You might also like
- AMOpportunities Certificate of ImmunizationDocument1 pageAMOpportunities Certificate of Immunizationashish guptaNo ratings yet
- Infectious Disease Medical Behavioral Screens AmendedDocument6 pagesInfectious Disease Medical Behavioral Screens AmendedHengkyNo ratings yet
- Cargo Security Awareness - Etextbook - 2nd - Ed - 2016 - TCGP-79Document185 pagesCargo Security Awareness - Etextbook - 2nd - Ed - 2016 - TCGP-79kien Duy Phan80% (5)
- COVID-19 (Coronavirus) Exposure Questionnaire: Part 1 - Applicable For All ApplicantsDocument2 pagesCOVID-19 (Coronavirus) Exposure Questionnaire: Part 1 - Applicable For All ApplicantsMovin PrabhakaranNo ratings yet
- A Healthy World Starts Here: Nwdi Requirements For Sars Cov-2 (Covid-19) Antibody Rapid Diagnostic TestDocument2 pagesA Healthy World Starts Here: Nwdi Requirements For Sars Cov-2 (Covid-19) Antibody Rapid Diagnostic TestEric NagumNo ratings yet
- COVID-19 Vaccination Consent Form: Basic Info: First Tell Us Who You AreDocument2 pagesCOVID-19 Vaccination Consent Form: Basic Info: First Tell Us Who You AreVAS skytelNo ratings yet
- Norsu Health Declaration Form 1 September 2022Document1 pageNorsu Health Declaration Form 1 September 2022Joshua Allen AjetoNo ratings yet
- COVID-19 physician notesDocument3 pagesCOVID-19 physician notessecretos webNo ratings yet
- Undertaking Declaration PD2022 - 030Document2 pagesUndertaking Declaration PD2022 - 030MejoNo ratings yet
- Minor COVID Vaccine ConsentDocument2 pagesMinor COVID Vaccine ConsentAlexis G. MamaniNo ratings yet
- Covid-19 Workplace Exposure Faqs v4 1 1Document3 pagesCovid-19 Workplace Exposure Faqs v4 1 1api-316753283No ratings yet
- GW Hospital MOU & Observer Health Information FormDocument2 pagesGW Hospital MOU & Observer Health Information Formengel0321hotmail.comNo ratings yet
- Wadena County COVID-19 Vaccination PolicyDocument9 pagesWadena County COVID-19 Vaccination PolicyinforumdocsNo ratings yet
- RCare For You Health Declaration For Child Less Than 5 Yrs Ver1.2 (Medical)Document2 pagesRCare For You Health Declaration For Child Less Than 5 Yrs Ver1.2 (Medical)Mexico EnglishNo ratings yet
- Intern Program - Health Evaluation Form: If Yes, Please List BelowDocument2 pagesIntern Program - Health Evaluation Form: If Yes, Please List BelowJHON FREDY VELÁSQUEZNo ratings yet
- Screening Script and Procedure For Reception and SchedulingDocument3 pagesScreening Script and Procedure For Reception and SchedulingJobert NarvaezNo ratings yet
- Health History and Immunization Form: University of Valley Forge - Health CenterDocument4 pagesHealth History and Immunization Form: University of Valley Forge - Health CenterBernard AmetepeNo ratings yet
- COVID-19 Vaccine Screening and Consent FormDocument2 pagesCOVID-19 Vaccine Screening and Consent FormKarina RojasNo ratings yet
- Medical Record FormDocument4 pagesMedical Record FormДария КоваленкоNo ratings yet
- Health Screening Requirements for Work Permit RenewalsDocument9 pagesHealth Screening Requirements for Work Permit Renewalsknop13No ratings yet
- Health Questionnaire FormDocument7 pagesHealth Questionnaire FormSadaf ShaukatNo ratings yet
- Self-Disclosure by Contractor Employees COVID-19 - 14-05-2020Document2 pagesSelf-Disclosure by Contractor Employees COVID-19 - 14-05-2020Ansar AliNo ratings yet
- COVID-19 (Coronavirus) Recovery QuestionnaireDocument3 pagesCOVID-19 (Coronavirus) Recovery QuestionnaireHasilwan ChanNo ratings yet
- COVID 19 Consent FormDocument2 pagesCOVID 19 Consent FormfvdssfdNo ratings yet
- Self-Disclosure by Contractor Employees COVID-19 (English)Document1 pageSelf-Disclosure by Contractor Employees COVID-19 (English)peters petersNo ratings yet
- Form B - Other Jobs - High - V High Risk TBDocument8 pagesForm B - Other Jobs - High - V High Risk TBMorshed HumayunNo ratings yet
- CONSENT FORM - COVID-19 VaccineDocument5 pagesCONSENT FORM - COVID-19 Vaccinebersabeh abayNo ratings yet
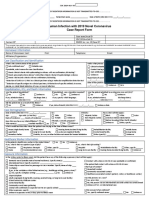
- Human Infection With 2019 Novel Coronavirus Case Report FormDocument2 pagesHuman Infection With 2019 Novel Coronavirus Case Report FormRicardo F. BernardinelliNo ratings yet
- Health Assessment Form For Students: YES NODocument1 pageHealth Assessment Form For Students: YES NOJohn AlvinNo ratings yet
- Health Assessment Form For Student 02 1Document1 pageHealth Assessment Form For Student 02 1GavinTLDNo ratings yet
- Annex A, B, and CDocument6 pagesAnnex A, B, and CJOHN GABRIEL CABIAANNo ratings yet
- COVID Vaccination Packet SFODocument16 pagesCOVID Vaccination Packet SFOferNo ratings yet
- Informed Consent UniversalDocument1 pageInformed Consent Universalahasgahsg031No ratings yet
- (IL) FMLA Certification Form Employee Condition Beatriz RuizDocument5 pages(IL) FMLA Certification Form Employee Condition Beatriz RuizBeatriz RuizNo ratings yet
- 2024 VPD FormFINAL 16012024Document5 pages2024 VPD FormFINAL 16012024dkid9876No ratings yet
- AMOpportunities Certificate of ImmunizationDocument1 pageAMOpportunities Certificate of ImmunizationАида АрзуманянNo ratings yet
- Covid-19 Test Claim FormDocument2 pagesCovid-19 Test Claim Formmuhammad anasNo ratings yet
- Adult Vaccine Access Program Covid Vaccine Final Consent FormDocument1 pageAdult Vaccine Access Program Covid Vaccine Final Consent FormJena LeeNo ratings yet
- FSSAI Vaccination Form - Tybar 2.5mlDocument2 pagesFSSAI Vaccination Form - Tybar 2.5mlanandsivNo ratings yet
- Occupational Health FormDocument3 pagesOccupational Health FormCherry Mañibo100% (1)
- Health Surveillance Form 2019 Novel Corona Virus: A. Clinical Symptoms/Signs YES NO RemarksDocument3 pagesHealth Surveillance Form 2019 Novel Corona Virus: A. Clinical Symptoms/Signs YES NO RemarksJohn Ervin AgenaNo ratings yet
- Workplace Readiness Guide for COVID-19Document37 pagesWorkplace Readiness Guide for COVID-19LNo ratings yet
- DOH-4359 (2010) Physician'S Order For Personal Care/Consumer Directed Personal Assistance ServicesDocument4 pagesDOH-4359 (2010) Physician'S Order For Personal Care/Consumer Directed Personal Assistance ServicesRebeca MartínezNo ratings yet
- COVID Questionnaire - FINALDocument2 pagesCOVID Questionnaire - FINALDeepanshu RathoreNo ratings yet
- Fitness Assesment FormDocument1 pageFitness Assesment FormJohn Mark RosalesNo ratings yet
- Preparing For Post Offer Evaluation & Health History Form 4.26.22Document13 pagesPreparing For Post Offer Evaluation & Health History Form 4.26.22Antonella VitaleNo ratings yet
- Health Screening Form Burhan Ullah KhanDocument1 pageHealth Screening Form Burhan Ullah KhanFareed KhanNo ratings yet
- COVID 19 Healthcare Workers GuideDocument9 pagesCOVID 19 Healthcare Workers GuidenilrmNo ratings yet
- 2019-ShadowerObserver-Application 191003 195038Document9 pages2019-ShadowerObserver-Application 191003 195038omer khanNo ratings yet
- COVID-19 Health Declaration FormDocument1 pageCOVID-19 Health Declaration Formkrizzane SuriaNo ratings yet
- PSW6 - PPHFDocument16 pagesPSW6 - PPHFanishthNo ratings yet
- Commonly Used Spanish Patient FormsDocument40 pagesCommonly Used Spanish Patient FormsCarlos VargasNo ratings yet
- New Query LetterDocument13 pagesNew Query LettersyawalNo ratings yet
- MD Occupational Health ProtocolDocument6 pagesMD Occupational Health ProtocolGareth GrechNo ratings yet
- Covid Questionnaire FormDocument2 pagesCovid Questionnaire FormtaguikenzoNo ratings yet
- Appendix 6 Undertaking - Declaration FormDocument1 pageAppendix 6 Undertaking - Declaration FormAr AsifNo ratings yet
- New Corona Form Revised Version-7Document1 pageNew Corona Form Revised Version-7Rishabh JainNo ratings yet
- MECKLENBURG COUNTY PUBLIC HEALTH - SAMPLE Positive COVID-19 Interview QuestionnaireDocument4 pagesMECKLENBURG COUNTY PUBLIC HEALTH - SAMPLE Positive COVID-19 Interview QuestionnaireWFAENo ratings yet
- Informed Consent: Republic of The Philippines National Police CommissionDocument6 pagesInformed Consent: Republic of The Philippines National Police CommissionAljomaih GatanelaNo ratings yet
- COVID-19 TEST CLAIMDocument2 pagesCOVID-19 TEST CLAIMnorhanaaNo ratings yet
- Bharti AXA Life Elite Advantage Plan 502-9743977 Kiranmayi Sayi YerukalapudiDocument1 pageBharti AXA Life Elite Advantage Plan 502-9743977 Kiranmayi Sayi YerukalapudiDixit SushmithaNo ratings yet
- COVID-19 Exposure Questionnaire for Healthcare WorkersDocument3 pagesCOVID-19 Exposure Questionnaire for Healthcare WorkersDixit SushmithaNo ratings yet
- 1277 - 2014 01 01 10 47 07 - 1388553427Document2 pages1277 - 2014 01 01 10 47 07 - 1388553427Dixit SushmithaNo ratings yet
- Name - Bharti AXA Life Elite Advantage PlanDocument8 pagesName - Bharti AXA Life Elite Advantage PlanDixit SushmithaNo ratings yet
- AST Study Centers 2021 Updated Till 25oct2021 GOVT DATADocument33 pagesAST Study Centers 2021 Updated Till 25oct2021 GOVT DATAprasadNo ratings yet
- Impact of Sugarcane Molasses in Concrete As Time Retarding and Water Reducing AdmixtureDocument131 pagesImpact of Sugarcane Molasses in Concrete As Time Retarding and Water Reducing AdmixtureMohamed MoralesNo ratings yet
- TECHNICALPAPER2Document8 pagesTECHNICALPAPER2spiderwebNo ratings yet
- Hoshizaki IM-500SAA Icemaker Service ManualDocument39 pagesHoshizaki IM-500SAA Icemaker Service ManualBenjamin DoverNo ratings yet
- Timbering Week 5Document22 pagesTimbering Week 5FikaduKitessa0% (1)
- Case3: What's in A Car 1. What Kind of Research Study Should Shridhar Undertake? Define TheDocument2 pagesCase3: What's in A Car 1. What Kind of Research Study Should Shridhar Undertake? Define TheRoshan kumar Rauniyar0% (3)
- 1 SMDocument9 pages1 SMhasanuddinnst1No ratings yet
- LPI PH PDFDocument4 pagesLPI PH PDFHumberto Tapias CutivaNo ratings yet
- Itp Concrete CoatingDocument4 pagesItp Concrete Coatingkaml100% (1)
- Writing Part 2 - An Essay: (120-180 Words)Document7 pagesWriting Part 2 - An Essay: (120-180 Words)María Daniela BroccardoNo ratings yet
- Lean Healthy Raw Food Winter RecipesDocument60 pagesLean Healthy Raw Food Winter RecipesKaio Sol100% (6)
- Individualized Learning Program Project Evaluation FormDocument3 pagesIndividualized Learning Program Project Evaluation Formakbisoi1No ratings yet
- Romeo and Julliet - Close Read AnalysisDocument5 pagesRomeo and Julliet - Close Read Analysisapi-514407929No ratings yet
- Earned Value Analysis 8 StepsDocument8 pagesEarned Value Analysis 8 StepsHira RazzaqNo ratings yet
- Mil STD 882eDocument104 pagesMil STD 882ecihan dağNo ratings yet
- Rulings On Healing and RukiyaDocument324 pagesRulings On Healing and RukiyatheproboxerNo ratings yet
- Probability and Statistics. ASSIGNMENT 2Document5 pagesProbability and Statistics. ASSIGNMENT 2ByhiswillNo ratings yet
- Choose the Right Low Boy Trailer ModelDocument42 pagesChoose the Right Low Boy Trailer ModelOdlnayer AllebramNo ratings yet
- Dental Cements: Dr. Hamida KhatunDocument39 pagesDental Cements: Dr. Hamida Khatunsakib samiNo ratings yet
- I Am Sharing 'ASSIGNMENT MAT099 - E08G5 - WRTTEN REPORT' With YouDocument23 pagesI Am Sharing 'ASSIGNMENT MAT099 - E08G5 - WRTTEN REPORT' With YouaqilNo ratings yet
- SEO-Optimized Title for Document on English Exam QuestionsDocument4 pagesSEO-Optimized Title for Document on English Exam Questionsminh buiNo ratings yet
- 4 A CompiledDocument167 pages4 A CompiledArjun MiddhaNo ratings yet
- Cell Structure & FunctionDocument38 pagesCell Structure & Functiongundogan21100% (1)
- Analyzing Historical DocumentDocument4 pagesAnalyzing Historical DocumentChristine Joy VillasisNo ratings yet
- Presentation - On SVAMITVADocument18 pagesPresentation - On SVAMITVAPraveen PrajapatiNo ratings yet
- Doctor's Office Call About Infected Foot InjuryDocument5 pagesDoctor's Office Call About Infected Foot InjuryNur annisa HarahapNo ratings yet
- Technical Information No. 12 Vermicular Graphite Cast Iron: MicrostructureDocument1 pageTechnical Information No. 12 Vermicular Graphite Cast Iron: MicrostructureVelina MilevaNo ratings yet
- The Right Help at The Right Time: MatterDocument24 pagesThe Right Help at The Right Time: MattermariustudoracheNo ratings yet
- Dual Domain Image Encryption Using Bit Plane Scrambling and Sub - Band ScramblingDocument16 pagesDual Domain Image Encryption Using Bit Plane Scrambling and Sub - Band Scramblingraja rishyantNo ratings yet