You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- (Doi 10.1002 - 14356007.a06 - 565.pub2) Liu, Gordon Y. T. - Ullmann's Encyclopedia of Industrial Chemistry - ChlorohydrinsDocument25 pages(Doi 10.1002 - 14356007.a06 - 565.pub2) Liu, Gordon Y. T. - Ullmann's Encyclopedia of Industrial Chemistry - ChlorohydrinsWidya Isti AriantiNo ratings yet
- The Spreader Flap in Primary Rhinoplasty: BackgroundDocument8 pagesThe Spreader Flap in Primary Rhinoplasty: BackgroundAlex Rolando SuntaxiNo ratings yet
- Psychosocial Characteristics of Young PDFDocument8 pagesPsychosocial Characteristics of Young PDFAlex Rolando SuntaxiNo ratings yet
- Reflections On Aesthetic Fac Ial Surger y in Men: Ross A. Clevens,, Stephen PrendivilleDocument12 pagesReflections On Aesthetic Fac Ial Surger y in Men: Ross A. Clevens,, Stephen PrendivilleAlex Rolando SuntaxiNo ratings yet
- Facial Treatment Preferences Among Aesthetically.5 PDFDocument9 pagesFacial Treatment Preferences Among Aesthetically.5 PDFAlex Rolando SuntaxiNo ratings yet
- Reflections On Aesthetic Fac Ial Surger y in Men: Ross A. Clevens,, Stephen PrendivilleDocument12 pagesReflections On Aesthetic Fac Ial Surger y in Men: Ross A. Clevens,, Stephen PrendivilleAlex Rolando SuntaxiNo ratings yet
- Code - 2216 - Congenital EventrationDocument5 pagesCode - 2216 - Congenital EventrationHumaida Hasan SamiraNo ratings yet
- Jan 2018 P1CDocument15 pagesJan 2018 P1CThant Hayman ThwayNo ratings yet
- Review Test Acids, Bases & Buffers1Document9 pagesReview Test Acids, Bases & Buffers1Kristina Moira ArenasNo ratings yet
- L&T INFOTECHDocument15 pagesL&T INFOTECHKshama NikhadeNo ratings yet
- Erp SSTDocument32 pagesErp SSTAzmi Nurse OfficialNo ratings yet
- Amine Sweetening UnitDocument3 pagesAmine Sweetening Unit1122goodNo ratings yet
- 04 P006 12786Document8 pages04 P006 12786bijoy82No ratings yet
- GC-MS Analysis of Ethyl Acetate Extract of Sterptomyces Species Isolated From VermicastDocument5 pagesGC-MS Analysis of Ethyl Acetate Extract of Sterptomyces Species Isolated From Vermicastvikram krishnaNo ratings yet
- RehabilitationDocument1 pageRehabilitationEbru SayılganNo ratings yet
- Characterising Forages For Ruminant FeedingDocument9 pagesCharacterising Forages For Ruminant FeedingClaudia SossaNo ratings yet
- Answer To Exam 3A-2020Document7 pagesAnswer To Exam 3A-2020Phạm Thái HàNo ratings yet
- E14F05P09Document6 pagesE14F05P09Víctor RomeuNo ratings yet
- Ama Computer Learning Center Malolos: Evaluation SheetDocument1 pageAma Computer Learning Center Malolos: Evaluation Sheetrenzo ronquilloNo ratings yet
- Muscle Structure and Functions of The Muscular SystemDocument4 pagesMuscle Structure and Functions of The Muscular SystemscadmoreNo ratings yet
- 1st Mock P1 EnglishDocument18 pages1st Mock P1 EnglishIshan RiveraNo ratings yet
- Iit Scrap JeeDocument1 pageIit Scrap Jeevenu MNo ratings yet
- Form No. 16: Details of Salary Paid and Any Other Income and Tax DeductedDocument2 pagesForm No. 16: Details of Salary Paid and Any Other Income and Tax DeductedSundaresan ChockalingamNo ratings yet
- PPT Skenario A - G6 - Blok 14Document66 pagesPPT Skenario A - G6 - Blok 14Ellysa CarolinnNo ratings yet
- 20BABBA342 Applied PsychologyDocument8 pages20BABBA342 Applied PsychologyBeatking HarshilNo ratings yet
- GD380A-L ListDocument6 pagesGD380A-L ListNam Won HongNo ratings yet
- Worksheet 4 On Transportation (Circulatory System)Document2 pagesWorksheet 4 On Transportation (Circulatory System)Naruto UzumakiNo ratings yet
- Wilo Water PumpDocument16 pagesWilo Water PumpThit SarNo ratings yet
- Crystal Healing Power PDFDocument36 pagesCrystal Healing Power PDFrkamundimuNo ratings yet
- Asian Culture Brief PhilippinesDocument4 pagesAsian Culture Brief PhilippinesMuizuriNo ratings yet
- 1st Set Crim LawDocument20 pages1st Set Crim Lawconnie1joy1alarca1omNo ratings yet
- Oncology McqsDocument115 pagesOncology McqsSyed NoorNo ratings yet
- Astm E571 - 12Document5 pagesAstm E571 - 12maxpan max100% (2)
- Keselamatan Semasa Mengisi Petrol Di Stesyen MinyakDocument24 pagesKeselamatan Semasa Mengisi Petrol Di Stesyen Minyakraymond cheanNo ratings yet
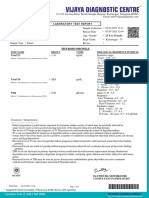
- Thyroid Profile: Laboratory Test ReportDocument1 pageThyroid Profile: Laboratory Test ReportArunsai Gilla100% (1)