You might also like
- Emergency Response PlanDocument24 pagesEmergency Response PlanArdi Pratama100% (2)
- BattleTech - Magazine - Commander Quarterly, Issue 3067 - (WizKids Product)Document54 pagesBattleTech - Magazine - Commander Quarterly, Issue 3067 - (WizKids Product)toddtimlake2336100% (1)
- SnakesDocument4 pagesSnakessathya62No ratings yet
- Handbook On Treatment Guidelines For Snake Bite and Scorpion Sting 2008 - TNHSP PublicationDocument118 pagesHandbook On Treatment Guidelines For Snake Bite and Scorpion Sting 2008 - TNHSP PublicationDr.Sagindar75% (4)
- Dr. Dr. Tri Maharani, M.si., Sp. em - Snake Bite Medical Management CrebonDocument33 pagesDr. Dr. Tri Maharani, M.si., Sp. em - Snake Bite Medical Management Crebonrio100% (1)
- Management of Snake Bite National Guideline 2014Document66 pagesManagement of Snake Bite National Guideline 2014jonmax86No ratings yet
- Hand Book On Treatment Guidelines For Snake Bite and Scorpion StingDocument129 pagesHand Book On Treatment Guidelines For Snake Bite and Scorpion StingBruno100% (8)
- Snake Bite Injury: - PRESENTOR-Dr Varsha N Shetty - Moderator-Dr Nagaraj ShettyDocument64 pagesSnake Bite Injury: - PRESENTOR-Dr Varsha N Shetty - Moderator-Dr Nagaraj ShettyDr. Apoorva KottaryNo ratings yet
- Geography One Liner Ias Pcs PathshalaDocument198 pagesGeography One Liner Ias Pcs PathshalaAkshay Kumar100% (2)
- Radha Theke Poschimbongo: A journey Through Four MilleniumFrom EverandRadha Theke Poschimbongo: A journey Through Four MilleniumRating: 3 out of 5 stars3/5 (2)
- Snake Bite ICU ManagementDocument52 pagesSnake Bite ICU Managementperfectdoc100% (3)
- Indigenous Cattle Breeds of India - EnglishDocument13 pagesIndigenous Cattle Breeds of India - EnglishBharat MundheNo ratings yet
- Livestock Breeds - Specific FeaturesDocument11 pagesLivestock Breeds - Specific FeaturesShanmathiNo ratings yet
- Tribal GroupsDocument5 pagesTribal GroupsRahul BarnwalNo ratings yet
- Threatened Plants Maharashtra PDFDocument5 pagesThreatened Plants Maharashtra PDFSandipNanawareNo ratings yet
- Cattle and Buffalo Breeds Important CharacteristicsDocument2 pagesCattle and Buffalo Breeds Important Characteristicsmyacc992006No ratings yet
- Major Insect Problems-2015-16 To 2021-22Document3 pagesMajor Insect Problems-2015-16 To 2021-22Kaushal NaikNo ratings yet
- UPSC Civil Services Examination: UPSC Notes (GS-I) Topic: Major Crops in India (Geography Notes For UPSC)Document2 pagesUPSC Civil Services Examination: UPSC Notes (GS-I) Topic: Major Crops in India (Geography Notes For UPSC)Bhupender GhosliyaNo ratings yet
- Reptile Rap #10 (Jun 2010)Document28 pagesReptile Rap #10 (Jun 2010)ReticulatusNo ratings yet
- Follow Us Indian State Animals, Birds, Flowers, Trees With Nick NamesDocument11 pagesFollow Us Indian State Animals, Birds, Flowers, Trees With Nick NamesM. Amebari NongsiejNo ratings yet
- Tribes and List of TribesDocument10 pagesTribes and List of TribesVishal SinghNo ratings yet
- Major Crops Grown in IndiaDocument2 pagesMajor Crops Grown in IndiaKiran ModapalleNo ratings yet
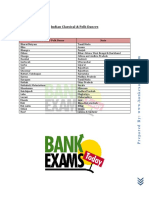
- Indian Classical & Folk Dances PDFDocument1 pageIndian Classical & Folk Dances PDFdharmaNo ratings yet
- Indian Classical & Folk DancesDocument1 pageIndian Classical & Folk DancesRaja O Romeyo NaveenNo ratings yet
- List of Indus Valley Civilisation Sites - WikipediaDocument11 pagesList of Indus Valley Civilisation Sites - WikipediaGOPALAKRISHNAN RAGOTHAMANNo ratings yet
- Nameri GuidebookDocument41 pagesNameri GuidebookWild Mahseer100% (1)
- Chhattisgarh GK-2Document2 pagesChhattisgarh GK-2dipteeagrawal48No ratings yet
- IB 19 4 Sofi OrientalScopsOwlDocument2 pagesIB 19 4 Sofi OrientalScopsOwlprintstore623No ratings yet
- Puppetry, Theatre Forms, Musical InstrumentDocument2 pagesPuppetry, Theatre Forms, Musical InstrumentMeghna TripathiNo ratings yet
- List of Indian Timber Trees WikipediaDocument5 pagesList of Indian Timber Trees WikipediaxiaoboshiNo ratings yet
- 1 5163445404494201495Document56 pages1 5163445404494201495Kartik JoshiNo ratings yet
- Biodiversity Heritage SitesDocument5 pagesBiodiversity Heritage SitesAnupam KherNo ratings yet
- Breeds 2017Document18 pagesBreeds 2017Sagar PatelNo ratings yet
- Tribal Communities in News: National Ias Academy Super40 (Booklet Number - 14) CONTACT: 9632334466Document3 pagesTribal Communities in News: National Ias Academy Super40 (Booklet Number - 14) CONTACT: 9632334466narottam kumar SinghNo ratings yet
- Traditional Rainwater Harvesting in India - Shekhar Raghavan - Akash Ganga TrustDocument3 pagesTraditional Rainwater Harvesting in India - Shekhar Raghavan - Akash Ganga Trustvidhan tiwariNo ratings yet
- Geography (English) One LinerDocument198 pagesGeography (English) One LinerappuNo ratings yet
- Tribals in India: Name: Bikrant Roy Class: Vii B' Roll No: 06 Subject: SSTDocument26 pagesTribals in India: Name: Bikrant Roy Class: Vii B' Roll No: 06 Subject: SSTSenthil KumarNo ratings yet
- SpeciesDocument22 pagesSpeciesVivek ShahiNo ratings yet
- Tribes of India-Quick Revision TableDocument18 pagesTribes of India-Quick Revision TablePraveen RawatNo ratings yet
- Bihar Map Based FactsDocument2 pagesBihar Map Based FactsSadira SafaqNo ratings yet
- Geography Part 9 Soils in IndiaDocument3 pagesGeography Part 9 Soils in IndiaServant of ALLAHNo ratings yet
- Cow Breeds of IndiaDocument10 pagesCow Breeds of IndiaBalaji RamamurtiNo ratings yet
- InscriptionsDocument9 pagesInscriptionseennav90No ratings yet
- Present Locations and Important Events in Ancient Mahabharata TimesDocument7 pagesPresent Locations and Important Events in Ancient Mahabharata TimesSuripeddi KoundinyaNo ratings yet
- IB 16 3 MohantyETAL BlackcappedKingfisherDocument3 pagesIB 16 3 MohantyETAL BlackcappedKingfishersumit aryaNo ratings yet
- Tribes in IndiaDocument19 pagesTribes in IndiaChinmoy BhattacharyyaNo ratings yet
- LA EX RRP 2021 INDIAN GEOGRAPHY @upsc - ThoughtDocument59 pagesLA EX RRP 2021 INDIAN GEOGRAPHY @upsc - ThoughtYashwant Singh RathoreNo ratings yet
- Areca TriandraDocument4 pagesAreca Triandraahil XO1BDNo ratings yet
- ENV - Endangered Birds PDFDocument4 pagesENV - Endangered Birds PDFChess ChessNo ratings yet
- Major Crops: Crop Details Region Grown in India World Sr. No. Lead Producers in India Largest Producer ChinaDocument2 pagesMajor Crops: Crop Details Region Grown in India World Sr. No. Lead Producers in India Largest Producer ChinaFalguni MathewsNo ratings yet
- Major Rivers and Their TributariesDocument2 pagesMajor Rivers and Their TributariesShah Khan100% (1)
- Major Points About Gujarat-Know Your States in PDF For SSC, Bank ExamsDocument6 pagesMajor Points About Gujarat-Know Your States in PDF For SSC, Bank ExamsHuman FundaNo ratings yet
- 07 Neoheterophrictus Smithi Gujarat First Record DMB NPM ADRDocument4 pages07 Neoheterophrictus Smithi Gujarat First Record DMB NPM ADRprasanNo ratings yet
- KINGKOBRARecord Q-1Document4 pagesKINGKOBRARecord Q-1RAHUL SHINDENo ratings yet
- Assam GK - PDF (Assam Competitive Exam)Document7 pagesAssam GK - PDF (Assam Competitive Exam)UAB MediaworksNo ratings yet
- Major Points About Assam - Know Your State in PDF For SSC, Bank ExamsDocument6 pagesMajor Points About Assam - Know Your State in PDF For SSC, Bank Examsedify educationNo ratings yet
- Current Affairs and GKDocument5 pagesCurrent Affairs and GKchinna12345No ratings yet
- Tribes Nomads and Settled CommunitiesDocument2 pagesTribes Nomads and Settled CommunitiesAnmol VIshwakarmaNo ratings yet
- PD/2007/AugustDocument1 pagePD/2007/AugustAravindVRNo ratings yet
- Soil Type Categories and Districts - Government-Of-Madhya-Pradesh, IndiaDocument2 pagesSoil Type Categories and Districts - Government-Of-Madhya-Pradesh, IndiaMayur MittalNo ratings yet
- The Term River System Refers To TheDocument3 pagesThe Term River System Refers To TheExecutive Officer Dhekiajuli APNo ratings yet
- Rabari CommunityDocument12 pagesRabari CommunityMayank Joshi50% (2)
- 29amazing Animal Facts: Plants and AnimalsDocument6 pages29amazing Animal Facts: Plants and AnimalsMohit ChinchkhedeNo ratings yet
- University Assistant Micro NotesDocument4 pagesUniversity Assistant Micro NotesNagarajan ValliNo ratings yet
- Maize Cultivars 1969-2017 PDFDocument65 pagesMaize Cultivars 1969-2017 PDFAshish RathodeNo ratings yet
- Reptile Rap #12 (May 2011)Document12 pagesReptile Rap #12 (May 2011)ReticulatusNo ratings yet
- Indian TribesDocument2 pagesIndian Tribespriyam duttaNo ratings yet
- Attachment RIVERS AND TRIBUTARIES Lyst4463Document14 pagesAttachment RIVERS AND TRIBUTARIES Lyst4463snapyn9No ratings yet
- Tiger ReservesDocument12 pagesTiger ReservesdvsdguNo ratings yet
- An Inventory and Assessment of Snake Diversity Ofgandhamardan Hills Range of Western Orissa IndiaDocument5 pagesAn Inventory and Assessment of Snake Diversity Ofgandhamardan Hills Range of Western Orissa IndiaShivraj ShindeNo ratings yet
- RAMPHOTYPHLOPS BRAMINUS (Brahminy Blind Snake) : Geographic DistributionDocument2 pagesRAMPHOTYPHLOPS BRAMINUS (Brahminy Blind Snake) : Geographic DistributionShivraj ShindeNo ratings yet
- Poisonous and Non-Poisonous Snakes DifferencesDocument3 pagesPoisonous and Non-Poisonous Snakes DifferencesShivraj ShindeNo ratings yet
- The Indian Wildlife (Protection) Act, 1972: (As Amended Upto 1993)Document7 pagesThe Indian Wildlife (Protection) Act, 1972: (As Amended Upto 1993)Shivraj ShindeNo ratings yet
- Snake Bite Prevention and Management in Rural IndiDocument1 pageSnake Bite Prevention and Management in Rural IndiShivraj ShindeNo ratings yet
- Cheklist of Reptiles of PakistanDocument8 pagesCheklist of Reptiles of PakistanShivraj ShindeNo ratings yet
- 297-306 01 Wagner1Document11 pages297-306 01 Wagner1Shivraj ShindeNo ratings yet
- Impact of Mechanisation On Socio Economic Condition of Donkey Guardians of District Sangli - Maharashtra - IndiaDocument9 pagesImpact of Mechanisation On Socio Economic Condition of Donkey Guardians of District Sangli - Maharashtra - IndiaShivraj ShindeNo ratings yet
- Cambodia LegislationDocument6 pagesCambodia LegislationTheng.SethNo ratings yet
- MO Training Book - WB - Snake Bite-Animal Bite - Common Poisonous BitesDocument88 pagesMO Training Book - WB - Snake Bite-Animal Bite - Common Poisonous BitesAnindya BiswasNo ratings yet
- Reptile Rap #13 (Sep 2011)Document16 pagesReptile Rap #13 (Sep 2011)ReticulatusNo ratings yet
- ZOOTOXINSDocument72 pagesZOOTOXINSSunil83% (6)
- Part 3Document196 pagesPart 3sdsaNo ratings yet
- Part A-7-Snake BiteDocument7 pagesPart A-7-Snake Bitefernanda1rondelli0% (1)
- Management of Snake Bite in India: Shibendu Ghosh, Prabuddha MukhopadhyayDocument6 pagesManagement of Snake Bite in India: Shibendu Ghosh, Prabuddha MukhopadhyaychandanNo ratings yet
- Clinical Practice Guideline:: Management of Venomous Snake BitesDocument54 pagesClinical Practice Guideline:: Management of Venomous Snake BitesBeni BolngNo ratings yet
- Snake Bite National Protocol PediatricsDocument45 pagesSnake Bite National Protocol Pediatricsarjun_paulNo ratings yet
- Snakebite QRG PDFDocument65 pagesSnakebite QRG PDFDESYNo ratings yet
- Snakebite Management Guide For Healthcare Providers in Malaysia 2011Document8 pagesSnakebite Management Guide For Healthcare Providers in Malaysia 2011fifa_0304535100% (1)
- Evaluation of Snake Repellents Against The Principal Venomous Snakes of India in Laboratory ConditionDocument7 pagesEvaluation of Snake Repellents Against The Principal Venomous Snakes of India in Laboratory ConditionRajesh KumarNo ratings yet
- Snakebite Treatment ProtocolDocument24 pagesSnakebite Treatment ProtocolravanoidNo ratings yet
- AntivenomDocument1 pageAntivenomAbu RaihanNo ratings yet
- 8 19 Management of Snake Bites PDFDocument12 pages8 19 Management of Snake Bites PDFdawnkuruvillaNo ratings yet
- Snake BiteDocument46 pagesSnake Bitejerly lNo ratings yet
- Poisonous Snakes in BangladeshDocument27 pagesPoisonous Snakes in BangladeshKazi AlmuqtadirNo ratings yet
- Distinction Between Poisonous and NonDocument9 pagesDistinction Between Poisonous and NonمحمدأميندماجNo ratings yet
- Medically Important Snakes in Sri Lanka Ver. 3 17.11.20191Document5 pagesMedically Important Snakes in Sri Lanka Ver. 3 17.11.20191Amila ShyamalNo ratings yet
- ATLS FatmawatiDocument35 pagesATLS FatmawatiAnindya Anjas PutriaviNo ratings yet
- National Guideline For Snakebite Management in Nepal 2019Document100 pagesNational Guideline For Snakebite Management in Nepal 2019VT BabuNo ratings yet