You might also like
- Workbook GitDocument13 pagesWorkbook GitJohn Lyndon SayongNo ratings yet
- Normal Gastrointestinal Embryology: Intestinal MalrotationDocument159 pagesNormal Gastrointestinal Embryology: Intestinal MalrotationDaNy ChiriacNo ratings yet
- Chapter 15: The Gastrointestinal System: Multiple Choice. Choose The Correct AnswerDocument3 pagesChapter 15: The Gastrointestinal System: Multiple Choice. Choose The Correct Answerbilly100% (1)
- Obstruction. DidacticsDocument87 pagesObstruction. DidacticsJoher MendezNo ratings yet
- Sigmoid Volvulus: Rashid Swed S. (Md4) Mwanyingili John A. (Md3)Document46 pagesSigmoid Volvulus: Rashid Swed S. (Md4) Mwanyingili John A. (Md3)Amani Twaha MsemakweliNo ratings yet
- Gastrointestinal Tract PathologyDocument8 pagesGastrointestinal Tract PathologyMiguel Cuevas Dolot100% (2)
- Bedah Anak: Sign/mushroom Sign/caterpillar SignDocument2 pagesBedah Anak: Sign/mushroom Sign/caterpillar SignNyakdaraJunimarzaNo ratings yet
- Bowel ObstructionsDocument24 pagesBowel ObstructionsArchie ZhangNo ratings yet
- Developmental Anomalies of Gastrointestinal Tract: Dr. Dev LakheraDocument66 pagesDevelopmental Anomalies of Gastrointestinal Tract: Dr. Dev LakheraNatashaNo ratings yet
- Chapter 172. Gastroschisis/Omphalocele: Wanda A. Chin, MDDocument3 pagesChapter 172. Gastroschisis/Omphalocele: Wanda A. Chin, MDChrisNo ratings yet
- Radiology Examination For Tractus Digestivus Chairunnisa, Dr. SP - RadDocument100 pagesRadiology Examination For Tractus Digestivus Chairunnisa, Dr. SP - RadDiana OCtavinaNo ratings yet
- Emergencies in GITDocument7 pagesEmergencies in GITsssajiNo ratings yet
- 2.4.5.2.3.a Bowel ObstructionDocument35 pages2.4.5.2.3.a Bowel ObstructionProject ByNo ratings yet
- Gastrointestinal Tract PathologyDocument12 pagesGastrointestinal Tract PathologyTurinawe Bin ByensiNo ratings yet
- Deviriligo Notes 12Document99 pagesDeviriligo Notes 12A Fish100% (1)
- Surg - Malrotation With VolvulusDocument3 pagesSurg - Malrotation With VolvulusSuren SubramaniamNo ratings yet
- Presentacion GastrointestinalDocument228 pagesPresentacion GastrointestinalNb + XB = AVNo ratings yet
- Appendisitis: DR Bambang Sugeng Bag. Bedah FK UnissulaDocument33 pagesAppendisitis: DR Bambang Sugeng Bag. Bedah FK UnissulaEsthy Espanyola PelapelaponNo ratings yet
- The Acute Distended AbdomenDocument2 pagesThe Acute Distended AbdomenTom Mallinson100% (1)
- Congenital Development Disorder of Esophagus, Stomach, Duodenum, Abdomen Wall, Anus and RectumDocument56 pagesCongenital Development Disorder of Esophagus, Stomach, Duodenum, Abdomen Wall, Anus and RectumSarah Nabella PutriNo ratings yet
- Small Bowel: Alaa MaaliDocument78 pagesSmall Bowel: Alaa MaaliHalima AssiNo ratings yet
- Image Interpretation 4 (Autosaved) SssDocument169 pagesImage Interpretation 4 (Autosaved) SssifeanyiNo ratings yet
- ACUTE ABDOMEN by DR NajamDocument65 pagesACUTE ABDOMEN by DR NajamdasdasfNo ratings yet
- MiniOSCE Surgery 1Document329 pagesMiniOSCE Surgery 1Mohammad BanisalmanNo ratings yet
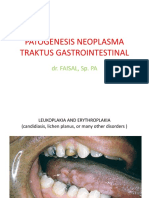
- Patogenesis Neoplasma Traktus Gastrointestinal: Dr. FAISAL, Sp. PADocument42 pagesPatogenesis Neoplasma Traktus Gastrointestinal: Dr. FAISAL, Sp. PAmitasushNo ratings yet
- Imaging of StomachDocument92 pagesImaging of StomachKN SharmaNo ratings yet
- EsophagusDocument4 pagesEsophagussildesireNo ratings yet
- Abdominal SignDocument85 pagesAbdominal Signnovitafitri123No ratings yet
- How To Read Chest Abdomen CT Scan X-RayDocument86 pagesHow To Read Chest Abdomen CT Scan X-RaymuhammadfyNo ratings yet
- Pediatric GI RadiologyDocument6 pagesPediatric GI Radiologysarguss14No ratings yet
- GIT Abnormality in Infant/Children On Radiology Imaging Which Need Surgery CorrectionDocument48 pagesGIT Abnormality in Infant/Children On Radiology Imaging Which Need Surgery Correctiondr fikriNo ratings yet
- Flow: When Obstruction - We Think High/Low Outlet Obstruction Complete/ Partial Mechanical or Functional (Ileus or Hirschprung)Document4 pagesFlow: When Obstruction - We Think High/Low Outlet Obstruction Complete/ Partial Mechanical or Functional (Ileus or Hirschprung)Youssry JaranillaNo ratings yet
- 155 - B3 Sesi 1 Asisten 2015Document91 pages155 - B3 Sesi 1 Asisten 2015Luthfi AnshoriNo ratings yet
- Dasar Dasar Radiologi Digestive Dan Nefrourinari1Document102 pagesDasar Dasar Radiologi Digestive Dan Nefrourinari1Mada Dwi Hari100% (1)
- OB POINTERS - Docx 1Document8 pagesOB POINTERS - Docx 1pinpindalgoNo ratings yet
- Acute Abdomen - AbiDocument21 pagesAcute Abdomen - AbiAbirami ShavaniNo ratings yet
- Curs Fetal Abdominal AnomaliesDocument137 pagesCurs Fetal Abdominal AnomaliesCristi SoareceNo ratings yet
- Small and Large Bowel Obstruction (1) - 1Document91 pagesSmall and Large Bowel Obstruction (1) - 1dagimb bekeleNo ratings yet
- Acute AppendicitisDocument5 pagesAcute AppendicitisPrasetya Ismail PermadiNo ratings yet
- Intestinal Obstruction in Pediatric PatientsDocument25 pagesIntestinal Obstruction in Pediatric PatientsHaryo Priambodo100% (1)
- Percussion of The Abdomen: Prof. R. Sukumar MD Institute of Internal Medicine MMC & GGHDocument25 pagesPercussion of The Abdomen: Prof. R. Sukumar MD Institute of Internal Medicine MMC & GGHVignesh Kumar ChandiraseharanNo ratings yet
- Patologia Chirurgicala A Apendicelui CecalDocument41 pagesPatologia Chirurgicala A Apendicelui CecalIrina DrewNo ratings yet
- Neonatal Billious VomitingDocument42 pagesNeonatal Billious Vomitinghayssam rashwan100% (1)
- RLQ PainDocument20 pagesRLQ PainBEATRICE SOPHIA PARMANo ratings yet
- Disorders of The IntestinesDocument64 pagesDisorders of The IntestinesCharmaine Torio PastorNo ratings yet
- Bowel OcclusionDocument4 pagesBowel OcclusionAndra BauerNo ratings yet
- Esophagus Anatomy, Physiology, and Diseases: Alan Chu March 13, 2013Document18 pagesEsophagus Anatomy, Physiology, and Diseases: Alan Chu March 13, 2013drNo ratings yet
- Esophagus Lecture Fatima NEW 2015Document31 pagesEsophagus Lecture Fatima NEW 2015Aileen EmyNo ratings yet
- (SURGPATH) 1.01 Gastrointestinal PathologyDocument20 pages(SURGPATH) 1.01 Gastrointestinal PathologyKarl ChavezNo ratings yet
- All FilesDocument35 pagesAll FilesHeena AmnaNo ratings yet
- Anatomy Atresia, Volvulus, Meckel's Diverticulum: BowelDocument45 pagesAnatomy Atresia, Volvulus, Meckel's Diverticulum: BowelkedokterankeluargaNo ratings yet
- Inguinal Hernia: Dr. Amar Rathod M.S. (Ayurved)Document18 pagesInguinal Hernia: Dr. Amar Rathod M.S. (Ayurved)GAURAV0% (1)
- PathologyDocument28 pagesPathologyninja-2001No ratings yet
- Gastrointestinal System DiseasesDocument6 pagesGastrointestinal System DiseasesHazel ConjeNo ratings yet
- Types and Management of Intestinal StomasDocument62 pagesTypes and Management of Intestinal Stomasminnalesri100% (6)
- College of Nursing Madurai Medical College Madurai-20Document23 pagesCollege of Nursing Madurai Medical College Madurai-20monishaNo ratings yet
- 14 - Barium Studies For GIT With NotesDocument50 pages14 - Barium Studies For GIT With NotesSunil ThomasNo ratings yet
- SURGERY Lecture 5 - Abdominal Wall, Omentum, Mesentery, Retroperitoneum (Dr. Wenceslao)Document13 pagesSURGERY Lecture 5 - Abdominal Wall, Omentum, Mesentery, Retroperitoneum (Dr. Wenceslao)Medisina101No ratings yet
- Pediatric SurgeryDocument167 pagesPediatric Surgerynanialex800No ratings yet
- Acute AbdomenDocument117 pagesAcute Abdomenayundaafdal100% (1)
- Osce AbdomenDocument33 pagesOsce AbdomenistiNo ratings yet
- Hemorrhoids and Anal ProblemsDocument64 pagesHemorrhoids and Anal ProblemsAhmed Noureldin Ahmed100% (4)
- IntussusceptionDocument4 pagesIntussusceptionlovethestarNo ratings yet
- Gastrointestinal Drugs 26269Document10 pagesGastrointestinal Drugs 26269Elena CondicNo ratings yet
- Cholestasis: Dr. Darmadi SPPD, FinasimDocument20 pagesCholestasis: Dr. Darmadi SPPD, FinasimTiens MonisaNo ratings yet
- Nursing Management OF Git Problems Gastric and Duodenal DisordersDocument109 pagesNursing Management OF Git Problems Gastric and Duodenal DisorderstantanbaragoNo ratings yet
- Diseases of The ColonDocument59 pagesDiseases of The ColonElvisNo ratings yet
- Quiz 1 Med Surg SummerDocument8 pagesQuiz 1 Med Surg SummerMc Harris VinasoyNo ratings yet
- @ (White Paper - Cut-Off) RS85 - S-Shearwave Imaging LiverDocument10 pages@ (White Paper - Cut-Off) RS85 - S-Shearwave Imaging LiverHajjab AnasNo ratings yet
- Module 2 (Disorders of The Git)Document3 pagesModule 2 (Disorders of The Git)Nur Fatima SanaaniNo ratings yet
- Diagnostic Tests A. Endoscopy: Nursing ConsiderationsDocument3 pagesDiagnostic Tests A. Endoscopy: Nursing ConsiderationsMae GabrielNo ratings yet
- Introduction To Gastrointestinal Tract (GIT) : Zheng Shihua The First Clinical Medical College Three Gorge UniversityDocument54 pagesIntroduction To Gastrointestinal Tract (GIT) : Zheng Shihua The First Clinical Medical College Three Gorge UniversityMadhu Sudhan PandeyaNo ratings yet
- Daftar Pustaka: Medicine. 7 Ed. Churchill Livingstone: EdinburgDocument3 pagesDaftar Pustaka: Medicine. 7 Ed. Churchill Livingstone: EdinburgseptinaNo ratings yet
- Stool Causes Associated Symptoms MelenaDocument2 pagesStool Causes Associated Symptoms Melenaadharra crystal dorinNo ratings yet
- Management of Patients With Gastro-Intestinal DisordersDocument84 pagesManagement of Patients With Gastro-Intestinal DisordersY. Beatrice AbigailNo ratings yet
- Bedside Nurse: Name of Student: Jela Mae V. Pates Score: - /25Document8 pagesBedside Nurse: Name of Student: Jela Mae V. Pates Score: - /25janna mae patriarcaNo ratings yet
- Pediatric Gastrointestinal DisordersDocument11 pagesPediatric Gastrointestinal DisordersANGELTHERESE CANDIANo ratings yet
- Terms and Strategies For Medical RecordsDocument42 pagesTerms and Strategies For Medical RecordsJesus ParragaNo ratings yet
- AFFERENT & EFFERENT SyndromeDocument12 pagesAFFERENT & EFFERENT SyndromeAli Sibra MulluziNo ratings yet
- 2a. Pathology of Gastric CancerDocument27 pages2a. Pathology of Gastric CancerWorku KifleNo ratings yet
- Abdominal Swelling - Insiders GuideDocument3 pagesAbdominal Swelling - Insiders GuideAbdul AkhtarNo ratings yet
- Daftar Pustaka - 4Document3 pagesDaftar Pustaka - 4PascaIKM STIKes KuninganNo ratings yet
- GastroenterologyDocument30 pagesGastroenterologyMohammad MohyeddienNo ratings yet
- Handbook Boli DigestiveDocument449 pagesHandbook Boli DigestiveAndreea Stănilă100% (2)
- Atlas of Sailvary Gland DiseaseDocument4 pagesAtlas of Sailvary Gland DiseaseMohammed FeroNo ratings yet
- Peraturan Bpjs Poli GigiDocument11 pagesPeraturan Bpjs Poli GigitarikusumaNo ratings yet
- Clinical Skills III: Gastrointestinal SystemDocument39 pagesClinical Skills III: Gastrointestinal Systemstella pangestikaNo ratings yet
- Gastritis. Ulcer DiseaseDocument60 pagesGastritis. Ulcer DiseaseShambhu AshokNo ratings yet
- Approach To The Infant or Child With Nausea and Vomiting - UpToDateDocument47 pagesApproach To The Infant or Child With Nausea and Vomiting - UpToDatemayteveronica1000No ratings yet