You might also like
- PADI Rescue Diver - Blank Knowledge ReviewDocument13 pagesPADI Rescue Diver - Blank Knowledge ReviewAj Quek67% (3)
- Redlands' 2015 California Public Records RequestsDocument26 pagesRedlands' 2015 California Public Records RequestsBeau Yarbrough100% (1)
- Surveillance of Fistula Function by Frequent.12Document4 pagesSurveillance of Fistula Function by Frequent.12PatríciaNo ratings yet
- A. ShalkamyDocument9 pagesA. ShalkamydeddybedahmksNo ratings yet
- SousaMorais2019 Article PercutaneousNephrostomyVsUreteDocument7 pagesSousaMorais2019 Article PercutaneousNephrostomyVsUreteraghad.bassalNo ratings yet
- S0090429521002594Document7 pagesS0090429521002594Mounia MarsouNo ratings yet
- 1 s2.0 S201325142400052X MainDocument3 pages1 s2.0 S201325142400052X Mainmosab.backkupNo ratings yet
- Endoscopic Ultrasound-Guided Portal Venous Access:: Diagnostic and Therapeutic ImplicationsDocument6 pagesEndoscopic Ultrasound-Guided Portal Venous Access:: Diagnostic and Therapeutic ImplicationsPNo ratings yet
- Ureterorenoscopy: Indications and Complications - A Retrospective StudyDocument6 pagesUreterorenoscopy: Indications and Complications - A Retrospective Studyhotland sitorusNo ratings yet
- Tsutsumi 1997Document6 pagesTsutsumi 1997Ahmad AlzawahrehNo ratings yet
- Histopathologic Features and Clinical Outcomes in 71 Cases of Bladder DiverticulaDocument6 pagesHistopathologic Features and Clinical Outcomes in 71 Cases of Bladder DiverticulaIrma Suriani DarwisNo ratings yet
- Magnetic Resonance Imaging Compared To Ultrasound As The Preferred Method For Diagnosing Intractable HaematospermiaDocument8 pagesMagnetic Resonance Imaging Compared To Ultrasound As The Preferred Method For Diagnosing Intractable HaematospermiaAhmad RafiqanTB0009No ratings yet
- Predictors of Cerebrospinal Fluid Leaks in Endoscopic Surgery For Pituitary TumorsDocument6 pagesPredictors of Cerebrospinal Fluid Leaks in Endoscopic Surgery For Pituitary Tumorsfabian arassiNo ratings yet
- Complicaciones Postesplenectomia 2Document6 pagesComplicaciones Postesplenectomia 2Miguel Angel Ruiz MarquezNo ratings yet
- Recurent EpistaxisDocument3 pagesRecurent EpistaxisFongmeicha Elizabeth MargarethaNo ratings yet
- ReoperastionDocument5 pagesReoperastionanon_235857083No ratings yet
- Operative Management of Anastomotic Leaks After Colorectal SurgeryDocument6 pagesOperative Management of Anastomotic Leaks After Colorectal SurgeryJorge OsorioNo ratings yet
- Factores de RiesgoDocument4 pagesFactores de RiesgoSiris Rieder GarridoNo ratings yet
- Complicatii IntraoperatoriiDocument9 pagesComplicatii IntraoperatoriiBogdan DinuNo ratings yet
- Ali Kordzadeh, Yiannis PanayiotopolousDocument23 pagesAli Kordzadeh, Yiannis PanayiotopolousArHamNo ratings yet
- RetrieveDocument11 pagesRetrieveMICHAEL NUGROHONo ratings yet
- Jurnal VaskularDocument5 pagesJurnal VaskulardrelvNo ratings yet
- Management of True Aneurysms of Hemodialysis Access FistulasDocument7 pagesManagement of True Aneurysms of Hemodialysis Access FistulasbobbyNo ratings yet
- Metaanalisis FD en Agudo Ajnr 223 Pacientes CagnazoDocument7 pagesMetaanalisis FD en Agudo Ajnr 223 Pacientes CagnazoangelNo ratings yet
- 10 1 1 525 6842Document6 pages10 1 1 525 6842sandyNo ratings yet
- 701 2022 Article 5445Document9 pages701 2022 Article 5445PeyepeyeNo ratings yet
- Mathieu TIPDocument5 pagesMathieu TIPIoannis ValioulisNo ratings yet
- BMC Surgery: Early Rectal Stenosis Following Stapled Rectal Mucosectomy For HemorrhoidsDocument6 pagesBMC Surgery: Early Rectal Stenosis Following Stapled Rectal Mucosectomy For Hemorrhoidsdinda24No ratings yet
- Jce80002 2413 2422Document10 pagesJce80002 2413 2422Erwin CandraNo ratings yet
- Adult Urology: ElsevierDocument6 pagesAdult Urology: Elsevierderr barrNo ratings yet
- Measure BUN Creat Urine LeakageDocument4 pagesMeasure BUN Creat Urine Leakagerendi wibowoNo ratings yet
- J Gie 2007 03 782Document1 pageJ Gie 2007 03 782Taregh KaramiNo ratings yet
- The Use of Single Stapling Techniques Reduces Anastomotic Complications in Minimal Invasive Rectal SurgeryDocument9 pagesThe Use of Single Stapling Techniques Reduces Anastomotic Complications in Minimal Invasive Rectal SurgeryHafidh HanifuddinNo ratings yet
- A-Line Complication PDFDocument8 pagesA-Line Complication PDFaeagesNo ratings yet
- Functional Outcomes of Surgical Treatment of Ureteral Injury Following Gynecological and Obstetrical SurgeryDocument4 pagesFunctional Outcomes of Surgical Treatment of Ureteral Injury Following Gynecological and Obstetrical SurgeryKharizmaNo ratings yet
- Ca SekumDocument7 pagesCa SekumNely M. RosyidiNo ratings yet
- Percutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaDocument6 pagesPercutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaCotaga IgorNo ratings yet
- 1 s2.0 S147751312300133X MainDocument7 pages1 s2.0 S147751312300133X MainYuki LaNo ratings yet
- 751-Article Text-2288-1-10-20220106Document6 pages751-Article Text-2288-1-10-20220106Arryza Fahrita IkhsaniNo ratings yet
- 2023 Warshaw JAVMADocument7 pages2023 Warshaw JAVMACarlos Rubiños AlonsoNo ratings yet
- UgiendosDocument12 pagesUgiendosManoj BurdakNo ratings yet
- TMP F0 AADocument4 pagesTMP F0 AAFrontiersNo ratings yet
- 10.1007@s00464 019 06670 9Document17 pages10.1007@s00464 019 06670 9Francisco Javier MacíasNo ratings yet
- Hämäläinen-Sainio1998 Article IncidenceOfFistulasAfterDrainaDocument5 pagesHämäläinen-Sainio1998 Article IncidenceOfFistulasAfterDrainaammarNo ratings yet
- Iranjradiol 14 03 21742Document5 pagesIranjradiol 14 03 21742AisahNo ratings yet
- A Retrospective Analysis of Ventriculoperitoneal Shunt Revision Cases of A Single InstituteDocument5 pagesA Retrospective Analysis of Ventriculoperitoneal Shunt Revision Cases of A Single InstituteDr. AyshaNo ratings yet
- Management of Venous Sinus - Related Epidural Hematomas - Parker2020Document10 pagesManagement of Venous Sinus - Related Epidural Hematomas - Parker2020Pgsharp ArianoNo ratings yet
- Santos 2017Document5 pagesSantos 2017Utami AsriNo ratings yet
- Predictors of Outcome For Anal Fistula Surgery: Maher A. Abbas, MD Christopher H. Jackson, Bs Philip I. Haigh, MD, MSCDocument6 pagesPredictors of Outcome For Anal Fistula Surgery: Maher A. Abbas, MD Christopher H. Jackson, Bs Philip I. Haigh, MD, MSCVan GoghNo ratings yet
- Art 20177509Document4 pagesArt 20177509Jashashree SaikiaNo ratings yet
- Aneurysm Characteristics and Risk of Rebleeding After Subarachnoid HaemorrhageDocument7 pagesAneurysm Characteristics and Risk of Rebleeding After Subarachnoid HaemorrhageanankastikNo ratings yet
- Outcomes of Ileal Conduit Urinary Diversion in Patients With Multiple SclerosisDocument7 pagesOutcomes of Ileal Conduit Urinary Diversion in Patients With Multiple SclerosisPutri Rizky AmaliaNo ratings yet
- Table 2 Preoperative Characteristics and Treatment of Patients Presenting With Complex Anal FistulaDocument4 pagesTable 2 Preoperative Characteristics and Treatment of Patients Presenting With Complex Anal FistulaTri Anna FitrianiNo ratings yet
- Surgical Treatment of Venous Malformations in Klippel-Trénaunay SyndromeDocument8 pagesSurgical Treatment of Venous Malformations in Klippel-Trénaunay SyndromenikitagustiNo ratings yet
- Chung PrognosisDocument6 pagesChung PrognosisMarlyn SuciningtiasNo ratings yet
- Outcome and Complication of Paediatric Dacryocystorhinostomy at Mardan Medical Complex Ophthalmology UnitDocument3 pagesOutcome and Complication of Paediatric Dacryocystorhinostomy at Mardan Medical Complex Ophthalmology UnitInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Aortic Balloon Occlusion For Controlling Intraoperative Hemorrhage in Patients With Placenta Previa Increta/percretaDocument6 pagesAortic Balloon Occlusion For Controlling Intraoperative Hemorrhage in Patients With Placenta Previa Increta/percretaClan MéxicoNo ratings yet
- Comparative Clinical Study Between Modified Ureteral Orthotopic Reimplantation and CohenDocument6 pagesComparative Clinical Study Between Modified Ureteral Orthotopic Reimplantation and CohenJulio GomezNo ratings yet
- Management of Colorectal Anastomotic Leakage-Differences Between Salvage and Anastomotic TakedownDocument6 pagesManagement of Colorectal Anastomotic Leakage-Differences Between Salvage and Anastomotic TakedownDumitru RadulescuNo ratings yet
- Complicaiones de La Ventriculostomia Agosto 2011Document6 pagesComplicaiones de La Ventriculostomia Agosto 2011Felipe Anduquia GarayNo ratings yet
- bien chung nieu mổ lấy thaiDocument4 pagesbien chung nieu mổ lấy thaiMint For MomsNo ratings yet
- XX 1-s2.0-S1748681512004184Document6 pagesXX 1-s2.0-S1748681512004184Ashwin KumarNo ratings yet
- XX IJU-25-461Document6 pagesXX IJU-25-461Ashwin KumarNo ratings yet
- XX Rru-11-269Document8 pagesXX Rru-11-269Ashwin KumarNo ratings yet
- XX Comparision of Uroflow Parameters Before and AfterDocument4 pagesXX Comparision of Uroflow Parameters Before and AfterAshwin KumarNo ratings yet
- Uro Owmetry and Evaluation of Voiding Disorders: Techniques in Urology October 1998Document8 pagesUro Owmetry and Evaluation of Voiding Disorders: Techniques in Urology October 1998Ashwin KumarNo ratings yet
- Lower Urinary Tract Function in Children and Adolescents Update ReportDocument11 pagesLower Urinary Tract Function in Children and Adolescents Update ReportAshwin KumarNo ratings yet
- Pediatric Surgery Case Taking Notes: Dr. Anusiri InugalaDocument44 pagesPediatric Surgery Case Taking Notes: Dr. Anusiri InugalaAshwin KumarNo ratings yet
- XX Uroflowmetric Evaluation of Patients With Hypospadias Treated in Our Clinic (#409281) - 523261Document4 pagesXX Uroflowmetric Evaluation of Patients With Hypospadias Treated in Our Clinic (#409281) - 523261Ashwin KumarNo ratings yet
- cs229.... Machine Language. Andrew NGDocument17 pagescs229.... Machine Language. Andrew NGkrishnaNo ratings yet
- Scientific Approaches For Impurity Profiling in New Pharmaceutical Substances and Its Products-An OverviewDocument18 pagesScientific Approaches For Impurity Profiling in New Pharmaceutical Substances and Its Products-An OverviewsrichainuluNo ratings yet
- Basic Concepts of SociologyDocument4 pagesBasic Concepts of SociologyAiman HaiqarlNo ratings yet
- DSP Lab RecordDocument97 pagesDSP Lab RecordLikhita UttamNo ratings yet
- Compliant Offshore StructureDocument50 pagesCompliant Offshore Structureapi-27176519100% (4)
- Hydrogen Codes and Standards Workshop: Naser ChowdhuryDocument24 pagesHydrogen Codes and Standards Workshop: Naser ChowdhuryDiana DhominicNo ratings yet
- January 2005 6677 Mechanics M1: Mark SchemeDocument7 pagesJanuary 2005 6677 Mechanics M1: Mark SchemeWael TareqNo ratings yet
- 413 1684 1 PB PDFDocument5 pages413 1684 1 PB PDFMhd RidwanNo ratings yet
- Appendix 2-4.ep31422 - g-16Document15 pagesAppendix 2-4.ep31422 - g-16bsnegi111No ratings yet
- Matter 1A Forms Properties and ChangesDocument47 pagesMatter 1A Forms Properties and ChangesSamKris Guerrero Malasaga100% (2)
- Amotec 12864Q DisplayDocument17 pagesAmotec 12864Q DisplayEdgarNo ratings yet
- J-20 Stealth Fighter Design Balances Speed and Agility - Defense Content From Aviation WeekDocument9 pagesJ-20 Stealth Fighter Design Balances Speed and Agility - Defense Content From Aviation WeekMahesNo ratings yet
- Product Life Cycle ManagementDocument35 pagesProduct Life Cycle ManagementRahul KumarNo ratings yet
- Installiation of Automatic Fire Sprinkler System and Design CalculationDocument8 pagesInstalliation of Automatic Fire Sprinkler System and Design CalculationSat AungNo ratings yet
- Newton Papers Letter Nat Phil Cohen EdDocument512 pagesNewton Papers Letter Nat Phil Cohen EdFernando ProtoNo ratings yet
- Lecture-I Introduction To Concrete TechnologyDocument102 pagesLecture-I Introduction To Concrete Technologyjs kalyana rama100% (4)
- PIA Rivalry Strategy MapDocument16 pagesPIA Rivalry Strategy MapRomeo KhanNo ratings yet
- Animal 1414Document6 pagesAnimal 1414trialink minsanNo ratings yet
- How To Write A Research Paper With Parenthetical DocumentationDocument5 pagesHow To Write A Research Paper With Parenthetical Documentationc9spy2qzNo ratings yet
- International StandardDocument8 pagesInternational Standardnazrul islamNo ratings yet
- CekocideDocument1 pageCekocideKaren Claire HorcaNo ratings yet
- NUMBERS 2 Percentage ChangeDocument2 pagesNUMBERS 2 Percentage ChangeDinangaNo ratings yet
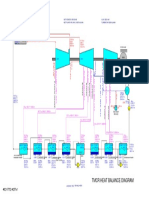
- 01 TMCR Heat Balance DiagramDocument1 page01 TMCR Heat Balance DiagramPrescila PalacioNo ratings yet
- GFRC Floating Concrete Hearth For Concrete Wood FiDocument11 pagesGFRC Floating Concrete Hearth For Concrete Wood FiJuliano. PQMNo ratings yet
- Heat Shrink CoatingDocument5 pagesHeat Shrink CoatingMekhmanNo ratings yet
- Ayurvedam For Hair Related IssuesDocument14 pagesAyurvedam For Hair Related IssuesGangadhar Yerraguntla100% (1)
- AnorexiaDocument1 pageAnorexiaCHIEF DOCTOR MUTHUNo ratings yet
- ISKRA Letak MC3xx 2016 Ver.4.0 2016.compressedDocument6 pagesISKRA Letak MC3xx 2016 Ver.4.0 2016.compressedmelanitisNo ratings yet