You might also like
- Water Culture in South Asia: Bangladesh Perspectives: Bangladesh perspectivesFrom EverandWater Culture in South Asia: Bangladesh Perspectives: Bangladesh perspectivesNo ratings yet
- Water, Sanitation and Hygiene PracticesDocument5 pagesWater, Sanitation and Hygiene PracticesHaziq Irfan KamalludinNo ratings yet
- Emerging Science for Sustainable Water Resources Management: a Guide for Water Professionals and Practitioners in IndiaFrom EverandEmerging Science for Sustainable Water Resources Management: a Guide for Water Professionals and Practitioners in IndiaNo ratings yet
- Jurnal BionursingDocument6 pagesJurnal Bionursingdiana pefbriantiNo ratings yet
- Research PaperDocument12 pagesResearch PapershreyanshNo ratings yet
- Dea 1Document11 pagesDea 1Dea Hadfina Kartika SariNo ratings yet
- A Study On Knowledge and Practice of Hand WashingDocument6 pagesA Study On Knowledge and Practice of Hand WashingDini GintingNo ratings yet
- Evaluation of WASH Indicators Associated With DiarDocument16 pagesEvaluation of WASH Indicators Associated With DiarAmardeep VishwakarmaNo ratings yet
- 2183 8675 5 PBDocument7 pages2183 8675 5 PBnadhira rashifantiNo ratings yet
- Assessment of Existing Domestic Water Sanitation Practices in Adilabad DistrictDocument10 pagesAssessment of Existing Domestic Water Sanitation Practices in Adilabad DistrictTJPRC PublicationsNo ratings yet
- Association Between Environmental Factors and Incidence of Diarrhea Among Toddlers in The Working Area of Ambal I Health Center, Kebumen, Center of Java, IndonesiaDocument9 pagesAssociation Between Environmental Factors and Incidence of Diarrhea Among Toddlers in The Working Area of Ambal I Health Center, Kebumen, Center of Java, IndonesiaIJELS Research JournalNo ratings yet
- Kejadian DiareDocument5 pagesKejadian DiareDesi AdestiNo ratings yet
- WASHARTICLEDocument4 pagesWASHARTICLEFomukwin Ayenui NoelNo ratings yet
- Food Quality SurveyDocument5 pagesFood Quality SurveyPrashant TripathiNo ratings yet
- Jurnal GeodesiDocument10 pagesJurnal GeodesiYusuf Hary SaputroNo ratings yet
- Hygiene and Sanitation Practices of Mothers and Prevalence of Diarrhea Among  2 Years of Children in A Resettlement ColonyDocument5 pagesHygiene and Sanitation Practices of Mothers and Prevalence of Diarrhea Among  2 Years of Children in A Resettlement ColonyIJAR JOURNALNo ratings yet
- Water WaterDocument18 pagesWater WaterWilliams ADEWOLENo ratings yet
- Prevalence of Acute Diarrheal Diseases and Associated Risk Factors Among Under Five Children in An Urban Slum of MumbaiDocument5 pagesPrevalence of Acute Diarrheal Diseases and Associated Risk Factors Among Under Five Children in An Urban Slum of MumbaiIJAR JOURNALNo ratings yet
- JakartaDocument7 pagesJakartaBachtiar M TaUfikNo ratings yet
- Solar Disinfection of Water For Diarrhoeal Prevention in Southern IndiaDocument4 pagesSolar Disinfection of Water For Diarrhoeal Prevention in Southern IndiaFelipe MNo ratings yet
- Food and Personal Hygiene Perceptions and PracticesDocument8 pagesFood and Personal Hygiene Perceptions and PracticesFa MoNo ratings yet
- Pi Is 1876034117301363Document6 pagesPi Is 1876034117301363ardytawaradaniNo ratings yet
- Journal MesinaDocument4 pagesJournal MesinaKrizelle MesinaNo ratings yet
- Review of Related LiteratureDocument7 pagesReview of Related Literaturemark3dasaNo ratings yet
- Hartini, Didik Gunawan Tamtomo, Nunuk Suryani: PendahuluanDocument9 pagesHartini, Didik Gunawan Tamtomo, Nunuk Suryani: PendahuluanGugelNo ratings yet
- Jurnal Kesehatan: Kebiasaan Buang Air Besar Sembarangan (BABS) Di Desa Tanjung Peranap, Tebing Tinggi BaratDocument9 pagesJurnal Kesehatan: Kebiasaan Buang Air Besar Sembarangan (BABS) Di Desa Tanjung Peranap, Tebing Tinggi BaratRidho MahendraNo ratings yet
- Reducing The User Burden in WASH Interventions ForDocument2 pagesReducing The User Burden in WASH Interventions ForRAHUL SHINDENo ratings yet
- HandHygiene PDFDocument5 pagesHandHygiene PDFDrBishnu Prasad MahalaNo ratings yet
- Maternal Knowledge, Attitudes and Practices Towards Prevention and Management of Child Diarrhoea in Urban and Rural Maseru, LesothoDocument20 pagesMaternal Knowledge, Attitudes and Practices Towards Prevention and Management of Child Diarrhoea in Urban and Rural Maseru, LesothoAnisa SafutriNo ratings yet
- A Study To Assess The Knowledge of The Utility of Toilets and Hazards of Open Air Defecation Practice Among Rural Adults of Muchakandi VillageDocument6 pagesA Study To Assess The Knowledge of The Utility of Toilets and Hazards of Open Air Defecation Practice Among Rural Adults of Muchakandi VillageInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 10 Z - Menik 2019 PDFDocument8 pages10 Z - Menik 2019 PDFAriF mauLNo ratings yet
- 3 Sop - Is TPMMDocument10 pages3 Sop - Is TPMMcahyo setiawanNo ratings yet
- Perception of Parents On Childhood Diarrhoea and IDocument5 pagesPerception of Parents On Childhood Diarrhoea and IAnisa SafutriNo ratings yet
- 1 s2.0 S2213398422000392 MainDocument9 pages1 s2.0 S2213398422000392 MainMoad RuzkiNo ratings yet
- Environmental Factors Associated With Acute Diarrhea Among Children Under Five Years of Age in Derashe District, Southern EthiopiaDocument10 pagesEnvironmental Factors Associated With Acute Diarrhea Among Children Under Five Years of Age in Derashe District, Southern Ethiopiadefitri sariningtyasNo ratings yet
- Public KnowledgeDocument7 pagesPublic KnowledgeSaad aliraqiNo ratings yet
- University of Santo Tomas College of NursingDocument11 pagesUniversity of Santo Tomas College of NursingFlorenze ArtNo ratings yet
- Article1381156255 - Juneja and ChaudharyDocument6 pagesArticle1381156255 - Juneja and ChaudharyWijetunga SomasiriNo ratings yet
- Upaya Penurunan Kasus Diare Dengan Meningkatkan Keterlibatan Ibu Dalam Gerakan PHBSDocument8 pagesUpaya Penurunan Kasus Diare Dengan Meningkatkan Keterlibatan Ibu Dalam Gerakan PHBSNidia Achirul tamaraNo ratings yet
- Pietzsch 1884Document5 pagesPietzsch 1884minjunk728No ratings yet
- Journal Homepage: - : 61 YearsDocument11 pagesJournal Homepage: - : 61 YearsIJAR JOURNALNo ratings yet
- Clinical Epidemiology and Global HealthDocument4 pagesClinical Epidemiology and Global HealthIndira SellyNo ratings yet
- Research Article Food and Personal Hygiene Perceptions and Practices Among Caregivers Whose Children Have Diarrhea: A Qualitative Study of Urban Mothers in Tangerang, IndonesiaDocument8 pagesResearch Article Food and Personal Hygiene Perceptions and Practices Among Caregivers Whose Children Have Diarrhea: A Qualitative Study of Urban Mothers in Tangerang, IndonesiaAndi UmmahNo ratings yet
- Tugas Bhs Inggris - Temu 2 - KLPMK 4 - A12-BDocument9 pagesTugas Bhs Inggris - Temu 2 - KLPMK 4 - A12-BWisnu 12No ratings yet
- Gambaran Riwayat Kejadian Diare Pada Balita Dan Pelaksanaan PHBS Dalam Tatanan Rumah Tangga Di Desa Gegelang Kecamatan Manggis Tahun 2013Document9 pagesGambaran Riwayat Kejadian Diare Pada Balita Dan Pelaksanaan PHBS Dalam Tatanan Rumah Tangga Di Desa Gegelang Kecamatan Manggis Tahun 2013lisaNo ratings yet
- Chu 2019Document6 pagesChu 2019Edgar Uriel Rodriguez MuñozNo ratings yet
- Faktor Pengaruh Terhadap Ketersediaan Septictank Dan Sambungan Sewerage System Permukiman Pinggiran Kali, Kel. Dangin Puri, DenpasarDocument8 pagesFaktor Pengaruh Terhadap Ketersediaan Septictank Dan Sambungan Sewerage System Permukiman Pinggiran Kali, Kel. Dangin Puri, DenpasarSinta NorhayatiNo ratings yet
- 92mengesha AdmassuDocument10 pages92mengesha AdmassuHusnullah PangeranNo ratings yet
- Manuskrip Pengmas Penyuluhan Stunting Kelompok 2Document26 pagesManuskrip Pengmas Penyuluhan Stunting Kelompok 2halidaNo ratings yet
- Health Status and Quality of Life of Geriatric Population in Old Age Homes and Living With Family in Chennai A Comparative StudyDocument5 pagesHealth Status and Quality of Life of Geriatric Population in Old Age Homes and Living With Family in Chennai A Comparative StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Evaluation of The Impact of The Plastic Biosand Filter On Health and Drinking Water Quality in Rural Tamale, GhanaDocument18 pagesEvaluation of The Impact of The Plastic Biosand Filter On Health and Drinking Water Quality in Rural Tamale, GhanaYusuf Niko FitrantoNo ratings yet
- Effects of A Participatory Agriculture and Nutrition EducationsDocument7 pagesEffects of A Participatory Agriculture and Nutrition EducationswaitNo ratings yet
- Knowledge, Attitude, and Practices of Community People Regarding Typhoid FeverDocument5 pagesKnowledge, Attitude, and Practices of Community People Regarding Typhoid FeverEddna SeharNo ratings yet
- Article SssssssssssssssssssDocument7 pagesArticle SssssssssssssssssssBULAN IFTINAZHIFANo ratings yet
- Risk Correlates of Diarrhea in Children Under 5 Years of Age in Slums of Bankura, West BengalDocument8 pagesRisk Correlates of Diarrhea in Children Under 5 Years of Age in Slums of Bankura, West BengalSanaNo ratings yet
- WASH (Water, Sanitation and Hygiene) : August 2018Document6 pagesWASH (Water, Sanitation and Hygiene) : August 2018Zakia RafiqNo ratings yet
- Acute Malnutrition PDFDocument10 pagesAcute Malnutrition PDFDamesa MiesaNo ratings yet
- Correlates of Household Food Insecurity and Low Dietary Diversity in Rural CambodiaDocument11 pagesCorrelates of Household Food Insecurity and Low Dietary Diversity in Rural CambodiaKomang TriwiramaNo ratings yet
- Effect of Household Life Behavior To Clean and Healthy Life in District Marabahan, Barito KualaDocument5 pagesEffect of Household Life Behavior To Clean and Healthy Life in District Marabahan, Barito KualaGalihNo ratings yet
- 8 Asep 2018Document6 pages8 Asep 2018AriF mauLNo ratings yet
- Iot-Based Compact-Matic Drinking Water Filtration Machine: August 2020Document7 pagesIot-Based Compact-Matic Drinking Water Filtration Machine: August 2020Sou TVNo ratings yet
- NSF Standard 14Document14 pagesNSF Standard 14osamihNo ratings yet
- Automatic Drinking Water Saving System For Municipal Water ProjectsDocument46 pagesAutomatic Drinking Water Saving System For Municipal Water ProjectsShanmugam Ramasamy0% (2)
- Pyanosid - Powder 3753 K 0317 Engl - 01Document5 pagesPyanosid - Powder 3753 K 0317 Engl - 01Ionuţ BuţurcăNo ratings yet
- 1.aqua CentreDocument7 pages1.aqua CentreYoga ArchNo ratings yet
- University of Zimbabwe Faculty of Engineering Department of Civil EngineeringDocument19 pagesUniversity of Zimbabwe Faculty of Engineering Department of Civil EngineeringRyeanKRumanoNo ratings yet
- Full Lab Report 5Document12 pagesFull Lab Report 5Siti SyuhadahNo ratings yet
- NSS 76 Ins Ch1Document41 pagesNSS 76 Ins Ch1Shoibal ChakravartyNo ratings yet
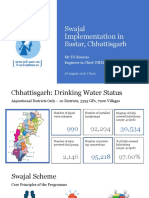
- Chattisgarh - PHED - Presentation On Swajal PilotDocument17 pagesChattisgarh - PHED - Presentation On Swajal PilotAksdgr8No ratings yet
- 1 - Introduction - Water Sypply System NewDocument8 pages1 - Introduction - Water Sypply System NewHappyKumarLadherNo ratings yet
- 1 7 AwhatisitDocument6 pages1 7 Awhatisitapi-264814535100% (1)
- WATER TESTING LABORATORY LAW FinalDocument4 pagesWATER TESTING LABORATORY LAW Finalanon_183657266No ratings yet
- AMERICAN RED CROSS 2006 Project Design and ProposalDocument55 pagesAMERICAN RED CROSS 2006 Project Design and ProposalAleksandar BogdanovicNo ratings yet
- Sustainable Water Resource Management - The Singapore ExperienceDocument81 pagesSustainable Water Resource Management - The Singapore ExperienceObserver Research Foundation (ORF), Mumbai100% (2)
- Caps Final Na Gyud Ni Nga Edit10000Document59 pagesCaps Final Na Gyud Ni Nga Edit10000Christian SanohNo ratings yet
- End-Year 2008 ReportDocument255 pagesEnd-Year 2008 ReportVichetrNo ratings yet
- Water and Sanitation Thesis TopicsDocument7 pagesWater and Sanitation Thesis Topicsshannongutierrezcorpuschristi100% (2)
- Charmaine V. Rosales: Related LiteraturesDocument6 pagesCharmaine V. Rosales: Related LiteraturesCharmaine RosalesNo ratings yet
- MPCA Response 5.29.20Document2 pagesMPCA Response 5.29.20Duluth News TribuneNo ratings yet
- PSTAdec 2017Document586 pagesPSTAdec 2017Ryan Bacarro BagayanNo ratings yet
- Pacp Macp OverviewDocument40 pagesPacp Macp Overviewjoescribd55No ratings yet
- Global Cholera Epidemiology: Opportunities To Reduce The Burden of Cholera by 2030Document4 pagesGlobal Cholera Epidemiology: Opportunities To Reduce The Burden of Cholera by 2030Gufron MustofaNo ratings yet
- Letter From Harvard Leaders To EPA's Andrew Wheeler On Proposed Science PolicyDocument60 pagesLetter From Harvard Leaders To EPA's Andrew Wheeler On Proposed Science PolicyEmily AtkinNo ratings yet
- Entrepreneurial Cognition: Exploring The Mindset of EntrepreneursDocument288 pagesEntrepreneurial Cognition: Exploring The Mindset of EntrepreneursErica_100% (1)
- Building Utilities 1 - Plumbing and Sanitary Systems QUIZ NO.: MT-QZ-01 Quiz E-File No.: Arbu1Qz01 - Dayso, AbrenDocument5 pagesBuilding Utilities 1 - Plumbing and Sanitary Systems QUIZ NO.: MT-QZ-01 Quiz E-File No.: Arbu1Qz01 - Dayso, AbrenAbren DaysoNo ratings yet
- Cholera Outbreak Guidelines: Preparedness, Prevention and ControlDocument105 pagesCholera Outbreak Guidelines: Preparedness, Prevention and ControlOxfam100% (1)
- Sanitation & Fumigation - Inspection - AnswersDocument2 pagesSanitation & Fumigation - Inspection - AnswersKirtishbose ChowdhuryNo ratings yet
- Water Management: For Urban and Peri-Urban HorticultureDocument4 pagesWater Management: For Urban and Peri-Urban HorticulturegiabrunNo ratings yet
- Superswell 47B BrochureDocument4 pagesSuperswell 47B BrochureYang W OngNo ratings yet
- Environmental Destruction in Ethiopia:A Leading Factor in Oromo MigrationFinalDocument21 pagesEnvironmental Destruction in Ethiopia:A Leading Factor in Oromo MigrationFinaloromopressNo ratings yet
- The Cyanide Canary: A True Story of InjusticeFrom EverandThe Cyanide Canary: A True Story of InjusticeRating: 4 out of 5 stars4/5 (51)
- Slow Violence and the Environmentalism of the PoorFrom EverandSlow Violence and the Environmentalism of the PoorRating: 4 out of 5 stars4/5 (5)
- The Rights of Nature: A Legal Revolution That Could Save the WorldFrom EverandThe Rights of Nature: A Legal Revolution That Could Save the WorldRating: 5 out of 5 stars5/5 (1)
- Waste: One Woman’s Fight Against America’s Dirty SecretFrom EverandWaste: One Woman’s Fight Against America’s Dirty SecretRating: 5 out of 5 stars5/5 (1)
- Art of Commenting: How to Influence Environmental Decisionmaking With Effective Comments, The, 2d EditionFrom EverandArt of Commenting: How to Influence Environmental Decisionmaking With Effective Comments, The, 2d EditionRating: 3 out of 5 stars3/5 (1)
- 3rd Grade Science: Life Sciences in Eco Systems | Textbook EditionFrom Everand3rd Grade Science: Life Sciences in Eco Systems | Textbook EditionNo ratings yet
- Desperate: An Epic Battle for Clean Water and Justice in AppalachiaFrom EverandDesperate: An Epic Battle for Clean Water and Justice in AppalachiaRating: 4 out of 5 stars4/5 (1)
- Environmental Education in Practice: Concepts and ApplicationsFrom EverandEnvironmental Education in Practice: Concepts and ApplicationsNo ratings yet
- Exposure: Poisoned Water, Corporate Greed, and One Lawyer's Twenty-Year Battle Against DuPontFrom EverandExposure: Poisoned Water, Corporate Greed, and One Lawyer's Twenty-Year Battle Against DuPontRating: 4.5 out of 5 stars4.5/5 (18)
- Busted!: Drug War Survival Skills and True Dope DFrom EverandBusted!: Drug War Survival Skills and True Dope DRating: 3.5 out of 5 stars3.5/5 (7)
- Exposure: Poisoned Water, Corporate Greed, and One Lawyer's Twenty-Year Battle against DuPontFrom EverandExposure: Poisoned Water, Corporate Greed, and One Lawyer's Twenty-Year Battle against DuPontRating: 4.5 out of 5 stars4.5/5 (9)
- The Intersection of Intellectual Property Law and the “Green” Movement: RIPL’s Green Issue 2010From EverandThe Intersection of Intellectual Property Law and the “Green” Movement: RIPL’s Green Issue 2010Rating: 5 out of 5 stars5/5 (2)
- Down to the Wire: Confronting Climate CollapseFrom EverandDown to the Wire: Confronting Climate CollapseRating: 4.5 out of 5 stars4.5/5 (8)
- Reduce, Reuse and Recycle : The Secret to Environmental Sustainability : Environment Textbooks | Children's Environment BooksFrom EverandReduce, Reuse and Recycle : The Secret to Environmental Sustainability : Environment Textbooks | Children's Environment BooksNo ratings yet
- Fighting Westway: Environmental Law, Citizen Activism, and the Regulatory War That Transformed New York CityFrom EverandFighting Westway: Environmental Law, Citizen Activism, and the Regulatory War That Transformed New York CityNo ratings yet
- Land Divided by Law: The Yakama Indian Nation as Environmental History, 1840-1933From EverandLand Divided by Law: The Yakama Indian Nation as Environmental History, 1840-1933No ratings yet
- New Paradigms in Environmental Biomonitoring Using PlantsFrom EverandNew Paradigms in Environmental Biomonitoring Using PlantsSupriya TiwariNo ratings yet
- Dawn at Mineral King Valley: The Sierra Club, the Disney Company, and the Rise of Environmental LawFrom EverandDawn at Mineral King Valley: The Sierra Club, the Disney Company, and the Rise of Environmental LawRating: 4 out of 5 stars4/5 (334)
- Ecosystem Facts That You Should Know - The Forests Edition - Nature Picture Books | Children's Nature BooksFrom EverandEcosystem Facts That You Should Know - The Forests Edition - Nature Picture Books | Children's Nature BooksNo ratings yet