You might also like
- Berkey Colortran Lighting & Production Equipment Price List 8-1975Document20 pagesBerkey Colortran Lighting & Production Equipment Price List 8-1975Alan Masters100% (1)
- Rolls Royce Turbines Borescope and Guide Tube GuideDocument7 pagesRolls Royce Turbines Borescope and Guide Tube GuideSean O'ConnorNo ratings yet
- Bermad Air Valve Price List 2021 DN50-DN200Document1 pageBermad Air Valve Price List 2021 DN50-DN200wawanNo ratings yet
- Boost Your Quality Career & Organization's Bottom LineDocument12 pagesBoost Your Quality Career & Organization's Bottom LineRob WillestoneNo ratings yet
- Iso+9000 3 1997Document38 pagesIso+9000 3 1997api-19846338No ratings yet
- Modeling of The Evaporation and Condensation Phase Change Problems With FLUENTDocument17 pagesModeling of The Evaporation and Condensation Phase Change Problems With FLUENTRashed KaiserNo ratings yet
- Tariff, Power Factor and Power Factor ImprovementDocument12 pagesTariff, Power Factor and Power Factor ImprovementnurliyanaNo ratings yet
- Guideline For Grade and Compensation FitmentDocument5 pagesGuideline For Grade and Compensation FitmentVijit MisraNo ratings yet
- MECH448 Mid-Terms Samples 2013Document6 pagesMECH448 Mid-Terms Samples 2013Imam A. RamadhanNo ratings yet
- Astm 1020 PDFDocument3 pagesAstm 1020 PDFbarrancabermeja24No ratings yet
- Safety Shut-Off Valve RMG 720Document8 pagesSafety Shut-Off Valve RMG 720dianudin safarudinNo ratings yet
- Clickable MDocument1 pageClickable Mapi-240084111No ratings yet
- 3 81 e pv15 Pneumatic On Off Globe Valves dn15 100 enDocument6 pages3 81 e pv15 Pneumatic On Off Globe Valves dn15 100 enQuyết Bạch ĐìnhNo ratings yet
- BR PE Spigot Products Range 2017Document27 pagesBR PE Spigot Products Range 2017GerryNo ratings yet
- Data Stok Spare Part Mesin LaserDocument1 pageData Stok Spare Part Mesin LaserHafidz SaepudinNo ratings yet
- Outdoor unit specifications tableDocument2 pagesOutdoor unit specifications tableAhmed NajjarNo ratings yet
- CE Marking Lamistal - PDF 2Document1 pageCE Marking Lamistal - PDF 2SenidaBektašNo ratings yet
- Goetze 2781 Datasheet enDocument4 pagesGoetze 2781 Datasheet enrosiNo ratings yet
- Product Bulletin Fisher Rotary Valve Selection Guide en 135280Document16 pagesProduct Bulletin Fisher Rotary Valve Selection Guide en 135280Rachmat MaulanaNo ratings yet
- Butterfly Valves Certificate RenewalDocument4 pagesButterfly Valves Certificate RenewalIsa KumNo ratings yet
- Water Features - SP & SupplierDocument4 pagesWater Features - SP & SupplierMohammed SayeeduddinNo ratings yet
- Type Approval CertificateDocument4 pagesType Approval CertificateDerick LopesNo ratings yet
- Standard Schedule of Rates for 2020-2021Document333 pagesStandard Schedule of Rates for 2020-2021Ramesh BabuNo ratings yet
- Double Regulating Valve (DRV) - DZR Brass Body, Xpress Ends For Copper/Carbon Steel/Stainless Steel TubeDocument11 pagesDouble Regulating Valve (DRV) - DZR Brass Body, Xpress Ends For Copper/Carbon Steel/Stainless Steel TubeImtiyaz KhanNo ratings yet
- En 10219 PDFDocument2 pagesEn 10219 PDFVivekNo ratings yet
- Quote - P22576 - Cinnabon - Dubai Hills Mall-1Document1 pageQuote - P22576 - Cinnabon - Dubai Hills Mall-1Nikita SalunkheNo ratings yet
- Product Bulletin Fisher Rotary Valve Selection Guide en 135280Document16 pagesProduct Bulletin Fisher Rotary Valve Selection Guide en 135280Alberto GuillenNo ratings yet
- Catalogu AVK PDFDocument247 pagesCatalogu AVK PDFDana BaNo ratings yet
- Bronze Relief Valve DN10 DN15 DN20Document2 pagesBronze Relief Valve DN10 DN15 DN20billNo ratings yet
- CE Marking Laminado Extraclear 88Document1 pageCE Marking Laminado Extraclear 88Filipe SousaNo ratings yet
- CE Marking - PDF 1Document1 pageCE Marking - PDF 1SenidaBektašNo ratings yet
- Fisher Vee-Ball (V150, V200 & V300) (NPS 1 Through 12)Document52 pagesFisher Vee-Ball (V150, V200 & V300) (NPS 1 Through 12)Arianeth BalcazarNo ratings yet
- Dismantling Joint - AVKDocument2 pagesDismantling Joint - AVKtecnoturbines ttNo ratings yet
- DFS (GS 06p01y01-E-E - 008)Document30 pagesDFS (GS 06p01y01-E-E - 008)tetioNo ratings yet
- Product Bulletin Fisher Rotary Valve Selection Guide en 135280Document16 pagesProduct Bulletin Fisher Rotary Valve Selection Guide en 135280jairo moralesNo ratings yet
- Type 14din Ds Aug 18Document3 pagesType 14din Ds Aug 18Suresh KumarNo ratings yet
- 319499012 Inventory of Spare Parts February09Document1 page319499012 Inventory of Spare Parts February09kramergeorgec397No ratings yet
- Inspection ReportDocument1 pageInspection ReportvenkatNo ratings yet
- Type 13din Ds Jan18Document3 pagesType 13din Ds Jan18Suresh KumarNo ratings yet
- InformationDocument2 pagesInformationbiswasdipankar05No ratings yet
- OL50 Based Low Intensity Obstruction LightDocument2 pagesOL50 Based Low Intensity Obstruction LightCarlos Merckx OlarteNo ratings yet
- PXC - Alati - Flajer 2020Document2 pagesPXC - Alati - Flajer 2020mikcomiNo ratings yet
- Lab IV Exp 10Document4 pagesLab IV Exp 10Moontarij JahanNo ratings yet
- Type 12din Ds Jan18Document3 pagesType 12din Ds Jan18Suresh KumarNo ratings yet
- Flange Adaptor PN 16Document1 pageFlange Adaptor PN 16Agung YudistiraNo ratings yet
- 03 Jul 201511 Jun 2014fiana162779Document6 pages03 Jul 201511 Jun 2014fiana162779Saumya ShrivastavaNo ratings yet
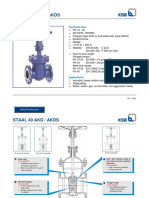
- Staal 40 Akd / Akds: Technical DataDocument6 pagesStaal 40 Akd / Akds: Technical Dataedark2009No ratings yet
- Application For Witness Inspection: Ly Hong Huan Hong River Surface Water Treatment Plant ProjectDocument2 pagesApplication For Witness Inspection: Ly Hong Huan Hong River Surface Water Treatment Plant ProjectPhu PhuocNo ratings yet
- Skolan CatalogDocument14 pagesSkolan CataloguaeradsNo ratings yet
- VZAV 202303 enDocument32 pagesVZAV 202303 enMafe CastilloNo ratings yet
- Ball Bearing Nom PDFDocument1 pageBall Bearing Nom PDFramanshriNo ratings yet
- b15 Electra B Dock Set 25250 25252 Catalogue Sheet 03 19Document4 pagesb15 Electra B Dock Set 25250 25252 Catalogue Sheet 03 19Igor GazdekNo ratings yet
- Vision Tester: Accurate Measurement With Simple and Comfortable OperationDocument2 pagesVision Tester: Accurate Measurement With Simple and Comfortable OperationFERNEY REYES MONSALVE0% (1)
- Catalog - CV. Berkat AnugerahDocument12 pagesCatalog - CV. Berkat AnugerahAshish GoelNo ratings yet
- GVAR360 HTFF354AS Service ManualDocument21 pagesGVAR360 HTFF354AS Service ManualUEENo ratings yet
- Avk Gate Valve PN 10 or PN 16 06/30 - 26/00Document2 pagesAvk Gate Valve PN 10 or PN 16 06/30 - 26/00Popescu OctavianNo ratings yet
- JRVSG CatalogDocument17 pagesJRVSG Cataloghan kimNo ratings yet
- HTFF525AS HTFF525AW Service ManualDocument22 pagesHTFF525AS HTFF525AW Service ManualUEE100% (1)
- DW12G SSDocument1 pageDW12G SSQuyết Bạch ĐìnhNo ratings yet
- Circular Sightglas e Malux Din28121Document2 pagesCircular Sightglas e Malux Din28121ivanoliveira3261No ratings yet
- Valvulas Saturno 2011 PDFDocument2 pagesValvulas Saturno 2011 PDFJose Ignacio Ancalaf RainNo ratings yet
- Deublin Main CatalogueDocument60 pagesDeublin Main CatalogueAlTakamol coNo ratings yet
- Europa Check and Foot Valves: Technical CatalogueDocument16 pagesEuropa Check and Foot Valves: Technical CatalogueDomagoj ButumovićNo ratings yet
- Butterfly Valve DesponiaDocument8 pagesButterfly Valve Desponiadk_moehammedNo ratings yet
- Type 9 Ds Jan18Document3 pagesType 9 Ds Jan18Suresh KumarNo ratings yet
- Project: Engineering, Procurement & Construction For Upgrade Uthmaniyah-Abqaiq Pipelines Systems Bi# 10-01196 CONTRACT# 6600049184Document1 pageProject: Engineering, Procurement & Construction For Upgrade Uthmaniyah-Abqaiq Pipelines Systems Bi# 10-01196 CONTRACT# 6600049184Mohamed Wasim ShaikhNo ratings yet
- Understanding Lightning and Lightning Protection: A Multimedia Teaching GuideFrom EverandUnderstanding Lightning and Lightning Protection: A Multimedia Teaching GuideNo ratings yet
- Electronic Funds Transfer (Eft) Authorization Agreement: Page 1 of 3Document3 pagesElectronic Funds Transfer (Eft) Authorization Agreement: Page 1 of 3JayNo ratings yet
- Patient Encounter Form: Facility Number: Facility Name: Facility Address: NPI NumberDocument2 pagesPatient Encounter Form: Facility Number: Facility Name: Facility Address: NPI NumberJayNo ratings yet
- Address Change FormDocument2 pagesAddress Change FormJayNo ratings yet
- DDIN Individual Preventive Plan - Sample CombinedDocument16 pagesDDIN Individual Preventive Plan - Sample CombinedJayNo ratings yet
- Contoh 1 Application Letter CV Bahasa InggrisDocument6 pagesContoh 1 Application Letter CV Bahasa InggrisUlya QonitaNo ratings yet
- CableConduits InterflexDocument132 pagesCableConduits InterflexSEO BDMNo ratings yet
- PMT Hps 34 VF 03 23 Mag3000 SpecificationsDocument17 pagesPMT Hps 34 VF 03 23 Mag3000 Specificationswika mepNo ratings yet
- SMA and Sofar Inverter PricelistDocument3 pagesSMA and Sofar Inverter PricelistYuvaraj JeyachandranNo ratings yet
- Electrode Kinetics and Polarization PhenomenonDocument3 pagesElectrode Kinetics and Polarization PhenomenonbhanuNo ratings yet
- Knowledge Test For The Understanding of Load Chart For Crane Operators and Lifting SupervisorsDocument2 pagesKnowledge Test For The Understanding of Load Chart For Crane Operators and Lifting SupervisorsMohd FadliNo ratings yet
- Introduction To The Project and Overview of Power System SecurityDocument9 pagesIntroduction To The Project and Overview of Power System Securitysalagasim100% (1)
- Microsoft Powerpoint 2013 Tutorial Student Technology Assistant CenterDocument12 pagesMicrosoft Powerpoint 2013 Tutorial Student Technology Assistant CenterBosko LjubisavljevicNo ratings yet
- Manual-Humdinger Concrete Vibrator 20151126 UKDocument20 pagesManual-Humdinger Concrete Vibrator 20151126 UKValentin NiculaeNo ratings yet
- DR Reporting Made Easy With Report Builder 3.0Document132 pagesDR Reporting Made Easy With Report Builder 3.0robertorojasfeijoNo ratings yet
- GeoTextiles PDFDocument6 pagesGeoTextiles PDFAsım DavulcuNo ratings yet
- Arcor - enDocument2 pagesArcor - enIker MelladoNo ratings yet
- Analysis Based On 15-16 SORDocument195 pagesAnalysis Based On 15-16 SORAjay SaikumarNo ratings yet
- Off Grid PV Systems Design GuidelinesDocument24 pagesOff Grid PV Systems Design GuidelinestantibaNo ratings yet
- Rolls ModelsDocument186 pagesRolls ModelsapeirotanNo ratings yet
- 2015 Ordinance BTech DtuDocument32 pages2015 Ordinance BTech DtuGaganpreetSinghNo ratings yet
- MB09807UDocument27 pagesMB09807URavishka SilvaNo ratings yet
- (BS 5955-8-2001) - Plastics Pipework (Thermoplastics Materials) - Specification For The Installation of Thermoplastic Pipes and Associated Fittings For Use in Domestic HoDocument14 pages(BS 5955-8-2001) - Plastics Pipework (Thermoplastics Materials) - Specification For The Installation of Thermoplastic Pipes and Associated Fittings For Use in Domestic HojohnNo ratings yet
- SJ-20100510160815-008-ZXSDR BTS&Node B (V4.09.21) Performance Counter Reference - 325875Document413 pagesSJ-20100510160815-008-ZXSDR BTS&Node B (V4.09.21) Performance Counter Reference - 325875sndi1765100% (1)
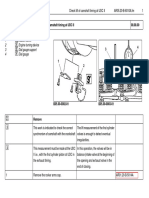
- AR05.20-B-6010A.fm Check Lift of Camshaft Timing at UDC II 08.08.00Document4 pagesAR05.20-B-6010A.fm Check Lift of Camshaft Timing at UDC II 08.08.00LUKASNo ratings yet
- 2014 Summer Model Answer PaperDocument20 pages2014 Summer Model Answer Papercivil gpkpNo ratings yet
- 1978 Fairchild TTL Data Book PDFDocument752 pages1978 Fairchild TTL Data Book PDFNiraj KapaseNo ratings yet
- Typical Cable Laying Details For Direct Buried, Low Tension CablesDocument6 pagesTypical Cable Laying Details For Direct Buried, Low Tension CablesAbdul Muneer PalapraNo ratings yet