You might also like
- Gestational Weight GainDocument3 pagesGestational Weight GainainindyaNo ratings yet
- Research PaperDocument18 pagesResearch Paperapi-545542584No ratings yet
- Journal Pone 0173937Document15 pagesJournal Pone 0173937Julenda CintarinovaNo ratings yet
- Nursing Research Final PaperDocument19 pagesNursing Research Final Paperapi-545362651No ratings yet
- Effects of Prepregnancy Dietary Patterns On Infant Birth Weight A Prospective Cohort StudyDocument11 pagesEffects of Prepregnancy Dietary Patterns On Infant Birth Weight A Prospective Cohort StudyLola SantiaNo ratings yet
- Energy Requirements and Recommended Weight Gain in PregnancyDocument4 pagesEnergy Requirements and Recommended Weight Gain in PregnancyMegaNo ratings yet
- Pregnancy Exercise Overweight MetaanalysisDocument11 pagesPregnancy Exercise Overweight MetaanalysisAisleenHNo ratings yet
- s12884 022 04542 0Document10 pagess12884 022 04542 0Risma Ripfandiana SariNo ratings yet
- Nutrients 08 00342 With CoverDocument6 pagesNutrients 08 00342 With Coverredactor 1No ratings yet
- 02 003 ValsamakisDocument13 pages02 003 ValsamakisCostin VrabieNo ratings yet
- Exercise in Pregnant Women and Birth WeightDocument4 pagesExercise in Pregnant Women and Birth WeightJelita SihombingNo ratings yet
- Diabetic MaternlaDocument4 pagesDiabetic MaternlaAde Gustina SiahaanNo ratings yet
- 2017 Article 632 PDFDocument11 pages2017 Article 632 PDFJauhiraNo ratings yet
- Maternal Diet, BreastfeedingDocument6 pagesMaternal Diet, BreastfeedingRiska Diene PratiwiNo ratings yet
- The Effects of Vigorous Intensity Exercise in The Third Trimester of Pregnancy A Systematic Review and MetaanalysisDocument18 pagesThe Effects of Vigorous Intensity Exercise in The Third Trimester of Pregnancy A Systematic Review and MetaanalysisJaqueline OliveiraNo ratings yet
- Pregnancy Weight GainDocument9 pagesPregnancy Weight GainKevin MulyaNo ratings yet
- Nutrition in Pregnancy: Basic Principles and RecommendationsDocument7 pagesNutrition in Pregnancy: Basic Principles and Recommendationssuci triana putriNo ratings yet
- Maternal Anthropometry and Low Birth Weight: A Review: G. Devaki and R. ShobhaDocument6 pagesMaternal Anthropometry and Low Birth Weight: A Review: G. Devaki and R. ShobhaJihan PolpokeNo ratings yet
- 2017 Article 1291Document9 pages2017 Article 1291afanafisNo ratings yet
- Começando CedoDocument14 pagesComeçando Cedojulianapaiva05No ratings yet
- Maternal Exercise During Pregnancy Reduces The Risk of Preterm Birth Through The Mediating Role of PlacentaDocument9 pagesMaternal Exercise During Pregnancy Reduces The Risk of Preterm Birth Through The Mediating Role of Placentasjulianacr04No ratings yet
- Effects of Physical Activity During Pregnancy On Neonatal Birth WeightDocument8 pagesEffects of Physical Activity During Pregnancy On Neonatal Birth WeightRitmaNo ratings yet
- Jurnal ViolenceDocument6 pagesJurnal ViolenceIris BerlianNo ratings yet
- The Effect of Yoga On The Delivery and Neonatal Outcomes in Nulliparous Pregnant Women in Iran: A Clinical Trial StudyDocument9 pagesThe Effect of Yoga On The Delivery and Neonatal Outcomes in Nulliparous Pregnant Women in Iran: A Clinical Trial StudyErica Ade WahyuniNo ratings yet
- Maternal and Early-Life Nutrition and HealthDocument4 pagesMaternal and Early-Life Nutrition and HealthTiffani_Vanessa01No ratings yet
- An Overview of Maternal and Fetal Short and Long-Term Impact of Physical Activity During PregnancyDocument11 pagesAn Overview of Maternal and Fetal Short and Long-Term Impact of Physical Activity During Pregnancyalvaro alarconNo ratings yet
- Final Research Paper - Maternal Risks OutcomesDocument12 pagesFinal Research Paper - Maternal Risks Outcomesapi-354198040No ratings yet
- Davies 2016Document9 pagesDavies 2016Agung GuretnoNo ratings yet
- Effect of Antenatal Dietary Interventions in Maternal Obesity On Pregnancy Weight Gain and Birthweight Healthy Mums and Babies (HUMBA) Randomized TrialDocument13 pagesEffect of Antenatal Dietary Interventions in Maternal Obesity On Pregnancy Weight Gain and Birthweight Healthy Mums and Babies (HUMBA) Randomized TrialAripin Ari AripinNo ratings yet
- Physical InterventionDocument9 pagesPhysical Interventionconstantius augustoNo ratings yet
- Nutrition Counseling During Pregnancy On Maternal Weight GainDocument4 pagesNutrition Counseling During Pregnancy On Maternal Weight GainAbha AyushreeNo ratings yet
- Impact of Maternal Probiotic Supplemented Dietary Counselling On Pregnancy Outcome and Prenatal and Postnatal Growth A Double Blind Placebo Controlled StudyDocument8 pagesImpact of Maternal Probiotic Supplemented Dietary Counselling On Pregnancy Outcome and Prenatal and Postnatal Growth A Double Blind Placebo Controlled Studytami ariyasraNo ratings yet
- Roggero Et Al., 2011Document7 pagesRoggero Et Al., 2011Luana BarrosNo ratings yet
- Metgud Factors Affecting Birth Weight of A Newborn - A Community Based Study in Rural Karnataka, IndiaDocument4 pagesMetgud Factors Affecting Birth Weight of A Newborn - A Community Based Study in Rural Karnataka, IndiajanetNo ratings yet
- Nutrition in Pregnancy Basic Principles and RecommendationsDocument6 pagesNutrition in Pregnancy Basic Principles and RecommendationsAndrea Hinostroza PinedoNo ratings yet
- Protocol - PaedsDocument3 pagesProtocol - PaedsShradha PrakashNo ratings yet
- Being Macrosomic at Birth Is An Independent Predictor of Overweight in Children: Results From The IDEFICS StudyDocument9 pagesBeing Macrosomic at Birth Is An Independent Predictor of Overweight in Children: Results From The IDEFICS StudySayuri BenitesNo ratings yet
- Singhal Susu Formula 2010Document12 pagesSinghal Susu Formula 2010Anezakii MahannaniiNo ratings yet
- Body Composition in First 10 DaysDocument7 pagesBody Composition in First 10 DaysThaíssa CasagrandeNo ratings yet
- Nutrition in Pregnancy Basic Principles and RecommendationsDocument2 pagesNutrition in Pregnancy Basic Principles and RecommendationsMegaNo ratings yet
- Lactation and Contraception: ReviewDocument7 pagesLactation and Contraception: ReviewAnca CucuNo ratings yet
- Maternal Obesity and High-Fat Diet Program Offspring Metabolic SyndromeDocument13 pagesMaternal Obesity and High-Fat Diet Program Offspring Metabolic SyndromeMuhammad BasriNo ratings yet
- Pregnancy Weight Gain in Twin Gestations and Maternal and Child Health Outcomes at 5 YearsDocument16 pagesPregnancy Weight Gain in Twin Gestations and Maternal and Child Health Outcomes at 5 YearsMariela PrietoNo ratings yet
- Ijwh 5 501Document7 pagesIjwh 5 501MarianaafiatiNo ratings yet
- Literature Review Obesity in PregnancyDocument6 pagesLiterature Review Obesity in Pregnancyafmzbdjmjocdtm100% (1)
- Maternal Dietary Intake and Physical Activity Habits During The Postpartum Period: Associations With Clinician Advice in A Sample of Australian First Time MothersDocument10 pagesMaternal Dietary Intake and Physical Activity Habits During The Postpartum Period: Associations With Clinician Advice in A Sample of Australian First Time MothersEva MulifahNo ratings yet
- Goodnight W. Optimal Nutrition For Improved....Document14 pagesGoodnight W. Optimal Nutrition For Improved....cvillafane1483No ratings yet
- Cme Reviewarticle: Current Concepts of Maternal NutritionDocument14 pagesCme Reviewarticle: Current Concepts of Maternal NutritionAllan V. MouraNo ratings yet
- Jurnal PDFDocument5 pagesJurnal PDFWaica PratiwiNo ratings yet
- Obesidad y ReproducciónDocument2 pagesObesidad y ReproducciónJaviera FranciscaNo ratings yet
- International Breastfeeding JournalDocument6 pagesInternational Breastfeeding JournalDitha FadhilaNo ratings yet
- IntroductionDocument3 pagesIntroductionZahra 9oNo ratings yet
- Nutrients 15 00988Document17 pagesNutrients 15 00988VIRGINA PUTRINo ratings yet
- Beneficios Del Ejercicio en La Mujer EmbarazadaDocument12 pagesBeneficios Del Ejercicio en La Mujer EmbarazadaRitaNo ratings yet
- Weight Gain in Pregnancy: Stephan RossnerDocument6 pagesWeight Gain in Pregnancy: Stephan RossnerKumah WisdomNo ratings yet
- Yong 2016Document8 pagesYong 2016yongyew2No ratings yet
- Role of Gastric Lavage in Newborn With Meconium Stained Amniotic Fluid:a Randomized Controlled TrailDocument3 pagesRole of Gastric Lavage in Newborn With Meconium Stained Amniotic Fluid:a Randomized Controlled TrailtriaanggareniNo ratings yet
- ARTICULO DE REVISION. OBESIDAD MATERNA Y PROGRAMACIÓN PRENATAL en WordDocument5 pagesARTICULO DE REVISION. OBESIDAD MATERNA Y PROGRAMACIÓN PRENATAL en WordrosaNo ratings yet
- Hiperemesis Gravidarum Di Rumah Sakit Pku Muhammadiyah GubugDocument13 pagesHiperemesis Gravidarum Di Rumah Sakit Pku Muhammadiyah GubugArina SaputriNo ratings yet
- Community Health Nursing BookDocument96 pagesCommunity Health Nursing BookSamantha Renei SanchezNo ratings yet
- May Not Occur To Everyone Does Not Come at A Specified Period Varies Across All People May Coincide With Physical Limitations of The BodyDocument4 pagesMay Not Occur To Everyone Does Not Come at A Specified Period Varies Across All People May Coincide With Physical Limitations of The BodyPatrick MatibagNo ratings yet
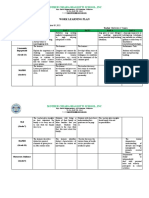
- September 05, 2022 - September 09, 2022Document2 pagesSeptember 05, 2022 - September 09, 2022Maybelyn de los ReyesNo ratings yet
- 21st Century Managerial and Leadership SkillsDocument19 pages21st Century Managerial and Leadership SkillsRichardRaqueno80% (5)
- Sense Memory 11: Private MomentDocument5 pagesSense Memory 11: Private MomentJonathan Samarro100% (4)
- Microteaching: MDR - TBDocument16 pagesMicroteaching: MDR - TBVikram Singh RanawatNo ratings yet
- 2-Vision Zero GuideDocument11 pages2-Vision Zero GuideMohd Afifi HashimNo ratings yet
- The ADHD Diagnosis GuideDocument13 pagesThe ADHD Diagnosis GuideArunima KapoorNo ratings yet
- Drug-Study ErgonDocument2 pagesDrug-Study ErgonPaolo UyNo ratings yet
- Peads Quiz MCQSDocument10 pagesPeads Quiz MCQSM.A. Ch.No ratings yet
- 5 Gifts For An Abundant Life. Create A Consciousness of Wealth (PDFDrive)Document178 pages5 Gifts For An Abundant Life. Create A Consciousness of Wealth (PDFDrive)AGANAH EmmanuelNo ratings yet
- Quiz Comprehension and Error Identification W2Document3 pagesQuiz Comprehension and Error Identification W2norlianaNo ratings yet
- Final Agenda - Deciphering MorphologyDocument4 pagesFinal Agenda - Deciphering MorphologySaket KumarNo ratings yet
- 0088-SS-C-MS-0035 Method Statement Foundation Work Rev 0 (1) Rev 2Document22 pages0088-SS-C-MS-0035 Method Statement Foundation Work Rev 0 (1) Rev 2edvanNo ratings yet
- Dialysis Cover LetterDocument5 pagesDialysis Cover Letterdthtrtlfg100% (2)
- Literature Matrix Research FinalDocument18 pagesLiterature Matrix Research FinalArianne Macy GarciaNo ratings yet
- SEMI-DETAILED LESSON PLAN EDUC FacilitatDocument3 pagesSEMI-DETAILED LESSON PLAN EDUC FacilitatBebot A. CabuguasNo ratings yet
- Term Exam Answer Sheet EnglishDocument11 pagesTerm Exam Answer Sheet Englishsameera gupteNo ratings yet
- Question Test 2 Oshm Aug 2021Document3 pagesQuestion Test 2 Oshm Aug 2021Syamala 29No ratings yet
- GeneticsDocument32 pagesGeneticsyuuki konnoNo ratings yet
- PM 303 Assignment Example DayCareCentre NewDocument13 pagesPM 303 Assignment Example DayCareCentre NewSalman SultanNo ratings yet
- Telaah Kritis Artikel Terapi PZ 2020Document7 pagesTelaah Kritis Artikel Terapi PZ 2020dewi arifahniNo ratings yet
- Complete Textbook of Phlebotomy 5th Edition Hoeltke Test BankDocument5 pagesComplete Textbook of Phlebotomy 5th Edition Hoeltke Test BankedwardbangeieNo ratings yet
- Argument Prospectus: Should Tobacco Products Be Banned?Document3 pagesArgument Prospectus: Should Tobacco Products Be Banned?Donny TraumaNo ratings yet
- Bow Hope - Perdev.eappDocument3 pagesBow Hope - Perdev.eappJelly Shane GorospeNo ratings yet
- Crim 5 Module 2Document14 pagesCrim 5 Module 2Gemie B. EspinaNo ratings yet
- Vyr Us 2000108 Ltv1200 Emergency Preparedness Brochure FinalDocument4 pagesVyr Us 2000108 Ltv1200 Emergency Preparedness Brochure FinalHarrrya hady WidjayaNo ratings yet
- The Present (Universal Truth)Document111 pagesThe Present (Universal Truth)Hitesh YadavNo ratings yet
- Donald Supers TheoryDocument20 pagesDonald Supers TheorytereNo ratings yet
- Pi Anterior ResectionDocument16 pagesPi Anterior ResectionEnika Natalia Christi TilaarNo ratings yet