You might also like
- Mariblanca Statistics and ProbabilityDocument14 pagesMariblanca Statistics and ProbabilityArmin Diolosa100% (1)
- Module 04 - Part1 AssignmentDocument10 pagesModule 04 - Part1 Assignmentsuresh avadutha75% (4)
- Department of Education: 4 QUARTER - Module 1Document16 pagesDepartment of Education: 4 QUARTER - Module 1Martica CanlasNo ratings yet
- Mercertrs SamplecontentDocument27 pagesMercertrs Samplecontentönay akgünNo ratings yet
- LC1 BMI and All-Cause Mortality in Older AdultsDocument16 pagesLC1 BMI and All-Cause Mortality in Older AdultsMariNo ratings yet
- Artigo 12Document17 pagesArtigo 12daisyscholliersNo ratings yet
- Prediction of Body Fat in 12-Y-Old African American and White Children: Evaluation of MethodsDocument11 pagesPrediction of Body Fat in 12-Y-Old African American and White Children: Evaluation of MethodsErna MiraniNo ratings yet
- Accuracy of Body Mass Index Cutoffs For Classifying Obesity in Chilean Children and AdolescentsDocument9 pagesAccuracy of Body Mass Index Cutoffs For Classifying Obesity in Chilean Children and AdolescentsJaneth Milagros Cantoral MilianNo ratings yet
- Age, Sex and Ethnic Differences in The Prevalence of Underweight and Overweight, Defined by Using The CDC and IOTF Cut Points in Asian ChildrenDocument8 pagesAge, Sex and Ethnic Differences in The Prevalence of Underweight and Overweight, Defined by Using The CDC and IOTF Cut Points in Asian Childrenatleticar1No ratings yet
- Neck Circumference As An Indicator of Elevated Central Adiposity in ChildrenDocument7 pagesNeck Circumference As An Indicator of Elevated Central Adiposity in ChildrenpqrsehunNo ratings yet
- Jurnal 12Document6 pagesJurnal 12Audio TechnicaNo ratings yet
- Estimating Stunting From Underweight Survey DataDocument9 pagesEstimating Stunting From Underweight Survey DataangrainadillaNo ratings yet
- Cintas - Article OJPCH 4 116Document6 pagesCintas - Article OJPCH 4 116oscar echeverri cardonaNo ratings yet
- Association of Body Mass Index and Waist-To-Hip Ratio With Brain StructureDocument8 pagesAssociation of Body Mass Index and Waist-To-Hip Ratio With Brain StructureBesta Arum BelaNo ratings yet
- Body Mass Index and Body Composition Measures by Dual X-Ray Absorptiometry in Patients Aged 10 To 21 Years With Spinal Cord InjuryDocument8 pagesBody Mass Index and Body Composition Measures by Dual X-Ray Absorptiometry in Patients Aged 10 To 21 Years With Spinal Cord InjuryJoão Pedro PontesNo ratings yet
- cole2012IOTF STANDARDSDocument11 pagescole2012IOTF STANDARDSatleticar1No ratings yet
- BMC Public Health: The Validity of Self-Reported Weight in US Adults: A Population Based Cross-Sectional StudyDocument10 pagesBMC Public Health: The Validity of Self-Reported Weight in US Adults: A Population Based Cross-Sectional Studyteamfrio827No ratings yet
- Skim Fold Medical Students MalaysiaDocument7 pagesSkim Fold Medical Students MalaysiaKalesware MuniandyNo ratings yet
- Cole2000 PDFDocument6 pagesCole2000 PDFatleticar1No ratings yet
- Perception of Body Image As Indicator of Weight Status in The European UnionDocument10 pagesPerception of Body Image As Indicator of Weight Status in The European UnionJuanPauloMúneraRuedaNo ratings yet
- BAI Publicacion Original 2011Document7 pagesBAI Publicacion Original 2011gaby fernandezNo ratings yet
- Relative Fat Mass (RFM) As A New Estimator of Whole-Body Fat Percentage A Cross-Sectional Study in American Adult IndividualsDocument11 pagesRelative Fat Mass (RFM) As A New Estimator of Whole-Body Fat Percentage A Cross-Sectional Study in American Adult IndividualsLaura Hernandez SanchezNo ratings yet
- Journal Review Obesity, Adiposity, Physical Fitness and Activity Levels in Cree ChildrenDocument10 pagesJournal Review Obesity, Adiposity, Physical Fitness and Activity Levels in Cree ChildrendaniNo ratings yet
- Nutritional Assesment StatusDocument23 pagesNutritional Assesment StatusAbdisamed AllaaleNo ratings yet
- Measuring Body CompositionDocument6 pagesMeasuring Body CompositionKamruzzaman Manik100% (1)
- JAMA EEUU Prvalencia Obesidad InfantilDocument8 pagesJAMA EEUU Prvalencia Obesidad InfantilAnonymous 0iU1pPeQNo ratings yet
- MC Dowell 2008 NHSR 010Document46 pagesMC Dowell 2008 NHSR 010fgeafadaedNo ratings yet
- Mid-Upper Arm Circumference As An Indicator of UnderweightDocument7 pagesMid-Upper Arm Circumference As An Indicator of UnderweightgianellaNo ratings yet
- Obesity StudyDocument15 pagesObesity StudyBayAreaNewsGroupNo ratings yet
- Body Weight, Health, and Longevity: Medicine and Public IssuesDocument11 pagesBody Weight, Health, and Longevity: Medicine and Public IssuesDavid WheelerNo ratings yet
- Racial/Ethnic and Socioeconomic Status Differences in Overweight and Health-Related Behaviors Among American Students: National Trends 1986 - 2003Document10 pagesRacial/Ethnic and Socioeconomic Status Differences in Overweight and Health-Related Behaviors Among American Students: National Trends 1986 - 2003'fanny Quenhita'No ratings yet
- Measurement of Body Composition in Children - UpToDateDocument27 pagesMeasurement of Body Composition in Children - UpToDatemarina alvesNo ratings yet
- Measuring Obesity 2Document11 pagesMeasuring Obesity 2Maged AllamNo ratings yet
- 45 FullDocument18 pages45 FullDyah Ajeng PratiwiNo ratings yet
- Harrington 2012Document5 pagesHarrington 2012atleticar1No ratings yet
- Weight and Skin Colour As Predictors of Vitamin D Status: Results of An Epidemiological Investigation Using Nationally Representative DataDocument8 pagesWeight and Skin Colour As Predictors of Vitamin D Status: Results of An Epidemiological Investigation Using Nationally Representative Datatihemex618No ratings yet
- Anthropometric MeasurementDocument2 pagesAnthropometric MeasurementJames ClarkNo ratings yet
- Body Mass Index ObesityDocument8 pagesBody Mass Index ObesityReyes Falcon D. ÁngelNo ratings yet
- Comparacion de Criterios Sindrome MetabolicoDocument6 pagesComparacion de Criterios Sindrome Metabolicomichgirl90No ratings yet
- Gemeos Derma ToDocument6 pagesGemeos Derma ToFranco CastroNo ratings yet
- Overview of The CDC Growth Charts: CDC: Safer - Healthier - People 1Document25 pagesOverview of The CDC Growth Charts: CDC: Safer - Healthier - People 1Batako HayashiNo ratings yet
- Frisancho1984 1Document12 pagesFrisancho1984 1AdelaNo ratings yet
- Mult2 - Novas Ref Avaliação Curvas InfantilDocument16 pagesMult2 - Novas Ref Avaliação Curvas InfantilDanielle Raquel GonçalvesNo ratings yet
- Calf Circumference Cutoff Values From The NHANES 1999 A 2006Document9 pagesCalf Circumference Cutoff Values From The NHANES 1999 A 2006anthropometricaNo ratings yet
- Vit D Deficiency Cin Obesity Meta-AnalysisDocument7 pagesVit D Deficiency Cin Obesity Meta-AnalysisJade IreneNo ratings yet
- Highnam 2007Document16 pagesHighnam 2007Mario SansoneNo ratings yet
- s12877 019 1363 0Document8 pagess12877 019 1363 0besnier.analuciaNo ratings yet
- Santana 2019 - de Santana - Brasil - VAT y MortalidadDocument11 pagesSantana 2019 - de Santana - Brasil - VAT y Mortalidad2192036250No ratings yet
- Research Article: Gender Differences in The Association Between Sleep Duration and Body Composition: The Cardia StudyDocument8 pagesResearch Article: Gender Differences in The Association Between Sleep Duration and Body Composition: The Cardia StudyVistaa Vistoo AnasariNo ratings yet
- 24 1520325260 - 06-03-2018 PDFDocument9 pages24 1520325260 - 06-03-2018 PDFEditor IJRITCCNo ratings yet
- FONTAINE, K. R. Et Al.. Years of Life Lost Due To ObesityDocument7 pagesFONTAINE, K. R. Et Al.. Years of Life Lost Due To Obesityalline.valleNo ratings yet
- Worldwide Trends in Underweight and Obesity From 1990 To 2022Document24 pagesWorldwide Trends in Underweight and Obesity From 1990 To 2022luis sanchezNo ratings yet
- Standing Long Jump en Estudiantes ColombianosDocument22 pagesStanding Long Jump en Estudiantes Colombianosnatavidarte14No ratings yet
- A Composite Score Combining Waist Circumference and Body Mass Index More Accurately Predicts Body Fat Percentage in 6-To 13-Year-Old ChildrenDocument7 pagesA Composite Score Combining Waist Circumference and Body Mass Index More Accurately Predicts Body Fat Percentage in 6-To 13-Year-Old ChildrenThalia KarampasiNo ratings yet
- 1 s2.0 S0168822715000522 MainDocument8 pages1 s2.0 S0168822715000522 Maintri1994No ratings yet
- Nutritional Status and Its Relationship With Blood Pressure Among Children and Adolescents in South ChinaDocument7 pagesNutritional Status and Its Relationship With Blood Pressure Among Children and Adolescents in South ChinautarinuNo ratings yet
- Reliabilitas Pengukuran Inter Dan Intraobserver AntropometriDocument7 pagesReliabilitas Pengukuran Inter Dan Intraobserver AntropometriRifka Laily MafazaNo ratings yet
- 10 1038@ijo2008102Document7 pages10 1038@ijo2008102Thedy BarrosNo ratings yet
- Anthropometric Reference Data For International Use: Recommendations From A World Health Organization Expert Committee1"3Document9 pagesAnthropometric Reference Data For International Use: Recommendations From A World Health Organization Expert Committee1"3Yuga RahmadanaNo ratings yet
- Anthropometric Measurement To Identify Undernutrition in Cerabral PalsyDocument8 pagesAnthropometric Measurement To Identify Undernutrition in Cerabral PalsyPam Travezani MiyazakiNo ratings yet
- Application of Binary Logistic Regression Model To Assess The Likelihood of OverweightDocument8 pagesApplication of Binary Logistic Regression Model To Assess The Likelihood of OverweightNoora ShresthaNo ratings yet
- JCCM MS Id 000138Document7 pagesJCCM MS Id 000138chiquitaputriNo ratings yet
- Social Justice and the Urban Obesity Crisis: Implications for Social WorkFrom EverandSocial Justice and the Urban Obesity Crisis: Implications for Social WorkNo ratings yet
- A Consideration That Childhood Obesity Could Be Classified As Legalized Child AbuseFrom EverandA Consideration That Childhood Obesity Could Be Classified As Legalized Child AbuseNo ratings yet
- Projects and Project-Based Learning - What's The DifferenceDocument5 pagesProjects and Project-Based Learning - What's The DifferenceKalesware MuniandyNo ratings yet
- Acid and Alkali: 6.1 Properties of Acids and AlkalisDocument2 pagesAcid and Alkali: 6.1 Properties of Acids and AlkalisKalesware MuniandyNo ratings yet
- Ecosystem: 2.1 Energy Flow in An EcosystemDocument3 pagesEcosystem: 2.1 Energy Flow in An EcosystemKalesware MuniandyNo ratings yet
- Biodiversity: 1.1 Diversity of OrganismsDocument2 pagesBiodiversity: 1.1 Diversity of OrganismsKalesware MuniandyNo ratings yet
- Boyle's Law SimulationDocument2 pagesBoyle's Law SimulationKalesware MuniandyNo ratings yet
- 8226 18984 1 PBDocument9 pages8226 18984 1 PBKalesware MuniandyNo ratings yet
- 5E Instructional Model OnlineDocument13 pages5E Instructional Model OnlineKalesware MuniandyNo ratings yet
- Overview of Curriculum Change: A Brief Discussion: Nilay Mondal Dr. Arjun Chandra DasDocument6 pagesOverview of Curriculum Change: A Brief Discussion: Nilay Mondal Dr. Arjun Chandra DasKalesware MuniandyNo ratings yet
- MBAv1 PDFDocument171 pagesMBAv1 PDFRitik VermaNo ratings yet
- Scheme of Work SS2 3RD TermDocument2 pagesScheme of Work SS2 3RD TermangelNo ratings yet
- ES AssignmentDocument19 pagesES AssignmentLt. ShabanNo ratings yet
- Lesson Day 4Document9 pagesLesson Day 4Divine Jyrah H. VictorinoNo ratings yet
- Ex Simulare Monte Carlo - Ex Din ExcelDocument14 pagesEx Simulare Monte Carlo - Ex Din ExcelIulia TacheNo ratings yet
- (Math10-Q4-W3-Activity 3) Interpretation of Measures of PositionDocument2 pages(Math10-Q4-W3-Activity 3) Interpretation of Measures of PositionKathleen Minsalan ParazoNo ratings yet
- Professional Education - Let ReviewerDocument40 pagesProfessional Education - Let ReviewerAprillenNo ratings yet
- Disclosure To Promote The Right To InformationDocument14 pagesDisclosure To Promote The Right To InformationAbhey DograNo ratings yet
- Normal and Exponential Distribution: by Abhijeet SalunkeDocument21 pagesNormal and Exponential Distribution: by Abhijeet SalunkeAsh KNo ratings yet
- The SQLSSelf-report Quality of Life Measure For People With SchizophreniaDocument6 pagesThe SQLSSelf-report Quality of Life Measure For People With SchizophreniaWulandari AdindaNo ratings yet
- FOR 2nd Mid EditedDocument36 pagesFOR 2nd Mid EditedSP VetNo ratings yet
- Research PaperDocument6 pagesResearch PaperNegro, Gwyn SteffaniNo ratings yet
- Grade 10 Las 4 - Melc 2b - 4th QuarterDocument11 pagesGrade 10 Las 4 - Melc 2b - 4th Quarternorlie caneteNo ratings yet
- Central TendencyDocument26 pagesCentral Tendencyবিজয় সিকদারNo ratings yet
- Q4 A.S. Measures of Position For Grouped DataDocument9 pagesQ4 A.S. Measures of Position For Grouped Datasunshine batoyNo ratings yet
- Describing Data:: Displaying and Exploring DataDocument28 pagesDescribing Data:: Displaying and Exploring DataSougata Tikader FranchNo ratings yet
- Experiment 7Document5 pagesExperiment 7Hassan Raja khanNo ratings yet
- IE464 - T2 - Engineering Anthropometry and Workspace DesignDocument32 pagesIE464 - T2 - Engineering Anthropometry and Workspace DesignIbrahem Abdulrahman100% (2)
- A Semi-Detailed Lesson Plan in Teaching Percentiles For Grouped DataDocument7 pagesA Semi-Detailed Lesson Plan in Teaching Percentiles For Grouped DataJaymark AgsiNo ratings yet
- Assessment Let ReviewDocument154 pagesAssessment Let Reviewマイ ケ ルNo ratings yet
- CHAPTER 3 Statistical Description of DataDocument30 pagesCHAPTER 3 Statistical Description of DataLara FloresNo ratings yet
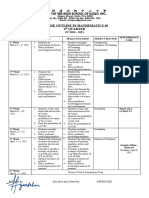
- Course Outline in Mathematics 10 4 Quarter: Dates Melc Skills Included Subject-Matter Performance Task 1 WeekDocument2 pagesCourse Outline in Mathematics 10 4 Quarter: Dates Melc Skills Included Subject-Matter Performance Task 1 WeekTiffany Joy Lencioco GambalanNo ratings yet
- Statistics For Business and Economics: Anderson Sweeney WilliamsDocument56 pagesStatistics For Business and Economics: Anderson Sweeney WilliamsDeepanjan SurNo ratings yet
- CHAPTER 3 Measure of Centeral TendencyDocument20 pagesCHAPTER 3 Measure of Centeral TendencyyonasNo ratings yet
- Asia Tech Salary Report 2024 (NodeFlair)Document82 pagesAsia Tech Salary Report 2024 (NodeFlair)Pierre TanNo ratings yet
- UMEP ModellingDocument18 pagesUMEP ModellingSyarif HidayatullahNo ratings yet