You might also like
- HAARP PatentDocument12 pagesHAARP PatentGordon DuffNo ratings yet
- Hiller Rotor Cycle InfoDocument17 pagesHiller Rotor Cycle Infomjs6029100% (1)
- CBC ReportDocument1 pageCBC ReportKamal DeepNo ratings yet
- Laboratory Test Report: Mrs. V Valli Kumari 81 Years FemaleDocument2 pagesLaboratory Test Report: Mrs. V Valli Kumari 81 Years FemaleumaNo ratings yet
- PILE Foundation Analysis - ASCE William Saul-1980 - SearchableDocument22 pagesPILE Foundation Analysis - ASCE William Saul-1980 - Searchablev100% (1)
- Tec. Qx. Russell Taylor HumeralDocument32 pagesTec. Qx. Russell Taylor HumeralAlvaro_086No ratings yet
- Determination of Intravascular Volume Status byDocument6 pagesDetermination of Intravascular Volume Status bymalisalukmanNo ratings yet
- Source Dyuver: R. G. HumphreyDocument4 pagesSource Dyuver: R. G. HumphreydrivinerNo ratings yet
- Natural Frequencies of Toroidal TanksDocument27 pagesNatural Frequencies of Toroidal TanksHCStepNo ratings yet
- Instant Lit TheoryDocument1 pageInstant Lit TheoryHolt ParkerNo ratings yet
- Calphysics Institute - Introduction To Zero-Point EnergyDocument9 pagesCalphysics Institute - Introduction To Zero-Point EnergyPeter FrankNo ratings yet
- Paper - Yoan Elfina Litani REVISI2Document8 pagesPaper - Yoan Elfina Litani REVISI2MellaNo ratings yet
- United States Patent (191: Crowder (11) Patent Number: (45) Date of PatentDocument5 pagesUnited States Patent (191: Crowder (11) Patent Number: (45) Date of Patentgtr56No ratings yet
- Us 3995557Document6 pagesUs 3995557drive2345No ratings yet
- Post Fcps Fellowship Options For Radiology Residents: Resident'S SectionDocument4 pagesPost Fcps Fellowship Options For Radiology Residents: Resident'S SectionAkhtar AbbasNo ratings yet
- 黃土高原地區土壤可蝕性及其應用研究Document9 pages黃土高原地區土壤可蝕性及其應用研究.................100% (1)
- Nasa Ntrs Archive 19930094567Document13 pagesNasa Ntrs Archive 19930094567Mikail AviciNo ratings yet
- Pont S Index and Dental Arch FormDocument6 pagesPont S Index and Dental Arch FormMafe SalazarNo ratings yet
- Hydrocarbonate Reservoir Characterization Constrained To 3D Seismic AttributesDocument10 pagesHydrocarbonate Reservoir Characterization Constrained To 3D Seismic AttributesseanmohdNo ratings yet
- A Simple Model of Space Radiation Damage in GaAs Solar CellsDocument33 pagesA Simple Model of Space Radiation Damage in GaAs Solar CellsijgoiesfefNo ratings yet
- L09 - Annale UDJG 2006 Fascicula VDocument6 pagesL09 - Annale UDJG 2006 Fascicula VCarlos ArenasNo ratings yet
- United States Patent (191: Bieniosek (45) Date of Patent: May 23, 1989Document4 pagesUnited States Patent (191: Bieniosek (45) Date of Patent: May 23, 1989harishkumarsinghNo ratings yet
- ISRM-4CONGRESS-1979-032 - The Residual Shear Strength of Filled Joints in RockDocument8 pagesISRM-4CONGRESS-1979-032 - The Residual Shear Strength of Filled Joints in Rockcastille1956No ratings yet
- JF STEFFE Rheology Book Resumen 2019Document364 pagesJF STEFFE Rheology Book Resumen 2019Centzon TotochtinNo ratings yet
- C3-And CR3-dependent Microglial Clearance Protects Photoreceptors in Retinitis PigmentosaDocument19 pagesC3-And CR3-dependent Microglial Clearance Protects Photoreceptors in Retinitis PigmentosaZulkarnainNo ratings yet
- Microgrid 3Document11 pagesMicrogrid 3Bijay PrasadNo ratings yet
- Roane, James B. - The Balanced Force Concept, JOE, 11, 5, May 1985Document9 pagesRoane, James B. - The Balanced Force Concept, JOE, 11, 5, May 1985Härôld BäthôryNo ratings yet
- OF Shell: CardsDocument45 pagesOF Shell: CardsscribdNo ratings yet
- WPC 096853Document7 pagesWPC 096853omboNo ratings yet
- United States Patent (191: (11) Patent Number: (45) Date of PatentDocument5 pagesUnited States Patent (191: (11) Patent Number: (45) Date of PatentSalmanPashaNo ratings yet
- The Frequency of Respiratory Failure in Patients With Morbid Obesity Undergoing Gastric BypassDocument6 pagesThe Frequency of Respiratory Failure in Patients With Morbid Obesity Undergoing Gastric BypassLuis AlcalaNo ratings yet
- Artificial Hand Using Embedded SystemDocument8 pagesArtificial Hand Using Embedded SystemSK Sayeed Sid0% (3)
- GreatDocument17 pagesGreatTarunNo ratings yet
- US DOE Solar Powered Satellite - Military Implications - 1978Document46 pagesUS DOE Solar Powered Satellite - Military Implications - 1978Jim Lee100% (1)
- Studies of The Motion of The Brain at A Suddenly Applied Rotation of The SkullDocument8 pagesStudies of The Motion of The Brain at A Suddenly Applied Rotation of The SkullDeepsNo ratings yet
- United States Patent (19) : Gray, SRDocument7 pagesUnited States Patent (19) : Gray, SRMary AndersonNo ratings yet
- CDC 56275 DS1Document3 pagesCDC 56275 DS1Mika MonzNo ratings yet
- Mecanizáció Aerod.Document184 pagesMecanizáció Aerod.babusa70No ratings yet
- Power Generation App. of NanofluidsDocument16 pagesPower Generation App. of NanofluidsNavraj SinghNo ratings yet
- Effect of Finishing On The in Vivo Wear Rate of A Posterior Composite ResinDocument3 pagesEffect of Finishing On The in Vivo Wear Rate of A Posterior Composite ResinNaoki MezarinaNo ratings yet
- Alt-O. : Indlvlduelly /@Document7 pagesAlt-O. : Indlvlduelly /@drivinerNo ratings yet
- Deconvolution Technique Application To Spectral Contour AnalysisDocument12 pagesDeconvolution Technique Application To Spectral Contour AnalysisYassine ZidNo ratings yet
- Deconvolution Technique Application To Spectral Contour AnalysisDocument12 pagesDeconvolution Technique Application To Spectral Contour AnalysisYassine ZidNo ratings yet
- Deconvolution Technique Application To Spectral Contour AnalysisDocument12 pagesDeconvolution Technique Application To Spectral Contour AnalysisYassine ZidNo ratings yet
- High Intensity Ultrasonic GeneratorDocument10 pagesHigh Intensity Ultrasonic GeneratorHai NguyenNo ratings yet
- Aspek Non Teknis Dalam Keberhasilan Perawatan Dengan Gigi Tiruan LengkapDocument6 pagesAspek Non Teknis Dalam Keberhasilan Perawatan Dengan Gigi Tiruan LengkapHamba AllahNo ratings yet
- To ToDocument4 pagesTo Toamitgh88No ratings yet
- United States Patent: MinetDocument7 pagesUnited States Patent: Minetkees321No ratings yet
- 1.5 Constitutive Laws For Soils From A Physical ViewpointDocument51 pages1.5 Constitutive Laws For Soils From A Physical ViewpointMinhLêNo ratings yet
- Silla ConvertibleDocument4 pagesSilla Convertibleingeniomeca8800No ratings yet
- Vol. 3, No.: Ieee OnDocument8 pagesVol. 3, No.: Ieee OnLndr VldNo ratings yet
- United States Patent (191: Moriya Et A1Document8 pagesUnited States Patent (191: Moriya Et A1a5216730No ratings yet
- (Plate Ut Check Procedure (For Lamination Check) - 1Document6 pages(Plate Ut Check Procedure (For Lamination Check) - 1Deepan RajNo ratings yet
- 2006 GS5 CaneDocument5 pages2006 GS5 CaneRafael CarmoNo ratings yet
- Gambaran Maturasi Tulang Karpal Dan Servikal Pada Pasien Ortodontt Usia 9 - 18 TAHUN (Studi Foto Karpal Dan Sefalometri)Document8 pagesGambaran Maturasi Tulang Karpal Dan Servikal Pada Pasien Ortodontt Usia 9 - 18 TAHUN (Studi Foto Karpal Dan Sefalometri)fezia TiffaniNo ratings yet
- The Capacity Design of Reinforced Concrete Hybrid Structures For Multistorey Buildings T. Paulay and W. J. GoodsirDocument17 pagesThe Capacity Design of Reinforced Concrete Hybrid Structures For Multistorey Buildings T. Paulay and W. J. GoodsirFrankie ChanNo ratings yet
- Application of Ar and VR in HealthcareDocument19 pagesApplication of Ar and VR in HealthcareRushaliNo ratings yet
- Valve Maintenance and Repair Training CourseDocument3 pagesValve Maintenance and Repair Training CourseHayderr HassNo ratings yet
- Generator: United States Patent (191Document11 pagesGenerator: United States Patent (191Niki MikiNo ratings yet
- Colloquium Spectroscopicum Internationale: Plenary Lectures Presented at the XVIII Colloquium Spectroscopicum International, Grenoble, France, 15 - 19 September 1975From EverandColloquium Spectroscopicum Internationale: Plenary Lectures Presented at the XVIII Colloquium Spectroscopicum International, Grenoble, France, 15 - 19 September 1975J. P. RobinNo ratings yet
- Seismic Migration: Imaging of Acoustic Energy by Wave Field ExtrapolationFrom EverandSeismic Migration: Imaging of Acoustic Energy by Wave Field ExtrapolationNo ratings yet
- Lab Flow SheetDocument2 pagesLab Flow SheetRyan LazatinNo ratings yet
- New Health Care Clinical: Laboratory SrinagarDocument1 pageNew Health Care Clinical: Laboratory SrinagarRajaNo ratings yet
- Loa HPD - Mrs. Agnes M. VivasDocument1 pageLoa HPD - Mrs. Agnes M. VivasChariece PamatianNo ratings yet
- QC ALAT ELEKTROLITDocument4 pagesQC ALAT ELEKTROLITlaboratorium rsud jatipadangNo ratings yet
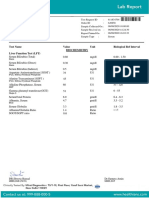
- Liver Function Test (LFT) Test Name Observed Values Units Biological Reference IntervalsDocument1 pageLiver Function Test (LFT) Test Name Observed Values Units Biological Reference IntervalsseravanakumarNo ratings yet
- Mindray Coagulation Reagent DD BrochureDocument1 pageMindray Coagulation Reagent DD BrochureAIINo ratings yet
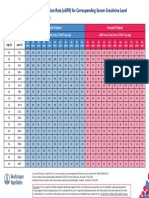
- Comparative Study: Formula Praktis Estimasi Laju: Filtrasi Glomerulus (LFG) Dengan Biomarker Kreatinin SerumDocument8 pagesComparative Study: Formula Praktis Estimasi Laju: Filtrasi Glomerulus (LFG) Dengan Biomarker Kreatinin SerumAchmad ThoriqNo ratings yet
- Daftar Reagent Di Laboratorium Tahun 2015Document4 pagesDaftar Reagent Di Laboratorium Tahun 2015nur aida utamiNo ratings yet
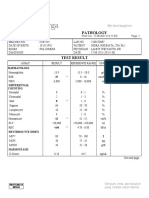
- Pathology: HaematologiDocument2 pagesPathology: HaematologiFerry SukinataNo ratings yet
- LiverDocument1 pageLiverkhanmohammadchinuNo ratings yet
- Hema I Chapter 11 - RBC IndicesDocument13 pagesHema I Chapter 11 - RBC IndicesSitra ZekeriyaNo ratings yet
- Test Name Value Unit Biological Ref Interval Biochemistry Liver Function Test (LFT)Document7 pagesTest Name Value Unit Biological Ref Interval Biochemistry Liver Function Test (LFT)Himanshu GarkhelNo ratings yet
- Diabetes Book HindiDocument18 pagesDiabetes Book HindiAdityaNo ratings yet
- 7 - MT Hematology Module 7 LectureDocument3 pages7 - MT Hematology Module 7 LectureAnthonyNo ratings yet
- Liquichek D-Dimer Control Levels Low, 1, 2 and 3: MétodoDocument3 pagesLiquichek D-Dimer Control Levels Low, 1, 2 and 3: Métodotavogaona8979No ratings yet
- Yumizen G CTRL I (Level 1) For Yumizen G LineDocument2 pagesYumizen G CTRL I (Level 1) For Yumizen G LinelilwatarslilNo ratings yet
- General Biochemistry: Biochemistry Tests Were Done With Mindray Bs 2000 & Rayto 420 & Mindray Bs380 & Capillarys SebiaDocument3 pagesGeneral Biochemistry: Biochemistry Tests Were Done With Mindray Bs 2000 & Rayto 420 & Mindray Bs380 & Capillarys Sebiajohnny.lip.322No ratings yet
- Haemoglobin Percentage: Visit Id: R7758972Document2 pagesHaemoglobin Percentage: Visit Id: R7758972iyengaarNo ratings yet
- Pathology & Clinical Laboratory (M) SDN - BHD: Scan QR For VerificationDocument1 pagePathology & Clinical Laboratory (M) SDN - BHD: Scan QR For VerificationAzhar SabriNo ratings yet
- L96 - M/S Om Sai Path Lab Chiriyatand Khas Mahal More Patna BIHAR Mobile No:9334498936Document2 pagesL96 - M/S Om Sai Path Lab Chiriyatand Khas Mahal More Patna BIHAR Mobile No:9334498936sunny SINGHNo ratings yet
- Egfr ChartDocument1 pageEgfr ChartMahesh DoshiNo ratings yet
- Blood Test ReportDocument1 pageBlood Test ReportDhruv JainNo ratings yet
- Haematology, Biochemistry, Serology and Immunology, Microbiology, Cytology, Histopathology, Endocrinology, Ultrasonography & X-RayDocument2 pagesHaematology, Biochemistry, Serology and Immunology, Microbiology, Cytology, Histopathology, Endocrinology, Ultrasonography & X-RayPankaj BeniwalNo ratings yet
- Parameter For Mindray Reagent On BS-380 (V9.0)Document3 pagesParameter For Mindray Reagent On BS-380 (V9.0)Aniket dubeyNo ratings yet
- Isaac Typhoid NegativeDocument5 pagesIsaac Typhoid Negativeganesh khondeNo ratings yet
- Sunshine Hospitals: Department of PathologyDocument2 pagesSunshine Hospitals: Department of PathologyVarun reddyNo ratings yet
- Lab - Report - BHAVISHKA JIDocument4 pagesLab - Report - BHAVISHKA JIYogeshKumarLoharNo ratings yet
- Juhi Shinde (871) 05.05.23Document6 pagesJuhi Shinde (871) 05.05.23Tushar ShindeNo ratings yet