You might also like
- Case Presentation ManingasDocument7 pagesCase Presentation ManingasestimojervsNo ratings yet
- Verazon, Bsn3a-Myastenia NCPDocument5 pagesVerazon, Bsn3a-Myastenia NCPJaylord VerazonNo ratings yet
- The Art and Practice of Hypnotic Induction: Favorite Methods of Master Clinicians: Voices of Experience, #1From EverandThe Art and Practice of Hypnotic Induction: Favorite Methods of Master Clinicians: Voices of Experience, #1Rating: 5 out of 5 stars5/5 (1)
- Ncp-Drug StudyDocument2 pagesNcp-Drug StudyMark oliver GonzalesNo ratings yet
- Assessment Subjective: "Apat Na Araw Na SiyangDocument2 pagesAssessment Subjective: "Apat Na Araw Na Siyangmarlon_taycoNo ratings yet
- NCPDocument3 pagesNCPMichael TokongNo ratings yet
- Nursing Care Plan: Cues Nursing Diagnosis Rationale Specific Objective Interventions Rationale EvaluationDocument2 pagesNursing Care Plan: Cues Nursing Diagnosis Rationale Specific Objective Interventions Rationale Evaluation22 - Fernandez, Lyza Mae D.No ratings yet
- Final Thyroid Storm NCPDocument6 pagesFinal Thyroid Storm NCPoguitekim1No ratings yet
- Ncp3 CunananDocument2 pagesNcp3 CunananAbbyNo ratings yet
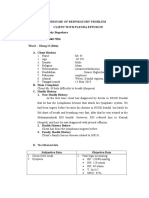
- Resume of Respiratory ProblemDocument5 pagesResume of Respiratory ProblemIbi Yulia SetyaniNo ratings yet
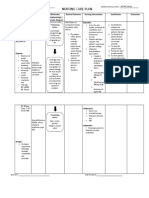
- NCP-Bronchial Asthma Without EvalDocument2 pagesNCP-Bronchial Asthma Without EvalTrisha Lapid MatulaNo ratings yet
- Drug StudyDocument5 pagesDrug Studyboxed juiceNo ratings yet
- APOLONIO, Reyjan L. (NCP 1)Document2 pagesAPOLONIO, Reyjan L. (NCP 1)REYJAN APOLONIONo ratings yet
- CORPUZ QQQDocument3 pagesCORPUZ QQQRomm JacobNo ratings yet
- Nursing Care Plan: Assessment Diagnosis Goal Planning Interventions Rationale Evaluations Subjective Data: "I HaveDocument9 pagesNursing Care Plan: Assessment Diagnosis Goal Planning Interventions Rationale Evaluations Subjective Data: "I HaveRicha AcharyaNo ratings yet
- Ventolin DrugstudyDocument1 pageVentolin DrugstudyMsOrangeNo ratings yet
- Materi Nursing Care PlanDocument1 pageMateri Nursing Care PlanSiti nur Kholifatus samsiyahNo ratings yet
- Nursing Care Plan Assessment Diagnosis Outcome Intervention Rationale EvaluationDocument5 pagesNursing Care Plan Assessment Diagnosis Outcome Intervention Rationale EvaluationMarivic Yuson MalagarNo ratings yet
- Nursing Care Plan: Assessment Nursing Diagnosis Nursing Analysis Planning Nursing Interventions Rationale EvaluationDocument4 pagesNursing Care Plan: Assessment Nursing Diagnosis Nursing Analysis Planning Nursing Interventions Rationale EvaluationElla EvangelistaNo ratings yet
- Lrti Case Drug StudyDocument6 pagesLrti Case Drug Studyn_I_K_K_I02No ratings yet
- Name: L.J.A AGE: 20 Years Old SEX: Male CC: Cough and DOB Admitting/Working Diagnosis: AsthmaDocument2 pagesName: L.J.A AGE: 20 Years Old SEX: Male CC: Cough and DOB Admitting/Working Diagnosis: AsthmaMae Therese B. MAGNONo ratings yet
- NCP Ineffective Breathing ActualDocument3 pagesNCP Ineffective Breathing ActualArian May Marcos100% (1)
- Ineffective Breathing PatternDocument3 pagesIneffective Breathing PatternReichelle Perlas62% (13)
- Assessment Diagnosis Planning Intervention Rationale EvaluationDocument2 pagesAssessment Diagnosis Planning Intervention Rationale EvaluationJustine Mae A. LoriaNo ratings yet
- Intravenous AnesthesiaDocument6 pagesIntravenous AnesthesiaBarda GulanNo ratings yet
- Community Acquired Pneumonia Nursing Care Plan: Demonstrate Pursed-Lip and Diaphragmatic Breathing To The PatientDocument4 pagesCommunity Acquired Pneumonia Nursing Care Plan: Demonstrate Pursed-Lip and Diaphragmatic Breathing To The PatientKrisianne Mae Lorenzo Francisco100% (1)
- Requirement in NCM 312: Presented By: Chloie Marie C. Rosalejos Submitted To: Ma. Lynn C. ParambitaDocument7 pagesRequirement in NCM 312: Presented By: Chloie Marie C. Rosalejos Submitted To: Ma. Lynn C. ParambitaChloie Marie RosalejosNo ratings yet
- Nursing Care Plan: Congestive Heart Failure-Deep Vein ThrombosisDocument19 pagesNursing Care Plan: Congestive Heart Failure-Deep Vein ThrombosisRiza Angela BarazanNo ratings yet
- Dnrle Covid NCPDocument3 pagesDnrle Covid NCPEna RodasNo ratings yet
- Romero, Deinielle Ingrid M. (Pulmo)Document3 pagesRomero, Deinielle Ingrid M. (Pulmo)Deinielle Magdangal RomeroNo ratings yet
- Subjective: IndependentDocument2 pagesSubjective: IndependentRea LynNo ratings yet
- Drug StudyDocument17 pagesDrug StudyJhucyl Mae GalvezNo ratings yet
- The Nursing Process FormatDocument11 pagesThe Nursing Process FormatMichelle Gee MagdaleNo ratings yet
- Assessment Nursing Diagnossis Scientific Basis Goal Nursing Intervention Rationale Evaluation IndependentDocument10 pagesAssessment Nursing Diagnossis Scientific Basis Goal Nursing Intervention Rationale Evaluation IndependentPamela laquindanumNo ratings yet
- College of Nursing: Cebu Normal UniversityDocument5 pagesCollege of Nursing: Cebu Normal UniversityChelsea WuNo ratings yet
- GROUP-3 (BSN 1K - Asynchronous Activity-Case Application For NCP MakingDocument3 pagesGROUP-3 (BSN 1K - Asynchronous Activity-Case Application For NCP MakingBeatrice Adrianne RanarioNo ratings yet
- Ineffectuve Breathign PatternDocument2 pagesIneffectuve Breathign PatternDiana Marie Magango FranciaNo ratings yet
- Drug Study: Propofol: CNS Depressants: AdditiveDocument5 pagesDrug Study: Propofol: CNS Depressants: AdditiveShara Lailanie A. AzisNo ratings yet
- NCP For Medical WardDocument5 pagesNCP For Medical WardJoyce Remo Zarate100% (2)
- SleepScience Vol5 Issue04 Art07Document4 pagesSleepScience Vol5 Issue04 Art07locoproanimalNo ratings yet
- NAME: Kristyn Joy D. Atangen DATE: Oct. 7, 2019: Subjective: DXDocument2 pagesNAME: Kristyn Joy D. Atangen DATE: Oct. 7, 2019: Subjective: DXTyn TynNo ratings yet
- Salbutamol Drug SummDocument1 pageSalbutamol Drug SummWarren100% (2)
- Student NurseDocument2 pagesStudent NurseTAYABAN, KENNETH JAKE, Q.No ratings yet
- Albuterol SalbutamolDocument2 pagesAlbuterol SalbutamolPePpER29No ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanRachelleNo ratings yet
- Problem 3Document2 pagesProblem 3Janah PagayNo ratings yet
- DANDY PUTRA SURYA (2014901056) - NCP Ineffective Breathing PatternDocument10 pagesDANDY PUTRA SURYA (2014901056) - NCP Ineffective Breathing PatternAlri LestariNo ratings yet
- EpiglDocument2 pagesEpiglfifiNo ratings yet
- Nursing Care PlanDocument7 pagesNursing Care Planmcd7r883% (6)
- Case Presentaion Pe (FinalDocument29 pagesCase Presentaion Pe (FinalFatema AkhterNo ratings yet
- Final Na Jud Ni As In!Document19 pagesFinal Na Jud Ni As In!joyrena ochondraNo ratings yet
- Nursing Care PlanDocument3 pagesNursing Care PlanShania Erika EnajeNo ratings yet
- Careplan 1Document11 pagesCareplan 1ligaba1559No ratings yet
- Nursing Care Plan: Lopez, Maria Sofia B. 9/29/2020 3-BSN-B Prof. ZoletaDocument5 pagesNursing Care Plan: Lopez, Maria Sofia B. 9/29/2020 3-BSN-B Prof. ZoletaSofiaLopezNo ratings yet
- Work On The Following QuestionsDocument7 pagesWork On The Following QuestionsCenn Dela RosaNo ratings yet
- RESPIRATORYDocument44 pagesRESPIRATORYJannele BernadasNo ratings yet
- NCP For CAP TB.Document5 pagesNCP For CAP TB.Cherry Ann BalagotNo ratings yet
- Scientific Writing and Peer Review Assignment 3 RubricDocument4 pagesScientific Writing and Peer Review Assignment 3 RubricKainatNo ratings yet
- Human Physiology Lab: Practicing Peer Review ExampleDocument3 pagesHuman Physiology Lab: Practicing Peer Review ExampleKainatNo ratings yet
- Case Management Supervision and Clinical Skills Supervision-ReflectionDocument10 pagesCase Management Supervision and Clinical Skills Supervision-ReflectionKainatNo ratings yet
- CPM Matrix For UBERDocument1 pageCPM Matrix For UBERKainatNo ratings yet
- Module 3 Reflective Essay GuidanceDocument10 pagesModule 3 Reflective Essay GuidanceKainatNo ratings yet
- Dissertation - QuestionnaireDocument5 pagesDissertation - QuestionnaireKainatNo ratings yet
- Working in The Steel Industry: Fact SheetDocument2 pagesWorking in The Steel Industry: Fact SheetKainatNo ratings yet
- Instructions 1Document1 pageInstructions 1KainatNo ratings yet
- Accommodating Passengers With Disabilities in AviationDocument3 pagesAccommodating Passengers With Disabilities in AviationKainatNo ratings yet
- Order ID 370530681: General MetricsDocument25 pagesOrder ID 370530681: General MetricsKainatNo ratings yet
- Group 6-BUSM1215 Assignment2 Part A-1Document15 pagesGroup 6-BUSM1215 Assignment2 Part A-1KainatNo ratings yet
- Philtech Institute of Arts and Technology Inc. Subject: Event Management Services Week 6 LESSON 6: Risk Management Learning OutcomesDocument9 pagesPhiltech Institute of Arts and Technology Inc. Subject: Event Management Services Week 6 LESSON 6: Risk Management Learning OutcomesMelissa Formento LustadoNo ratings yet
- 6125 EydfDocument1 page6125 Eydfjbethge01No ratings yet
- Land Surface Temp and Disease - PPTDocument28 pagesLand Surface Temp and Disease - PPTGOSPEL FACTORYNo ratings yet
- 4500-LSS Combined Handbook 2.2Document76 pages4500-LSS Combined Handbook 2.2Nguyễn Văn TrungNo ratings yet
- High Yield PediatricsDocument78 pagesHigh Yield Pediatricsjose100% (1)
- 27 34Document8 pages27 34Mohammad LavasaniNo ratings yet
- ANT341 Presentation 7Document2 pagesANT341 Presentation 7Dan Gideon CariagaNo ratings yet
- Haramase Simulator Achievement GuideDocument3 pagesHaramase Simulator Achievement GuideRisdiansyah 08633% (9)
- 2 Infectious Disease EpidemiologyDocument62 pages2 Infectious Disease Epidemiologykindness jawoNo ratings yet
- Final SPMCWaiverfortraineesandaffiliatesDocument3 pagesFinal SPMCWaiverfortraineesandaffiliatesSuzanne AndresNo ratings yet
- A Case Study of Intercontinental Bank PLC On MotivationDocument63 pagesA Case Study of Intercontinental Bank PLC On MotivationNnorom Goodluck KelechiNo ratings yet
- Unit 6-Develop and Implement Proactive Monitoring Systems For Health and Safety RGDocument13 pagesUnit 6-Develop and Implement Proactive Monitoring Systems For Health and Safety RGAshraf EL WardajiNo ratings yet
- Pokemon - Pearl Version - Manual - NDS PDFDocument32 pagesPokemon - Pearl Version - Manual - NDS PDFpika chuNo ratings yet
- Fall 08 MC Newsletter Research Microscopy & Histology CoreDocument4 pagesFall 08 MC Newsletter Research Microscopy & Histology CoreslusompedsNo ratings yet
- Social Studies SbaDocument20 pagesSocial Studies SbaAjay SinghNo ratings yet
- Taxation ProjectDocument23 pagesTaxation ProjectAkshata MasurkarNo ratings yet
- An Elementary School Classroom in A Slum NotesDocument8 pagesAn Elementary School Classroom in A Slum NotesSunilDwivediNo ratings yet
- IMO 884 TowingDocument15 pagesIMO 884 TowingPrasanna Kumar Kollala100% (3)
- Manufactouring Agreement Semiconductors Template - 1Document21 pagesManufactouring Agreement Semiconductors Template - 1David Jay MorNo ratings yet
- Consumer Guide To Medicaid PlanningDocument28 pagesConsumer Guide To Medicaid PlanningChristine NohNo ratings yet
- Cement Mill ReportDocument13 pagesCement Mill ReportYhaneNo ratings yet
- Itc Maurya: (Luxury Hotel Collection)Document31 pagesItc Maurya: (Luxury Hotel Collection)Gopi KrishnaNo ratings yet
- 3 Agricultural PestDocument10 pages3 Agricultural Pest137 - ShubhamNo ratings yet
- Bailey CH 7 81-120Document82 pagesBailey CH 7 81-120melaniaNo ratings yet
- NURS FPX 6210 Assessment 3 Strategic Visioning With StakeholdersDocument5 pagesNURS FPX 6210 Assessment 3 Strategic Visioning With Stakeholdersfarwaamjad771No ratings yet
- Aerosoft Airbus X Extended - Normal ProceduresDocument26 pagesAerosoft Airbus X Extended - Normal Proceduresluka40No ratings yet
- Arya Petroleum International (API) Located in Harmriya Free Zone-UAEDocument2 pagesArya Petroleum International (API) Located in Harmriya Free Zone-UAEKaushal SutariaNo ratings yet
- The Priming Effect of Family Obligation On Filipino Students Academic PerformanceDocument15 pagesThe Priming Effect of Family Obligation On Filipino Students Academic PerformancepauNo ratings yet
- Exploring The Nexus Between Nutrition and Academic Performance in Secondary Education A Case Study in Nyarushanje Sub County, Rukungiri DistrictDocument12 pagesExploring The Nexus Between Nutrition and Academic Performance in Secondary Education A Case Study in Nyarushanje Sub County, Rukungiri DistrictKIU PUBLICATION AND EXTENSIONNo ratings yet
- Oleh World Health Organization - 2009 - 11 Jan 2007 - : Dirujuk 560 Kali Artikel TerkaitDocument3 pagesOleh World Health Organization - 2009 - 11 Jan 2007 - : Dirujuk 560 Kali Artikel TerkaitDado ArmawanNo ratings yet