You might also like
- Fever NCPDocument5 pagesFever NCPNikael Patun-ogNo ratings yet
- Portex Ambulatory Chest Drainage Brochure - Portex - SmithDocument2 pagesPortex Ambulatory Chest Drainage Brochure - Portex - SmithCampaign MediaNo ratings yet
- Methods of Colostomy Construction No Effect On.6Document8 pagesMethods of Colostomy Construction No Effect On.6Charles CardosoNo ratings yet
- The Stamp Technique For Direct Class II Composite Restorations: A Case SeriesDocument6 pagesThe Stamp Technique For Direct Class II Composite Restorations: A Case SeriesFasich BaihaqiNo ratings yet
- Biomechanical Comparison of Meniscus-Suture Constructs For Pullout Repair of Medial Meniscus Posterior Root TearsDocument6 pagesBiomechanical Comparison of Meniscus-Suture Constructs For Pullout Repair of Medial Meniscus Posterior Root Tearsdados2000No ratings yet
- Extended Trochanteric Osteotomy in Revision Total Hip Arthroplasty - Contemporary Outcomes of 612 HipsDocument12 pagesExtended Trochanteric Osteotomy in Revision Total Hip Arthroplasty - Contemporary Outcomes of 612 Hips阿欧有怪兽No ratings yet
- Int Endodontic J - 2022 - Chaniotis - Present Status and Future Directions Management of Curved and Calcified Root CanalsDocument29 pagesInt Endodontic J - 2022 - Chaniotis - Present Status and Future Directions Management of Curved and Calcified Root CanalsDaniel Martínez VásquezNo ratings yet
- J Aanat 2021 151779Document10 pagesJ Aanat 2021 151779snkidNo ratings yet
- 논문원문Document4 pages논문원문Donghee LeeNo ratings yet
- The Use of Bioceramics As Root-End Filling Materials in Periradicular Surgery: A Literature ReviewDocument10 pagesThe Use of Bioceramics As Root-End Filling Materials in Periradicular Surgery: A Literature ReviewpoojaNo ratings yet
- Jurnal Reading THTDocument7 pagesJurnal Reading THTSucii Sekar NingrumNo ratings yet
- Artigo EngimplanDocument6 pagesArtigo EngimplanKevinNo ratings yet
- Customized Thermoplast Retentive Aid For Partial Auricular Prosthesis-A Case ReportDocument9 pagesCustomized Thermoplast Retentive Aid For Partial Auricular Prosthesis-A Case ReportIJAR JOURNALNo ratings yet
- 22arun Thesis ArticleDocument8 pages22arun Thesis ArticlebhupendraNo ratings yet
- Evaluation of Continuous Arch and Segmented Arch Leveling Techniques in Adult Patients-A Clinical Study PDFDocument6 pagesEvaluation of Continuous Arch and Segmented Arch Leveling Techniques in Adult Patients-A Clinical Study PDFDiana Paola FontechaNo ratings yet
- A Prospective Clinical Study of Mineral Trioxide Aggregate and IRM When Used As Root End Filling Materials inDocument7 pagesA Prospective Clinical Study of Mineral Trioxide Aggregate and IRM When Used As Root End Filling Materials inernesto fidel aramendiz galindoNo ratings yet
- Becker 2018Document12 pagesBecker 2018Vinicius RechNo ratings yet
- CADCAM Technology For Implant Abutments, Crowns, and SuperstructuresDocument10 pagesCADCAM Technology For Implant Abutments, Crowns, and SuperstructuresJean OrtizNo ratings yet
- Literature - Review - of - Surgical 2020 - Excelente ResumoDocument13 pagesLiterature - Review - of - Surgical 2020 - Excelente ResumoliligunnerNo ratings yet
- Letter To The Editor - Re. - The Modified Socket Shield - (J Craniofac Surg, March 2018)Document10 pagesLetter To The Editor - Re. - The Modified Socket Shield - (J Craniofac Surg, March 2018)Cristina EneNo ratings yet
- Evaluation of Total Corneal Power MeasurementsDocument7 pagesEvaluation of Total Corneal Power MeasurementsMariana Luzardo bravoNo ratings yet
- Graftless Maxillary Sinus Lift Using Lateral.20Document8 pagesGraftless Maxillary Sinus Lift Using Lateral.20yuan.nisaratNo ratings yet
- Item Response Theory and Computerized Adaptive.3Document5 pagesItem Response Theory and Computerized Adaptive.3danebrosNo ratings yet
- 1 s2.0 S0169260722003911 MainDocument17 pages1 s2.0 S0169260722003911 MainAnand SolomonNo ratings yet
- RepairDocument11 pagesRepairTamer HamdyNo ratings yet
- The Use of Temporoparietal Fascia Flap For Surgical Treatment of Traumatic Auricle DefectsDocument5 pagesThe Use of Temporoparietal Fascia Flap For Surgical Treatment of Traumatic Auricle Defectslia indria watiNo ratings yet
- Canthopexy Evaluation - Anny SubillagaDocument2 pagesCanthopexy Evaluation - Anny SubillagaAnny SubillagaNo ratings yet
- Yahia Shape Memory Implants Yahia Shape Memory ImplantsDocument23 pagesYahia Shape Memory Implants Yahia Shape Memory ImplantsTejas krishnakanthNo ratings yet
- Artuculo EndodonciaDocument4 pagesArtuculo EndodonciaGiovanni VasconezNo ratings yet
- Elemental and Microstructural Analysis of Fake, Real, and Standard Orthodontic BracketsDocument7 pagesElemental and Microstructural Analysis of Fake, Real, and Standard Orthodontic BracketsdraNo ratings yet
- Yang 2019Document6 pagesYang 2019KevinNo ratings yet
- Review of A Single Surgeon's Stapedotomy Cases Performed With A Nickel Titanium Prosthesis Over A 14-Year PeriodDocument6 pagesReview of A Single Surgeon's Stapedotomy Cases Performed With A Nickel Titanium Prosthesis Over A 14-Year PeriodAbderrahim BOURIALNo ratings yet
- July 1Document8 pagesJuly 1Waseem AhmedNo ratings yet
- 10 23736@S1973-9087 17 04749-9Document8 pages10 23736@S1973-9087 17 04749-9Kings AndrewNo ratings yet
- ERRORSINIMPRESSIONMAKINGDocument86 pagesERRORSINIMPRESSIONMAKINGanushiNo ratings yet
- Errors in Impression MakingDocument86 pagesErrors in Impression MakingArinaNo ratings yet
- Incidence of Lower Eyelid Asymmetry: An Anthropometric Analysis of 204 PatientsDocument6 pagesIncidence of Lower Eyelid Asymmetry: An Anthropometric Analysis of 204 PatientsAndrewNo ratings yet
- Easjdom 43 91-96 FTDocument6 pagesEasjdom 43 91-96 FTTuan NguyenNo ratings yet
- 7khlqàxhqfhri¿ (Hgsurvwkhvhvrqshulrgrqwdokhdowk: (Olqd%Oxpd $Oglv9Lg) LV XQWLV LjxuvDocument10 pages7khlqàxhqfhri¿ (Hgsurvwkhvhvrqshulrgrqwdokhdowk: (Olqd%Oxpd $Oglv9Lg) LV XQWLV LjxuvJimmy Bryan Caparachini GuerreroNo ratings yet
- SurgNeurolInt 2012 3 1 68 97537 PDFDocument6 pagesSurgNeurolInt 2012 3 1 68 97537 PDFHumberto SandovalNo ratings yet
- Olfactory Outcomes After Middle Turbinate Resection in Endoscopic Transsphenoidal Surgery: A Prospective Randomized StudyDocument7 pagesOlfactory Outcomes After Middle Turbinate Resection in Endoscopic Transsphenoidal Surgery: A Prospective Randomized Studypaul00040No ratings yet
- (2009 Kotsovilis) A Systematic Review and Meta-Analysis On The Effect of Implant Length On The Survival of Rough-Surface Dental ImplantsDocument20 pages(2009 Kotsovilis) A Systematic Review and Meta-Analysis On The Effect of Implant Length On The Survival of Rough-Surface Dental Implantsyena1010No ratings yet
- Modified Technique of Underlay Myringoplasty: Journal of Otolaryngology-ENT ResearchDocument4 pagesModified Technique of Underlay Myringoplasty: Journal of Otolaryngology-ENT ResearchAkanshaNo ratings yet
- A Systematic Review and Meta-Analysis On The Effect of Implant Length On The Survival of Rough-Surface Dental ImplantsDocument20 pagesA Systematic Review and Meta-Analysis On The Effect of Implant Length On The Survival of Rough-Surface Dental Implantshkwgt7vskwNo ratings yet
- Mineral Trioxide Aggregate Applications in Endodontics: A ReviewDocument9 pagesMineral Trioxide Aggregate Applications in Endodontics: A ReviewKatherine CiezaNo ratings yet
- AJODO-2013 Erbe 143 6 760Document7 pagesAJODO-2013 Erbe 143 6 760player osamaNo ratings yet
- A Novel, Customizable Injection Protocol For Treatment of The Forehead With IncobotulinumtoxinA PDFDocument10 pagesA Novel, Customizable Injection Protocol For Treatment of The Forehead With IncobotulinumtoxinA PDFLewis PiersNo ratings yet
- Int Endodontic J 2022 Chaniotis Present Status and Future Directions Management of Curved and Calcified Root CanalsDocument29 pagesInt Endodontic J 2022 Chaniotis Present Status and Future Directions Management of Curved and Calcified Root Canalsreggae21No ratings yet
- 1 s2.0 S1349007922001335 Main 2Document6 pages1 s2.0 S1349007922001335 Main 2janeNo ratings yet
- Evaluation of The Fracture Resistance and Modulus of Elasticity of Commercially Available Core MaDocument4 pagesEvaluation of The Fracture Resistance and Modulus of Elasticity of Commercially Available Core MaSatya AsatyaNo ratings yet
- J Esthet Restor Dent - 2018 - Tezulas - Clinical Procedures Designs and Survival Rates of All Ceramic Resin Bonded FixedDocument12 pagesJ Esthet Restor Dent - 2018 - Tezulas - Clinical Procedures Designs and Survival Rates of All Ceramic Resin Bonded FixedS. BenzaquenNo ratings yet
- A Comparative Finite Element Analysis of Two Surgical Methods For CryptotiaDocument5 pagesA Comparative Finite Element Analysis of Two Surgical Methods For CryptotiaMaico Rendón de la CruzNo ratings yet
- Int Endodontic J - 2022 - Chaniotis - Present Status and Future Directions Management of Curved and Calcified Root CanalsDocument29 pagesInt Endodontic J - 2022 - Chaniotis - Present Status and Future Directions Management of Curved and Calcified Root CanalsLaura AmayaNo ratings yet
- S of Environmental Factors On Maxillofacial Elastomers: Part II-Report of SurveyDocument4 pagesS of Environmental Factors On Maxillofacial Elastomers: Part II-Report of SurveypalliNo ratings yet
- A Comparative Study of Microscopic and Endoscopic Type I TympanoplastyDocument4 pagesA Comparative Study of Microscopic and Endoscopic Type I TympanoplastyPutraNo ratings yet
- Implant Related Fractures of The Femur Following.4Document7 pagesImplant Related Fractures of The Femur Following.4ANA MARIA ROCIO HURTADO ORTEGANo ratings yet
- Double Duplicate Technique For Cad Cam Full Arch Immediate Loading A Technical Description and Case ReportDocument9 pagesDouble Duplicate Technique For Cad Cam Full Arch Immediate Loading A Technical Description and Case ReportYuki MuraNo ratings yet
- Open Vs Closed VIP2Document11 pagesOpen Vs Closed VIP2Ahmad FareedNo ratings yet
- Otitis MediaDocument6 pagesOtitis MedianonniNo ratings yet
- Eurheartj Intracoronary ImagingDocument20 pagesEurheartj Intracoronary ImagingDan PruneaNo ratings yet
- Visual Demand, Visual Ability and Vision Standards.4Document6 pagesVisual Demand, Visual Ability and Vision Standards.4ichmatul oktaveniNo ratings yet
- Journal of Cranio-Maxillo-Facial SurgeryDocument6 pagesJournal of Cranio-Maxillo-Facial SurgeryKihyun YooNo ratings yet
- Otoplasty Through Ventral Skin Incision and Shaping of The Antihelix by Abrasion-A Retrospective StudyDocument8 pagesOtoplasty Through Ventral Skin Incision and Shaping of The Antihelix by Abrasion-A Retrospective StudyKihyun YooNo ratings yet
- Otorhinolaryngology: Modified Bilateral Fasciaperichondrial Ap For Prominent Ear CorrectionDocument7 pagesOtorhinolaryngology: Modified Bilateral Fasciaperichondrial Ap For Prominent Ear CorrectionKihyun YooNo ratings yet
- Dupilumab Side Effect in A Patient With Atopic Dermatitis: A Case Report StudyDocument4 pagesDupilumab Side Effect in A Patient With Atopic Dermatitis: A Case Report StudyKihyun YooNo ratings yet
- A Rare Skin Infection in Atopic Dermatitis: A Case ReportDocument3 pagesA Rare Skin Infection in Atopic Dermatitis: A Case ReportKihyun YooNo ratings yet
- Article in Press: Quality of Life in Cushing's Disease: A Long Term Issue?Document6 pagesArticle in Press: Quality of Life in Cushing's Disease: A Long Term Issue?Kihyun YooNo ratings yet
- Kebutuhan Keluarga Pasien Di Ruang CCUDocument14 pagesKebutuhan Keluarga Pasien Di Ruang CCULita Vsi PekanbaruNo ratings yet
- PTC Application FormDocument1 pagePTC Application FormJose Mari F. EsguerraNo ratings yet
- Newswriting ExercisesDocument13 pagesNewswriting ExercisesMichelle Alejo CortezNo ratings yet
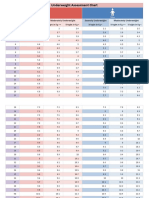
- Underweight Assessment Chart: Weight in KG Weight in KG Weight in KGDocument3 pagesUnderweight Assessment Chart: Weight in KG Weight in KG Weight in KGYuvraj GargNo ratings yet
- Alpha Blood Root Paste ResultsDocument5 pagesAlpha Blood Root Paste ResultsJeNo ratings yet
- JHA LiftingDocument4 pagesJHA Liftingsyamimi balkhisNo ratings yet
- Ms. MantillaDocument3 pagesMs. MantillaJames Elwood DoyolaNo ratings yet
- كتالوج الأجهزة الطبيةDocument8 pagesكتالوج الأجهزة الطبيةIslam HosniNo ratings yet
- Reduction of Implant Loading Using A Modified Centric Occlusal AnatomyDocument16 pagesReduction of Implant Loading Using A Modified Centric Occlusal AnatomyPablo Gutiérrez Da VeneziaNo ratings yet
- CryoStore Brochure Combined 2021Document7 pagesCryoStore Brochure Combined 2021srinivas PilliNo ratings yet
- Ahmar Metastasis Health JournalDocument9 pagesAhmar Metastasis Health JournalSyafaringga Dian oscarNo ratings yet
- Converting Intravenous Infusion To Saline LockDocument2 pagesConverting Intravenous Infusion To Saline LockRosehelle CamelloNo ratings yet
- Manajemen Pasien Dekstroskoliosis Berat Dengan Kegagalan Napas Yang Disebabkan Oleh Syok Septik Dan PneumoniaDocument8 pagesManajemen Pasien Dekstroskoliosis Berat Dengan Kegagalan Napas Yang Disebabkan Oleh Syok Septik Dan PneumoniaMachfud SidiqNo ratings yet
- Determination of LD and ED by Dose Response Relationship and Assessment of Toxicological and Non Toxicological Behaviour of Ipomoea HederaceaDocument3 pagesDetermination of LD and ED by Dose Response Relationship and Assessment of Toxicological and Non Toxicological Behaviour of Ipomoea HederaceaeyobNo ratings yet
- Visitor Health Declaration FormDocument1 pageVisitor Health Declaration FormHung Kwan1 KeungNo ratings yet
- Dasar Pengelolaan Penderita Gawat Darurat: Dept. Anestesiologi & Terapi Intensif FK-USU/RSUP H.Adam Malik-MedanDocument47 pagesDasar Pengelolaan Penderita Gawat Darurat: Dept. Anestesiologi & Terapi Intensif FK-USU/RSUP H.Adam Malik-Medanfibri fameliaNo ratings yet
- Electrikal TherapyDocument16 pagesElectrikal Therapyteluk_airNo ratings yet
- Patient Feedback QuestionnaireDocument2 pagesPatient Feedback QuestionnaireRanu AbhinavNo ratings yet
- Surgery & Allied Ortho, Ent, Ophthal & Anesthesia Topics by DR VishwaDocument7 pagesSurgery & Allied Ortho, Ent, Ophthal & Anesthesia Topics by DR Vishwaابو عبد الرحمنNo ratings yet
- Umbilical Hernia Repair in Conjunction With AbdominoplastyDocument2 pagesUmbilical Hernia Repair in Conjunction With AbdominoplastydoctorbanNo ratings yet
- Support, Replenish Protect The Stroke of A Brush: and WithDocument4 pagesSupport, Replenish Protect The Stroke of A Brush: and Withsmiledesigner_13No ratings yet
- Disaster NursingDocument3 pagesDisaster NursingAlkiana SalardaNo ratings yet
- The Nursing Role in Providing Comfort During Labor and BirthDocument18 pagesThe Nursing Role in Providing Comfort During Labor and Birthمريم حجيNo ratings yet
- EMS ResultDocument2 pagesEMS Resultsangamesh83107No ratings yet
- Dead Broke by Michelle StambaughDocument40 pagesDead Broke by Michelle Stambaughpratik patelNo ratings yet
- Phase 1 IntroDocument7 pagesPhase 1 Intro22024552 Hà Đăng LongNo ratings yet
- Seizure-NcpDocument2 pagesSeizure-NcpRomuel PaparonNo ratings yet
- Learning Activity Sheet in English 6: Quarter 4, Worksheet 1Document5 pagesLearning Activity Sheet in English 6: Quarter 4, Worksheet 1Janita AbergosNo ratings yet