You might also like
- Impacted Wisdom Tooth, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandImpacted Wisdom Tooth, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- ZirconiaDocument674 pagesZirconiaKalpanaNo ratings yet
- Distribution Pattern of The Superior and Inferior Labial Arteries Impact For Safe Upper and Lower Lip Augmentation ProceduresDocument8 pagesDistribution Pattern of The Superior and Inferior Labial Arteries Impact For Safe Upper and Lower Lip Augmentation ProceduresLizeth Conde Orozco100% (1)
- Womens Basketball Spring Strength Training-2Document1 pageWomens Basketball Spring Strength Training-2api-548848665No ratings yet
- Sepsis Syndromes in Adults Epidemiology, Definitions, Clinical Presentation, Diagnosis, and Prognosis - UpToDate PDFDocument64 pagesSepsis Syndromes in Adults Epidemiology, Definitions, Clinical Presentation, Diagnosis, and Prognosis - UpToDate PDFCarolinaDeLaCruzDavilaNo ratings yet
- Dental Health EbookDocument15 pagesDental Health EbooktmetscherNo ratings yet
- Growing Beautiful Teeth: Simple Strategies for Your Child to Have Perfect Teeth for LifeFrom EverandGrowing Beautiful Teeth: Simple Strategies for Your Child to Have Perfect Teeth for LifeNo ratings yet
- V154 BSBLDR602 Assessment Task - 1Document3 pagesV154 BSBLDR602 Assessment Task - 1Briyidt Alejandra CaroNo ratings yet
- 160120prospectus 2019-2020 PDFDocument171 pages160120prospectus 2019-2020 PDFMUHAMMAD HASEEB ASHRAF MUHAMMAD ASHRAFNo ratings yet
- Dental Risk Assessment FormDocument2 pagesDental Risk Assessment FormSamantha TacadNo ratings yet
- New Patient Health History Form - Art of DentistryDocument4 pagesNew Patient Health History Form - Art of DentistryGiovanna L BarajasNo ratings yet
- Assessment of Dental Hygiene QuestionnaireDocument3 pagesAssessment of Dental Hygiene QuestionnaireShaheryar Ahmed KhanNo ratings yet
- Paediatric Mouth Care Survey For Nursing Staff: If Yes, What Are These Barriers?Document2 pagesPaediatric Mouth Care Survey For Nursing Staff: If Yes, What Are These Barriers?Daal ChawlNo ratings yet
- Adult Orthodontics: The Only Way To Have Permanently Straight Teeth Is To Wear A Retainer On A Part-Time Basis For LifeDocument2 pagesAdult Orthodontics: The Only Way To Have Permanently Straight Teeth Is To Wear A Retainer On A Part-Time Basis For LifeAANo ratings yet
- BOS - Counselling DocumentsDocument104 pagesBOS - Counselling DocumentsUmair Wali KhanNo ratings yet
- فورماDocument9 pagesفورما22368717No ratings yet
- ADA PatientSmart DenturesDocument5 pagesADA PatientSmart DenturesrindapuspaNo ratings yet
- 2020 Dental History Form PacketDocument6 pages2020 Dental History Form PacketLandon AllenNo ratings yet
- What You Should Know Before Getting Dental ImplantsDocument3 pagesWhat You Should Know Before Getting Dental ImplantsJosline MuriikiNo ratings yet
- OrthoDocument12 pagesOrthoSammy ShnayderNo ratings yet
- Sjogrens Syndrome Hybrid ImplantDocument4 pagesSjogrens Syndrome Hybrid ImplantIshita GuptaNo ratings yet
- Adult Orthodontics - IOSDocument2 pagesAdult Orthodontics - IOSRajshekhar BanerjeeNo ratings yet
- Sample NOT FOR Reproduction: Interproximal ReductionDocument2 pagesSample NOT FOR Reproduction: Interproximal ReductionhemaadriNo ratings yet
- Webb Doc PaperworkDocument8 pagesWebb Doc Paperworkapi-723577399No ratings yet
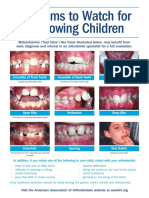
- Problems To Watch For in Growing ChildrenDocument2 pagesProblems To Watch For in Growing ChildrenMonica S. Alcouce TannerNo ratings yet
- Oral Procedures in Children: Dr. H. Ryan Kazemi Oral & Maxillofacial Surgery 4825 Bethesda Ave., #310 Bethesda, MD 20814Document8 pagesOral Procedures in Children: Dr. H. Ryan Kazemi Oral & Maxillofacial Surgery 4825 Bethesda Ave., #310 Bethesda, MD 20814Silvio DTNo ratings yet
- Oral and Denture Care PPT Finale 1Document75 pagesOral and Denture Care PPT Finale 1Jan Joseph BanzuelaNo ratings yet
- Dentalconsent-Vizilite 0001Document4 pagesDentalconsent-Vizilite 0001Orlando GesualdoNo ratings yet
- Recommendation FormsDocument1 pageRecommendation FormsRezi Sabutanan AmerilaNo ratings yet
- Recommendation FormsDocument1 pageRecommendation FormsRezi Sabutanan AmerilaNo ratings yet
- Consent Comp VeneersDocument3 pagesConsent Comp VeneersS MNo ratings yet
- Dental HistoryDocument2 pagesDental HistoryKgerbNo ratings yet
- 50 Dental CareDocument34 pages50 Dental CareEiveren Mae SutillezaNo ratings yet
- Preventing Dental Caries: Part 2. Case Studies in PreventionDocument6 pagesPreventing Dental Caries: Part 2. Case Studies in PreventionrespikNo ratings yet
- Recommendation FormsDocument1 pageRecommendation FormsJhon Rey DecatoriaNo ratings yet
- Commonly Asked Questions Regarding Dental SealantsDocument2 pagesCommonly Asked Questions Regarding Dental SealantsJosline MuriikiNo ratings yet
- Teaching PlanDocument22 pagesTeaching Planapi-564432337No ratings yet
- International Association of Pediatric Dentistry - Children 0-2 Years of AgeDocument14 pagesInternational Association of Pediatric Dentistry - Children 0-2 Years of AgeMafe SalazarNo ratings yet
- DENTIST DenturesDocument1 pageDENTIST DenturesRahulNo ratings yet
- Early Orthodontic TreatmentDocument1 pageEarly Orthodontic TreatmentSWATINo ratings yet
- Unit 4. Orthodontic TreatmentDocument1 pageUnit 4. Orthodontic Treatmentali veliNo ratings yet
- Preforma Modified by Hod SRDocument5 pagesPreforma Modified by Hod SRDrJayanti GhoshNo ratings yet
- Letter For Validation With InstrumentDocument7 pagesLetter For Validation With InstrumentShareinne TeamkNo ratings yet
- Dental Health Certificate FormDocument1 pageDental Health Certificate FormKimberly IlaganNo ratings yet
- February 2012Document1 pageFebruary 2012burlesonddsNo ratings yet
- 10 Treatments for Cracked or Chipped TeethDocument12 pages10 Treatments for Cracked or Chipped TeethDaveNo ratings yet
- How To Fix Gap TeethDocument9 pagesHow To Fix Gap TeethTrent SinanNo ratings yet
- Cleft Palate Pregnancy Mouth: Slideshow: Migraine Dos and Don'tsDocument6 pagesCleft Palate Pregnancy Mouth: Slideshow: Migraine Dos and Don'tsBenedictus HanjayaNo ratings yet
- Detailed Oral Health LessonDocument9 pagesDetailed Oral Health LessonRose Jyn Rosales MandayaNo ratings yet
- Improve Your Self-Confidence With Smile MakeoverDocument4 pagesImprove Your Self-Confidence With Smile MakeoverDental Practice TurkeyNo ratings yet
- Offpage SubmissonDocument8 pagesOffpage SubmissonriyankaprabhudigitalNo ratings yet
- 7b Oral Health Impact ProfileDocument2 pages7b Oral Health Impact ProfileTria Sesar AprianiNo ratings yet
- Tooth Developement in Babies and ToddlersDocument2 pagesTooth Developement in Babies and ToddlersCrapster GamingNo ratings yet
- Visiting The Dentist - Efe Gita Nov22023Document13 pagesVisiting The Dentist - Efe Gita Nov22023billahNo ratings yet
- Baby Teeth Matter-1Document2 pagesBaby Teeth Matter-1Manar ShawdaryNo ratings yet
- Effective Communications HandoutDocument1 pageEffective Communications HandoutSalai Thangte LaizoZanniatNo ratings yet
- 7 Daily Ways To Protect Your Teeth + 7 Remedies For Yellow TeethDocument6 pages7 Daily Ways To Protect Your Teeth + 7 Remedies For Yellow TeethWalid ZebbicheNo ratings yet
- ChildrensTeen Dental Car 7462609.ppsxDocument10 pagesChildrensTeen Dental Car 7462609.ppsxAdda VonDarkNo ratings yet
- Children/Teen Treatment Children/Teen TreatmentDocument10 pagesChildren/Teen Treatment Children/Teen TreatmentAdda VonDarkNo ratings yet
- Sample Dental Health Certificate-Optional: Section 1. To Be Completed by Parent or Guardian (Please Print)Document1 pageSample Dental Health Certificate-Optional: Section 1. To Be Completed by Parent or Guardian (Please Print)sherwin serranoNo ratings yet
- Visiting The Dentist British English TeacherDocument7 pagesVisiting The Dentist British English TeacherDaniel SantosNo ratings yet
- Presentation 2 Phase Treatment-2Document13 pagesPresentation 2 Phase Treatment-2memotarek2066No ratings yet
- Ngipin KoDocument5 pagesNgipin Kocarlsnerpios123No ratings yet
- Visiting The Dentist British English TeacherDocument7 pagesVisiting The Dentist British English Teacherliza kozachokNo ratings yet
- Understanding Alternative Energy ResourcesDocument7 pagesUnderstanding Alternative Energy ResourcesCharlie SumagaysayNo ratings yet
- C8 QuestionnairesDocument2 pagesC8 QuestionnairesCharlie SumagaysayNo ratings yet
- C3 QuestionnairesDocument2 pagesC3 QuestionnairesCharlie SumagaysayNo ratings yet
- UEP's Alternative Energy Course SyllabusDocument10 pagesUEP's Alternative Energy Course SyllabusCharlie SumagaysayNo ratings yet
- Filling a bucket with a garden hoseDocument3 pagesFilling a bucket with a garden hoseCharlie SumagaysayNo ratings yet
- C5 QuestionnairesDocument1 pageC5 QuestionnairesCharlie SumagaysayNo ratings yet
- C3 SolutionsDocument2 pagesC3 SolutionsCharlie SumagaysayNo ratings yet
- 09-12-22 MinutesDocument2 pages09-12-22 MinutesCharlie SumagaysayNo ratings yet
- Entre PassDocument2 pagesEntre PassCharlie SumagaysayNo ratings yet
- LetterDocument1 pageLetterCharlie SumagaysayNo ratings yet
- Auto Eng Ass 2Document5 pagesAuto Eng Ass 2Charlie SumagaysayNo ratings yet
- Pop CultureDocument5 pagesPop CultureCharlie SumagaysayNo ratings yet
- Industrial Plant EngineeringDocument9 pagesIndustrial Plant EngineeringCharlie SumagaysayNo ratings yet
- NBI Clearance Student Excuse RequestDocument1 pageNBI Clearance Student Excuse RequestCharlie SumagaysayNo ratings yet
- Vibar, Trexia Mae E. DMD-2A M3 Check-In ACTIVITY 4: With The AboveDocument1 pageVibar, Trexia Mae E. DMD-2A M3 Check-In ACTIVITY 4: With The AboveCharlie SumagaysayNo ratings yet
- Clothing LineDocument2 pagesClothing LineCharlie SumagaysayNo ratings yet
- Sumagaysay Activity4Document1 pageSumagaysay Activity4Charlie SumagaysayNo ratings yet
- SUMAGAYSAYDocument1 pageSUMAGAYSAYCharlie SumagaysayNo ratings yet
- A Reflection Paper News Title: PH Boosts Action For Climate, Community ResilienceDocument1 pageA Reflection Paper News Title: PH Boosts Action For Climate, Community ResilienceCharlie SumagaysayNo ratings yet
- SUMAGAYSAY, Charlie T. BS-Mechanical Engineering II 202098 PE 4 - Module 5 Knowledge Check Saq 1Document1 pageSUMAGAYSAY, Charlie T. BS-Mechanical Engineering II 202098 PE 4 - Module 5 Knowledge Check Saq 1Charlie SumagaysayNo ratings yet
- Medical Information Record FormDocument2 pagesMedical Information Record FormCharlie SumagaysayNo ratings yet
- A Reflection Paper News Title:PH Boosts Action For Climate, Community ResilienceDocument1 pageA Reflection Paper News Title:PH Boosts Action For Climate, Community ResilienceCharlie SumagaysayNo ratings yet
- Dimension Data To Be Gathered Data: Technoprenuership Summer Class 2022 Modul1BDocument1 pageDimension Data To Be Gathered Data: Technoprenuership Summer Class 2022 Modul1BCharlie SumagaysayNo ratings yet
- Mantenimiento Mecanico Residuos PDFDocument206 pagesMantenimiento Mecanico Residuos PDFGladys Gabriela Quispe RamosNo ratings yet
- Sorry, Wrong NumberDocument12 pagesSorry, Wrong NumberLaarni Airalyn CabreraNo ratings yet
- DR Barbara StarfieldDocument37 pagesDR Barbara StarfieldSuyanto SuyantoNo ratings yet
- Chloe Ting - 2 Weeks Shred Challenge - Free Workout ProgramDocument5 pagesChloe Ting - 2 Weeks Shred Challenge - Free Workout ProgramIndecisiveGurl100% (2)
- Dat e Physicians Order RationaleDocument4 pagesDat e Physicians Order Rationaleember parkNo ratings yet
- Wahyu Agung Kenworth Motors Case StudyDocument2 pagesWahyu Agung Kenworth Motors Case StudyWahyu Utama100% (1)
- How Do You Assess Biopure's Potential in The Human Market? The Animal Market? Human MarketDocument8 pagesHow Do You Assess Biopure's Potential in The Human Market? The Animal Market? Human MarketYilei RenNo ratings yet
- Policy Paper-Bpa108Document6 pagesPolicy Paper-Bpa108Aripin SangcopanNo ratings yet
- MR No. Urine Test ResultsDocument1 pageMR No. Urine Test Results112345678900No ratings yet
- Neural Mobilization: The Impossible: RichardDocument3 pagesNeural Mobilization: The Impossible: Richardsonali soumyashreeNo ratings yet
- Soy - A Review of The Literature - ALPHARAJDocument18 pagesSoy - A Review of The Literature - ALPHARAJIshantBansalNo ratings yet
- Spanish Dissertation TopicsDocument8 pagesSpanish Dissertation TopicsWritingPaperServicesToledo100% (1)
- General Part 25Document15 pagesGeneral Part 25Jean PangoNo ratings yet
- Barry Jones Correction ##Document2 pagesBarry Jones Correction ##Dr. Emad Elbadawy د عماد البدويNo ratings yet
- Pelaksanaan Perawatan Luka Post Operasi Sectio Caesarea Sesuai Standar Operasional ProsedurDocument9 pagesPelaksanaan Perawatan Luka Post Operasi Sectio Caesarea Sesuai Standar Operasional Prosedural ghaisaniNo ratings yet
- 5 6136226561843528157Document15 pages5 6136226561843528157Om Prakash RajNo ratings yet
- Prism 3 L&S-51-100Document50 pagesPrism 3 L&S-51-100bui thangNo ratings yet
- HHA - X-MET8000 Optimum + Expert Performance Document (Alloy) - Thin Window - V1-3Document5 pagesHHA - X-MET8000 Optimum + Expert Performance Document (Alloy) - Thin Window - V1-3Paula InesNo ratings yet
- Sensitive Care For The Deaf PDFDocument7 pagesSensitive Care For The Deaf PDFMohamedson MazzuNo ratings yet
- BSBMGT605 - BSBMGT615 Task 5.3 - Professional Development ReportDocument4 pagesBSBMGT605 - BSBMGT615 Task 5.3 - Professional Development ReportFernando Covos100% (1)
- Leyna Slivka-5Document1 pageLeyna Slivka-5api-490419585No ratings yet
- Pies Life Stages 88 SlidesDocument88 pagesPies Life Stages 88 Slidesapi-200177496100% (2)
- BSBLED809 Rsearch & Confirm Career Trends Assessment 1: Punam Pun TS 536Document12 pagesBSBLED809 Rsearch & Confirm Career Trends Assessment 1: Punam Pun TS 536dibesh dhakalNo ratings yet
- Vital-Action LevelsDocument34 pagesVital-Action LevelsLuis GallegosNo ratings yet
- Massive Hemoptysis An Update On The Role of Bronchoscopy in Diagnosis and Management PDFDocument21 pagesMassive Hemoptysis An Update On The Role of Bronchoscopy in Diagnosis and Management PDFdoc_next_doorNo ratings yet
- OSHA Form 301 Incident ReportDocument1 pageOSHA Form 301 Incident ReportjorgeNo ratings yet