You might also like
- Definitions of MmpiDocument11 pagesDefinitions of MmpiBook ReaderNo ratings yet
- Educational Supervision in Social Work: A Task-Centered Model for Field Instruction and Staff DevelopmentFrom EverandEducational Supervision in Social Work: A Task-Centered Model for Field Instruction and Staff DevelopmentNo ratings yet
- Annual Review of Addictions and Offender Counseling: Best PracticesFrom EverandAnnual Review of Addictions and Offender Counseling: Best PracticesNo ratings yet
- Home Environment and Early Cognitive Development: Longitudinal ResearchFrom EverandHome Environment and Early Cognitive Development: Longitudinal ResearchAllen W. GottfriedNo ratings yet
- What You Need to Know When Your Child Is Admitted to a Psychiatric FacilityFrom EverandWhat You Need to Know When Your Child Is Admitted to a Psychiatric FacilityNo ratings yet
- The Therapist's Starter Guide: Setting Up and Building Your Practice, Working with Clients, and Managing Professional GrowthFrom EverandThe Therapist's Starter Guide: Setting Up and Building Your Practice, Working with Clients, and Managing Professional GrowthNo ratings yet
- ASWB EXAMINATION IN SOCIAL WORK [ASWB] (1 VOL.): Passbooks Study GuideFrom EverandASWB EXAMINATION IN SOCIAL WORK [ASWB] (1 VOL.): Passbooks Study GuideNo ratings yet
- DSM distributed system management Complete Self-Assessment GuideFrom EverandDSM distributed system management Complete Self-Assessment GuideNo ratings yet
- GROW: Someone I Loved Died: A Child's Workbook About Loss and GrievingFrom EverandGROW: Someone I Loved Died: A Child's Workbook About Loss and GrievingRating: 5 out of 5 stars5/5 (1)
- Final Group Counseling Project - Stress ManagementDocument82 pagesFinal Group Counseling Project - Stress Managementapi-548101945No ratings yet
- Malingering On The Personality Assessment Inventory: Identification of Specific Feigned DisordersDocument7 pagesMalingering On The Personality Assessment Inventory: Identification of Specific Feigned DisordersMissDSKNo ratings yet
- Causes and Risk Factors For Attention-Deficit Hyperactivity DisorderDocument8 pagesCauses and Risk Factors For Attention-Deficit Hyperactivity DisorderFranthesa LayloNo ratings yet
- Encouraging TeenagersDocument17 pagesEncouraging TeenagersTahNo ratings yet
- Millon Clinical IntroductionDocument27 pagesMillon Clinical IntroductionPratyush PrateekNo ratings yet
- Youngmee Kim - Gender in Psycho-Oncology (2018, Oxford University Press, USA)Document263 pagesYoungmee Kim - Gender in Psycho-Oncology (2018, Oxford University Press, USA)Dian Oktaria SafitriNo ratings yet
- C-SSRS Factsheet PDFDocument2 pagesC-SSRS Factsheet PDFAlejandroNo ratings yet
- The Mechanisms of Postpartum DepressionDocument70 pagesThe Mechanisms of Postpartum Depressionazniahsyam8269No ratings yet
- PSYCHIATRIC DISORDERS OF CHILDHOOD (Autosaved)Document43 pagesPSYCHIATRIC DISORDERS OF CHILDHOOD (Autosaved)Amy Lalringhluani Chhakchhuak100% (1)
- Adhd - Asrs .ScreenDocument4 pagesAdhd - Asrs .ScreenKenth GenobisNo ratings yet
- BDI ScaleDocument3 pagesBDI ScaleDeborah Bravian TairasNo ratings yet
- Case Analysis Case Study HelgaDocument10 pagesCase Analysis Case Study Helgaapi-487413988No ratings yet
- Personality Disorders PDFDocument35 pagesPersonality Disorders PDFABHINAVNo ratings yet
- Transformational assertiveness: how to stand up for yourselfDocument13 pagesTransformational assertiveness: how to stand up for yourselfPanchali_rNo ratings yet
- SdsadaDocument9 pagesSdsadaAnonymous KrfJpXb4iNNo ratings yet
- Rapid Screening for Adult ADHDDocument3 pagesRapid Screening for Adult ADHDPanduRespatiNo ratings yet
- Demographic and psychological assessment reportDocument3 pagesDemographic and psychological assessment reportmobeenNo ratings yet
- Trans-Affirming Therapist List - 8Document8 pagesTrans-Affirming Therapist List - 8api-250491080No ratings yet
- Introvert vs Extrovert Word Counts per DayDocument4 pagesIntrovert vs Extrovert Word Counts per Dayjisoo kimNo ratings yet
- Age 16 Child Behavior Checklist External Site MM FinalDocument6 pagesAge 16 Child Behavior Checklist External Site MM FinalSammy FilipeNo ratings yet
- Simple Thought Record WorksheetDocument2 pagesSimple Thought Record WorksheetEvaggelia ChroniNo ratings yet
- Y Bocs Information SampleDocument2 pagesY Bocs Information SampledevNo ratings yet
- The Unstructured Clinical InterviewDocument8 pagesThe Unstructured Clinical Interviewkasmiantoabadi100% (1)
- Theories of SuicideDocument43 pagesTheories of Suicidekrishnaa sistlaNo ratings yet
- 16PF BibDocument10 pages16PF BibdocagunsNo ratings yet
- Clinical Assessment InterviewDocument3 pagesClinical Assessment InterviewJena CalalangNo ratings yet
- Acceptance and Completion of Treatment Among Sex OffendersDocument17 pagesAcceptance and Completion of Treatment Among Sex OffenderspoopmanNo ratings yet
- Pages From FX207-0k2-Essentials of MCMI-IV Assessmen - Seth D. Grossman-2Document1 pagePages From FX207-0k2-Essentials of MCMI-IV Assessmen - Seth D. Grossman-2Kaisar OnoNo ratings yet
- Week 8 - Biopsychological Basis of Emotion, Aggression, and StressDocument17 pagesWeek 8 - Biopsychological Basis of Emotion, Aggression, and StressbbpcheeseNo ratings yet
- Adapting CBT For Children With An Autism Spectrum Disorder (ASD)Document3 pagesAdapting CBT For Children With An Autism Spectrum Disorder (ASD)Ina HasimNo ratings yet
- Guidelines for Interviewing ChildrenDocument9 pagesGuidelines for Interviewing Childrenaimara_viNo ratings yet
- Summary Sheet R-PAS Admin and ClarificationDocument2 pagesSummary Sheet R-PAS Admin and ClarificationMarina SwansonNo ratings yet
- DSM-5 and Culture - The Need To Move Towards A Shared Model of Care Within A More Equal Patient-Physician PartnershipDocument3 pagesDSM-5 and Culture - The Need To Move Towards A Shared Model of Care Within A More Equal Patient-Physician PartnershipPearl SkyNo ratings yet
- Gender Differences in Narcissism - A Meta-Analytic ReviewDocument52 pagesGender Differences in Narcissism - A Meta-Analytic ReviewBobi BadarevskiNo ratings yet
- Rehabilitation Psychology ChapterDocument48 pagesRehabilitation Psychology Chapterprince razzoukNo ratings yet
- Assessment and Behavioral Treatment of Selective MutismDocument22 pagesAssessment and Behavioral Treatment of Selective MutismAdriana ChertiNo ratings yet
- Violent Behaviour Assessment ScaleDocument2 pagesViolent Behaviour Assessment Scalejessicali717No ratings yet
- 2 MMPI-2 Validity-Scales Final PDFDocument9 pages2 MMPI-2 Validity-Scales Final PDFHanifa Bi BaritoNo ratings yet
- Vulnerablility CycleDocument21 pagesVulnerablility CycleVinicius SiqueiraNo ratings yet
- 1983 - The Brief Symptom Inventory, An Introductory ReportDocument11 pages1983 - The Brief Symptom Inventory, An Introductory ReportBogdan BaceanuNo ratings yet
- Trauma Checklist (PCL-C)Document4 pagesTrauma Checklist (PCL-C)Mayzie MayNo ratings yet
- Scoring The Strengths & Difficulties Questionnaire: For Age 4-17Document3 pagesScoring The Strengths & Difficulties Questionnaire: For Age 4-17gulittNo ratings yet
- Mmpi-3 Sample Score ReportDocument11 pagesMmpi-3 Sample Score ReportMohammad Hassan Haji HosseiniNo ratings yet
- Counselors For Social Justice Position Statement On DSM-5Document10 pagesCounselors For Social Justice Position Statement On DSM-5Julie R. AncisNo ratings yet
- Cca Outline With Summary ExampleDocument7 pagesCca Outline With Summary Exampleapi-460752676No ratings yet
- Clinical Rating Scales in Suicide AssessmentDocument8 pagesClinical Rating Scales in Suicide AssessmentCarol Artigas GómezNo ratings yet
- Reading 7 C TextsDocument3 pagesReading 7 C TextsNyan GyishinNo ratings yet
- Maxillary LandmarksDocument30 pagesMaxillary LandmarksRajsandeep Singh86% (14)
- Microlife BP A3 Plus: EN ES FR IT DE TR PT NL GR ARDocument81 pagesMicrolife BP A3 Plus: EN ES FR IT DE TR PT NL GR ARYatzy Choi NekitoNo ratings yet
- EpidemiologyDocument100 pagesEpidemiologyKailash NagarNo ratings yet
- Uber CEO EmailDocument5 pagesUber CEO EmailKhristopher J. BrooksNo ratings yet
- 12 SM 2017 Biology EngDocument206 pages12 SM 2017 Biology EngJaiminGajjar100% (1)
- TVEC Guide to Sri Lanka's Vocational Education SystemDocument31 pagesTVEC Guide to Sri Lanka's Vocational Education Systemshishir_cNo ratings yet
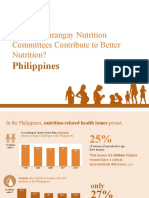
- How Do Barangay Nutrition Committees Contribute To Better Nutrition?Document20 pagesHow Do Barangay Nutrition Committees Contribute To Better Nutrition?Angelito CortunaNo ratings yet
- Intelligent ConstructionDocument4 pagesIntelligent ConstructionRikesh SapkotaNo ratings yet
- Pelvic Organ Prolapse After Laparoscopic Hysterectomy Compared With Vaginal Hysterectomy: The POP-UP StudyDocument10 pagesPelvic Organ Prolapse After Laparoscopic Hysterectomy Compared With Vaginal Hysterectomy: The POP-UP Studymuhammadnurul asmiNo ratings yet
- COMS322 Test Prep 4Document3 pagesCOMS322 Test Prep 4RisalNo ratings yet
- Syllabus Level 1 PDFDocument6 pagesSyllabus Level 1 PDFSwaprakash RoyNo ratings yet
- Occupational Therapy Practice Framework: Domain and Process Fourth Edition (2020)Document87 pagesOccupational Therapy Practice Framework: Domain and Process Fourth Edition (2020)Susana Ahumada100% (1)
- Course Outline - 664759538modular Curriculum For Pharmacy Students, September 2013Document357 pagesCourse Outline - 664759538modular Curriculum For Pharmacy Students, September 2013Sebaha TijoNo ratings yet
- Research Proposal 4Document3 pagesResearch Proposal 4api-385647692No ratings yet
- Leica Cryostat 1860 ManualDocument98 pagesLeica Cryostat 1860 ManualEmilio Fernandez LimónNo ratings yet
- 27 Annual ReportDocument102 pages27 Annual Reportudiptya_papai2007No ratings yet
- Cpale 2022Document3 pagesCpale 2022Mario ErazoNo ratings yet
- The Kübler-Ross Change Curve: Emotional Response To ChangeDocument9 pagesThe Kübler-Ross Change Curve: Emotional Response To ChangeChanel PostelNo ratings yet
- Bed Bath Procedure by Lydia Appiah Baffoe & Harriet Appiah KubiDocument28 pagesBed Bath Procedure by Lydia Appiah Baffoe & Harriet Appiah KubiGeorge Kwaku KetorNo ratings yet
- Sodium Bicarbonate: PresentationDocument3 pagesSodium Bicarbonate: Presentationmadimadi11No ratings yet
- FMU 101 - Chap 4 - Test Taking Strategies Part IIDocument11 pagesFMU 101 - Chap 4 - Test Taking Strategies Part IIMario LaraNo ratings yet
- ML SyllDocument2 pagesML Syllmurlak37No ratings yet
- Beliefs About Obsessional Thoughts InventoryDocument21 pagesBeliefs About Obsessional Thoughts InventoryMarta CerdáNo ratings yet
- Improving Project ProposalsDocument2 pagesImproving Project ProposalsNancy Nicasio SanchezNo ratings yet
- Alternative Feed for ChickensDocument28 pagesAlternative Feed for ChickensClaudens Printing ServicesNo ratings yet
- Alexthymia in Sexual Disorder Clinic PatientsDocument7 pagesAlexthymia in Sexual Disorder Clinic PatientsFélix Aníbal Acuña OlivosNo ratings yet
- A Six Step Approach To Writing A Formal SummaryDocument5 pagesA Six Step Approach To Writing A Formal SummaryБезымянный КактусNo ratings yet
- NCP Self EsteemDocument3 pagesNCP Self EsteemAlfadz AsakilNo ratings yet
- Launching of The Internet-Based Education ProgramDocument6 pagesLaunching of The Internet-Based Education ProgramaminoacidNo ratings yet





![ASWB EXAMINATION IN SOCIAL WORK [ASWB] (1 VOL.): Passbooks Study Guide](https://imgv2-1-f.scribdassets.com/img/word_document/402068986/149x198/afec08b5ad/1617230405?v=1)