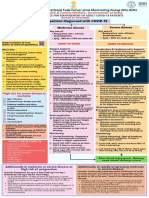
- AIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaSomnath Das GuptaNo ratings yet
- ACLS ACS Algorithm NewDocument3 pagesACLS ACS Algorithm Newsambo100% (1)
- Febrile Neutropenia Care GuidelineDocument2 pagesFebrile Neutropenia Care GuidelinedenokayuMRNo ratings yet
- Clinical Guideline For Management of Acute Pancreatitis in AdultsDocument13 pagesClinical Guideline For Management of Acute Pancreatitis in AdultsrivaldiNo ratings yet
- COVID-19 Antiviral TX Guidance 4-22-2020Document23 pagesCOVID-19 Antiviral TX Guidance 4-22-2020Lydia IsaacNo ratings yet
- Pediatric Guidelines for MIS-CDocument8 pagesPediatric Guidelines for MIS-CSaima UmairNo ratings yet
- Management of Common Cases in Emergency MedicineDocument55 pagesManagement of Common Cases in Emergency MedicinemonpyitharNo ratings yet
- OSCE EmergencyDocument26 pagesOSCE EmergencyXu PeihaoNo ratings yet
- Screenshot 2020-03-20 at 08.25.44 PDFDocument10 pagesScreenshot 2020-03-20 at 08.25.44 PDFMiguel Angel Palacios FloresNo ratings yet
- Kak Kar MintolDocument4 pagesKak Kar Mintoltrisna minNo ratings yet
- UH Treatment Protocol Edit 6 March 24 2020Document9 pagesUH Treatment Protocol Edit 6 March 24 2020zeeNo ratings yet
- COVID19 Management Algorithm 22042021 v1Document1 pageCOVID19 Management Algorithm 22042021 v1shivani shindeNo ratings yet
- AMI CP EnglishDocument1 pageAMI CP EnglishNovema AsharNo ratings yet
- Clinical Pathway StrokeDocument8 pagesClinical Pathway StrokedjizhieeNo ratings yet
- Adult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAdult Patient Diagnosed With COVID-19: Ministry of Health & Family Welfare, Government of Indiapramodbankhele3845No ratings yet
- Guidelines For First-Line Empirical Antibiotic Therapy in AdultsDocument1 pageGuidelines For First-Line Empirical Antibiotic Therapy in AdultsAnonymous s4yarxNo ratings yet
- Management of Status Epilepticus 2022Document8 pagesManagement of Status Epilepticus 2022albert siraitNo ratings yet
- Pediatric Acute Sepsis: Physician'S OrdersDocument4 pagesPediatric Acute Sepsis: Physician'S OrdersSughosh MitraNo ratings yet
- Resume: Hyperthyroid Perioperative ManagementDocument4 pagesResume: Hyperthyroid Perioperative ManagementWilujeng AnggrainiNo ratings yet
- Treating Febrile NeutropeniaDocument2 pagesTreating Febrile NeutropeniaAlvy SyukrieNo ratings yet
- Pediatrics MS WordDocument13 pagesPediatrics MS WordSamhitha SharmaNo ratings yet
- Clinical Guideline For Management of Acute Cholecystitis in AdultsDocument9 pagesClinical Guideline For Management of Acute Cholecystitis in AdultsGaby D'LuneNo ratings yet
- Clinical Guideline For Management of Acute Cholecystitis in AdultsDocument9 pagesClinical Guideline For Management of Acute Cholecystitis in AdultsPutria Rezki ArgathyaNo ratings yet
- Sellar Lesions Treatment OutcomesDocument15 pagesSellar Lesions Treatment Outcomes林奕廷No ratings yet
- M10 Standards MVD Management DR C AtkinsDocument26 pagesM10 Standards MVD Management DR C Atkinsveterinaria87No ratings yet
- Anesthetic ComplicationsDocument28 pagesAnesthetic ComplicationsSamuel RealesNo ratings yet
- NIV ProformaDocument10 pagesNIV ProformaWael N Sh GadallaNo ratings yet
- Brajac - ProtocolDocument13 pagesBrajac - Protocolthanh ngôNo ratings yet
- Management Protocol of Septic Shock: DiagnosisDocument3 pagesManagement Protocol of Septic Shock: Diagnosissky nutsNo ratings yet
- Emergency Laparotomy PDFDocument13 pagesEmergency Laparotomy PDFbushra mughalNo ratings yet
- QR Dengue Infection PDF Final PDFDocument8 pagesQR Dengue Infection PDF Final PDFina2407jrNo ratings yet
- Step 3 NotesDocument4 pagesStep 3 Notesjhk0428No ratings yet
- Model Test-1 SolveDocument20 pagesModel Test-1 SolveRaihanShaheedNo ratings yet
- COVID-19 Treatment GuidelinesDocument26 pagesCOVID-19 Treatment GuidelinesStonefalconNo ratings yet
- CCU HandoverDocument9 pagesCCU Handoverapi-192342497No ratings yet
- MR Muh. Arafah TB (Autosaved)Document14 pagesMR Muh. Arafah TB (Autosaved)tiarapolarisiriuzNo ratings yet
- Severe TBI 2017Document18 pagesSevere TBI 2017DM internaNo ratings yet
- FINAL COVID19 1 April 2021Document14 pagesFINAL COVID19 1 April 2021Wleed KhledNo ratings yet
- Rev Angel - Konsulan SupriadiDocument1 pageRev Angel - Konsulan SupriadiDoctoRides 46No ratings yet
- Pomr Dewi 190919Document6 pagesPomr Dewi 190919emjehNo ratings yet
- Kegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungDocument47 pagesKegawatdaruratan Bidang Ilmu Penyakit Dalam: I.Penyakit Dalam - MIC/ICU FK - UNPAD - RS DR - Hasan Sadikin BandungEfa FathurohmiNo ratings yet
- Morning Report: Date: Monday, 8 March 2021Document3 pagesMorning Report: Date: Monday, 8 March 2021Adinda DianNo ratings yet
- Deep Vein Thrombosis - 2003Document34 pagesDeep Vein Thrombosis - 2003farmasi_hm100% (1)
- CPG Management of Dengue Infection in Adults (3rd Edition) : December 2015Document9 pagesCPG Management of Dengue Infection in Adults (3rd Edition) : December 2015Zaidatul Atiqah MustafaNo ratings yet
- How To Stratify The Risk and When To Refer: NsteacsDocument28 pagesHow To Stratify The Risk and When To Refer: NsteacsRatna TambaNo ratings yet
- Chest Pain System - DisorderDocument1 pageChest Pain System - DisorderAA DDNo ratings yet
- CovidDocument31 pagesCovidShaheen SultanNo ratings yet
- O&G TestDocument8 pagesO&G TestMilo PingNo ratings yet
- Program Studi Pendidikan Spesialis Ilmu Penyakit Dalam: Fakultas Kedokteran Universitas BrawijayaDocument3 pagesProgram Studi Pendidikan Spesialis Ilmu Penyakit Dalam: Fakultas Kedokteran Universitas BrawijayaHelsa EldatarinaNo ratings yet
- Dr. Firdha's Morning Report on ER Patient with CKD, HF & CAPDocument4 pagesDr. Firdha's Morning Report on ER Patient with CKD, HF & CAPFirdha RositaNo ratings yet
- Journal Round Up Q4 2019Document2 pagesJournal Round Up Q4 2019WillNo ratings yet
- Therapeutics Gastro BlockDocument23 pagesTherapeutics Gastro BlockAngelique Mae Mortejo SalarzaNo ratings yet
- Acs With New Stemi GuidelineDocument35 pagesAcs With New Stemi Guidelinematmin07No ratings yet
- PROBLEM ORIENTED MEDICAL RECORD FOR ACUTE KIDNEY INJURY MANAGEMENTDocument1 pagePROBLEM ORIENTED MEDICAL RECORD FOR ACUTE KIDNEY INJURY MANAGEMENTFirdha RositaNo ratings yet
- Novation SL MKii English GuideDocument37 pagesNovation SL MKii English GuidefadythebassistNo ratings yet
- Dipnech ThoraxDocument5 pagesDipnech Thoraxluizfelipenobresc5492No ratings yet
- DIPNECH ErjournalsDocument13 pagesDIPNECH Erjournalsluizfelipenobresc5492No ratings yet
- Dipnech BJR 2018Document3 pagesDipnech BJR 2018luizfelipenobresc5492No ratings yet
- DIPNECH: When To Suggest This Diagnosis On CTDocument9 pagesDIPNECH: When To Suggest This Diagnosis On CTluizfelipenobresc5492No ratings yet
- Reversed Halo Sign in Invasive Fungal InfectionsDocument1 pageReversed Halo Sign in Invasive Fungal Infectionsluizfelipenobresc5492No ratings yet
- A Role For CT in COVID-19 - Lancet PDFDocument1 pageA Role For CT in COVID-19 - Lancet PDFluizfelipenobresc5492No ratings yet
- Primary Pulmonary Rhabdomyosarcoma Arising Within Cystic Adenomatoid Malformation: A Case Report and Review of The LiteratureDocument4 pagesPrimary Pulmonary Rhabdomyosarcoma Arising Within Cystic Adenomatoid Malformation: A Case Report and Review of The Literatureluizfelipenobresc5492No ratings yet
- Position Paper: Lancet Respir Med 2020Document12 pagesPosition Paper: Lancet Respir Med 2020luizfelipenobresc5492No ratings yet
- 2011-Expanded CatalogDocument9 pages2011-Expanded Catalogluizfelipenobresc5492No ratings yet
- Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia: A Case Report and Review of The LiteratureDocument5 pagesDiffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia: A Case Report and Review of The Literatureluizfelipenobresc5492No ratings yet
- Chapter 14A Pituitary Adenomas and CraniopharyngiomasDocument8 pagesChapter 14A Pituitary Adenomas and CraniopharyngiomasMohammad Ali IsmailNo ratings yet
- Interview Hanson IpqDocument8 pagesInterview Hanson Ipqluizfelipenobresc5492No ratings yet
- INDEXES Real BooksDocument81 pagesINDEXES Real Booksluizfelipenobresc5492No ratings yet
- Sanderson Accu-Tuner: Operating ManualDocument28 pagesSanderson Accu-Tuner: Operating Manualluizfelipenobresc5492No ratings yet
- American Journal of Roentgenology 2017 MachadoDocument7 pagesAmerican Journal of Roentgenology 2017 Machadoluizfelipenobresc5492No ratings yet
- R.E.N.A.L. Nephrometry Scoring SystemDocument5 pagesR.E.N.A.L. Nephrometry Scoring Systemluizfelipenobresc5492No ratings yet
- Drum Set NotationDocument23 pagesDrum Set NotationMarcos MendesNo ratings yet
- Samsung Manual GT S5830Document128 pagesSamsung Manual GT S5830Luiz Felipe NobreNo ratings yet
- Recist GuidelineDocument20 pagesRecist Guidelineferas_oskan781No ratings yet
- uMEC Vet - Operator's Manual - V5.0 - ENDocument198 pagesuMEC Vet - Operator's Manual - V5.0 - ENJuanNo ratings yet
- iMEC Operators Manual PDFDocument354 pagesiMEC Operators Manual PDFVinsmoke SanjiNo ratings yet
- PM - IntelliVue MP2 Patient MonitorDocument30 pagesPM - IntelliVue MP2 Patient MonitorpilarNo ratings yet
- MCQ Internal Medicine PDFDocument448 pagesMCQ Internal Medicine PDFAyaa Yousef100% (5)
- OMI 2018, MirandaDocument14 pagesOMI 2018, MirandaResidentes UrgenciasNo ratings yet
- Anti-Infectives Drug Advisory Committee MeetingDocument253 pagesAnti-Infectives Drug Advisory Committee MeetingbellamajNo ratings yet
- ECG InterpretationDocument95 pagesECG InterpretationNur Rahmat Wibowo100% (9)
- Philips QT MeasurementDocument6 pagesPhilips QT MeasurementECG CarditekNo ratings yet
- Overview of Sudden Cardiac Arrest and Sudden Cardiac Death - UpToDateDocument23 pagesOverview of Sudden Cardiac Arrest and Sudden Cardiac Death - UpToDateSamuel MartinezNo ratings yet
- Invega SustennaDocument33 pagesInvega SustennammoslemNo ratings yet
- Emergency Medicine - The Principles of Practice, 6E (2014) (PDF) (UnitedVRG) PDFDocument1,155 pagesEmergency Medicine - The Principles of Practice, 6E (2014) (PDF) (UnitedVRG) PDFspadky100% (3)
- Chlorine Dioxide Prophylaxis for COVID19 SymptomsDocument10 pagesChlorine Dioxide Prophylaxis for COVID19 SymptomsShane AgresNo ratings yet
- Datasheet ePM CompactDocument3 pagesDatasheet ePM CompactAlexander Ramirez GarciaNo ratings yet
- Management Methamphetamine ToxicityDocument20 pagesManagement Methamphetamine Toxicitykitchen245No ratings yet
- Paediatric ECG ChecklistDocument2 pagesPaediatric ECG ChecklistMuhammad Moazzam GulzarNo ratings yet
- Rilpivirine Injection Dosing and AdministrationDocument74 pagesRilpivirine Injection Dosing and AdministrationCamelia AirineiNo ratings yet
- Antipsychotics Guide Nov-20Document22 pagesAntipsychotics Guide Nov-20luis.parerasNo ratings yet
- Electrocardiographic Monitoring 2017Document72 pagesElectrocardiographic Monitoring 2017Mirela Marina BlajNo ratings yet
- Sample Pages From Pocket Medicine PDFDocument13 pagesSample Pages From Pocket Medicine PDFjolurl25% (4)
- Corrected QT Interval and Corrected QT Dispersion in ObesityDocument4 pagesCorrected QT Interval and Corrected QT Dispersion in ObesityasclepiuspdfsNo ratings yet
- Vomina Syrup - Uses, Side-Effects, Reviews, and Precautions - TabletWise - IndonesiaDocument1 pageVomina Syrup - Uses, Side-Effects, Reviews, and Precautions - TabletWise - IndonesiaMey KhNo ratings yet
- H 046 005013 00 Passport 17m12m Ops Manual FDA 6.0Document464 pagesH 046 005013 00 Passport 17m12m Ops Manual FDA 6.0bprzNo ratings yet
- Intellivue Mp60/Mp70 Patient Monitor: Philips M8005A, M8007A Technical Data SheetDocument20 pagesIntellivue Mp60/Mp70 Patient Monitor: Philips M8005A, M8007A Technical Data SheetZain MonNo ratings yet
- Ele&Arr&Com&Rev&Das&Zip&1 STDocument492 pagesEle&Arr&Com&Rev&Das&Zip&1 STeuinpersoana100% (3)
- ECG Interpretation Program: User'S GuideDocument154 pagesECG Interpretation Program: User'S Guidemogahid jojoNo ratings yet
- Plasmodium Falciparum Malaria: A Multicentre, Open-Label,: ArticlesDocument16 pagesPlasmodium Falciparum Malaria: A Multicentre, Open-Label,: ArticlesmdNo ratings yet
- Article - ECG Vs MCGDocument7 pagesArticle - ECG Vs MCGpaul_calburean7899No ratings yet
- ECG Lectures 2023-2024Document29 pagesECG Lectures 2023-2024owronrawan74No ratings yet
- Serial Comparison Algorithm ReferenceDocument28 pagesSerial Comparison Algorithm ReferenceHoàng Anh NguyễnNo ratings yet
- Clinical ElectrocardiographyDocument134 pagesClinical ElectrocardiographyHossain MuhammadNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (16)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)