You might also like
- Edtpa Elm Planning Commentary SandovalmarinaDocument9 pagesEdtpa Elm Planning Commentary Sandovalmarinaapi-251346191100% (3)
- GTSE Online Class III MathsDocument13 pagesGTSE Online Class III Mathssridhar100% (3)
- Givemed: A Webportal For Medicine Distribution Among Poverty-Stricken PeopleDocument7 pagesGivemed: A Webportal For Medicine Distribution Among Poverty-Stricken Peoplearchana palNo ratings yet
- Embedded Sat Ate Machines ImplementationDocument11 pagesEmbedded Sat Ate Machines ImplementationObamaDoutrinadorNo ratings yet
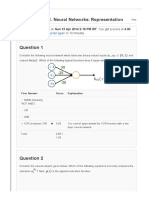
- Feedback — VIII. Neural Networks: Representation HelpDocument5 pagesFeedback — VIII. Neural Networks: Representation HelpChaitanya Kumar0% (1)
- Analyzing Financial Data and Implementing Financial Models Using RDocument360 pagesAnalyzing Financial Data and Implementing Financial Models Using RVikas Gupta100% (1)
- Mary Mavole NdoloDocument23 pagesMary Mavole NdoloJohnson MavoleNo ratings yet
- Björkman Svensson 2008Document36 pagesBjörkman Svensson 2008NPNo ratings yet
- National Volunteering in Mongolia - A Paper Presented To 3rd ISTR Conference by Glenn Benablo and Malou JuanitoDocument10 pagesNational Volunteering in Mongolia - A Paper Presented To 3rd ISTR Conference by Glenn Benablo and Malou JuanitoGlenn Bede A.Benablo100% (1)
- Understanding Factors Influencing The Adoption of Mhealth by Theelderly An Extension of The UTAUT33 PDFDocument10 pagesUnderstanding Factors Influencing The Adoption of Mhealth by Theelderly An Extension of The UTAUT33 PDFআল আমিনNo ratings yet
- Bjrkman PowerPeopleEvidence 2009 (2)Document36 pagesBjrkman PowerPeopleEvidence 2009 (2)maria jose vegaNo ratings yet
- Maternal 1Document10 pagesMaternal 1Inty Defly NandNo ratings yet
- Upazila Ngos: Public Health Has Been Defined As "The Science and Art of Preventing Disease, Prolonging LifeDocument14 pagesUpazila Ngos: Public Health Has Been Defined As "The Science and Art of Preventing Disease, Prolonging Lifehasibul khalidNo ratings yet
- Review of Literature on Healthcare Challenges in Rural AreasDocument12 pagesReview of Literature on Healthcare Challenges in Rural AreasJahzeel CubillaNo ratings yet
- Monica Utari Mariana LR 16.12Document8 pagesMonica Utari Mariana LR 16.12Bunda QueenaNo ratings yet
- MalawiDocument10 pagesMalawihst939100% (1)
- 2020 Article 5485Document8 pages2020 Article 5485marikum74No ratings yet
- An Evaluation of Health Systems Equity In: Indonesia: Study ProtocolDocument10 pagesAn Evaluation of Health Systems Equity In: Indonesia: Study ProtocolChristhin EsterNo ratings yet
- POLS 1503 Learning Journal Unit 7Document5 pagesPOLS 1503 Learning Journal Unit 7Cherry HtunNo ratings yet
- Sahn Etal 2003Document19 pagesSahn Etal 2003Neus Torres BlasNo ratings yet
- Universal Health Coverage in Morocco The Way To Reduce Inequalities ADocument8 pagesUniversal Health Coverage in Morocco The Way To Reduce Inequalities AChaymae SahraouiNo ratings yet
- Asia Pacific Health Challanges in 2050Document4 pagesAsia Pacific Health Challanges in 2050Shela Putri SundawaNo ratings yet
- Research ArticleDocument10 pagesResearch ArticleKrisleen AbrenicaNo ratings yet
- Role of Maternity Waiting Homes in Reduction of Maternal Mortality in EthiopiaDocument10 pagesRole of Maternity Waiting Homes in Reduction of Maternal Mortality in EthiopiaTegenne LegesseNo ratings yet
- Improving Emergency Obstetric Referral Systems in Low and Middle Income Countries: A Qualitative Study in A Tertiary Health Facility in GhanaDocument10 pagesImproving Emergency Obstetric Referral Systems in Low and Middle Income Countries: A Qualitative Study in A Tertiary Health Facility in GhanaTaklu Marama M. BaatiiNo ratings yet
- Mobile Health Information System: A Mobile App. To Aid Health Workers Relate Health InformationDocument12 pagesMobile Health Information System: A Mobile App. To Aid Health Workers Relate Health InformationMamanya Fadhil HaniNo ratings yet
- Health Equity and Migrants in The Greater Mekong SubregionDocument11 pagesHealth Equity and Migrants in The Greater Mekong SubregionRafif DaffaNo ratings yet
- Art 3A10.1186 2Fs12962 015 0030 3Document10 pagesArt 3A10.1186 2Fs12962 015 0030 3Syukron MakmunNo ratings yet
- Reaching The Unreachable: Barriers of The Poorest To Accessing NGO Healthcare Services in BangladeshDocument11 pagesReaching The Unreachable: Barriers of The Poorest To Accessing NGO Healthcare Services in BangladeshjlventiganNo ratings yet
- Rural FinalDocument11 pagesRural Finalapi-530825663No ratings yet
- Uhc Via PHCDocument19 pagesUhc Via PHCTeslim RajiNo ratings yet
- ResearchDocument27 pagesResearchAddisie TageleNo ratings yet
- Geissler 2015Document8 pagesGeissler 2015Jean M Huaman FiallegaNo ratings yet
- Abstract The Roleof Health Information Systemsin Achieving Universal Health Coverage AbdullaDocument2 pagesAbstract The Roleof Health Information Systemsin Achieving Universal Health Coverage AbdullaROBBIE PALCENo ratings yet
- Advancing The Dialogue - Mhealth AllianceDocument30 pagesAdvancing The Dialogue - Mhealth AllianceSteveEpsteinNo ratings yet
- Innovative Healthcare ApplicationsDocument57 pagesInnovative Healthcare ApplicationsojuNo ratings yet
- Accessibility of Primary Health Care Services: A Case Study of Kadakola Primary Health Centre in Mysore DistrictDocument12 pagesAccessibility of Primary Health Care Services: A Case Study of Kadakola Primary Health Centre in Mysore DistrictTharangini MNo ratings yet
- ProposalDocument19 pagesProposalMohammedNo ratings yet
- Impact of COVID-19 on Travel Behavior and Mode Choice in IndiaDocument4 pagesImpact of COVID-19 on Travel Behavior and Mode Choice in IndiaSk AslamNo ratings yet
- MLHWCountryCaseStudies Annex6 MozambiqueDocument20 pagesMLHWCountryCaseStudies Annex6 Mozambique高世超No ratings yet
- Telemedicine and Its BenefitsDocument27 pagesTelemedicine and Its Benefitsabidrk_21789No ratings yet
- Imci in MalawiDocument13 pagesImci in MalawiMikael StevanNo ratings yet
- Disaster 3 Ijerph 15 01879 v2Document29 pagesDisaster 3 Ijerph 15 01879 v2Devi SiswaniNo ratings yet
- Jurnal Jaminan KesDocument25 pagesJurnal Jaminan KesMeisya MonicaNo ratings yet
- Healthcare in Equatorial Guinea, West Africa: Obstacles and Barriers To CareDocument9 pagesHealthcare in Equatorial Guinea, West Africa: Obstacles and Barriers To CareRila Vita SariNo ratings yet
- Online Antenatal Consultation System Based On UML and Web Engineering ApproachDocument10 pagesOnline Antenatal Consultation System Based On UML and Web Engineering ApproachthesijNo ratings yet
- Limited Access To Health CareDocument5 pagesLimited Access To Health CarezeeshanNo ratings yet
- International Journal of Information Management: M. Nick HajliDocument4 pagesInternational Journal of Information Management: M. Nick HajlialfaNo ratings yet
- Factors Affecting Medical Services in Rural PhilippinesDocument5 pagesFactors Affecting Medical Services in Rural PhilippinesJohn Lesther PabiloniaNo ratings yet
- Use of Family Planning and Child Health Services in The Private Sector: An Equity Analysis of 12 DHS SurveysDocument12 pagesUse of Family Planning and Child Health Services in The Private Sector: An Equity Analysis of 12 DHS SurveysUpik SupuNo ratings yet
- Gaps in Universal Health Coverage in Malawi: A Qualitative Study in Rural CommunitiesDocument10 pagesGaps in Universal Health Coverage in Malawi: A Qualitative Study in Rural CommunitiesEma Nur FitrianaNo ratings yet
- Skilled Migration and Health Outcomes in Developing CountriesDocument17 pagesSkilled Migration and Health Outcomes in Developing Countriesfaseeh3335057No ratings yet
- K007 ANC KofintiDocument20 pagesK007 ANC KofintiRaymond ElikplimNo ratings yet
- International Journal For Equity in HealthDocument12 pagesInternational Journal For Equity in HealthjlventiganNo ratings yet
- Innovative Ways To Meet Health Challenges of Urban India - Radhika Arora - Sourav Neogi - Madhavi MisraDocument9 pagesInnovative Ways To Meet Health Challenges of Urban India - Radhika Arora - Sourav Neogi - Madhavi MisraJimmy KatiraNo ratings yet
- "Sehat Sahulat Program" - A Leap Into The Universal Health CoveraDocument9 pages"Sehat Sahulat Program" - A Leap Into The Universal Health Coverasameershah9sNo ratings yet
- Assignment Cover PageDocument11 pagesAssignment Cover PageSahadat HossainNo ratings yet
- Urban Health Policy ForumDocument5 pagesUrban Health Policy ForumTeddy CurranNo ratings yet
- Platforms For Sustainable Health Systems in Disadvantaged Communities: University of Denver - Jaishankar Memorial Center Concept PaperDocument4 pagesPlatforms For Sustainable Health Systems in Disadvantaged Communities: University of Denver - Jaishankar Memorial Center Concept PaperRandall KuhnNo ratings yet
- CAL Dr.Document16 pagesCAL Dr.Jimmy baginzNo ratings yet
- Essential ArticleDocument16 pagesEssential Articleapi-708352337No ratings yet
- Pankey Matt Hcin Capstone Paper FinalDocument15 pagesPankey Matt Hcin Capstone Paper Finalapi-542676458No ratings yet
- Proposed TeleMedicine Program For Rural Areas in Saudi ArabiaDocument29 pagesProposed TeleMedicine Program For Rural Areas in Saudi ArabiaMohamed Alkherb100% (1)
- Global Health Research: Closing Gaps, Expanding AccessDocument4 pagesGlobal Health Research: Closing Gaps, Expanding AccessAna GioacasNo ratings yet
- ANFIS-ABC MODEL PREDICTS TBM PERFORMANCEDocument10 pagesANFIS-ABC MODEL PREDICTS TBM PERFORMANCEASHUTOSH OJHANo ratings yet
- Public Transport Accessibility: A Literature Review: Periodica Polytechnica Transportation Engineering February 2018Document9 pagesPublic Transport Accessibility: A Literature Review: Periodica Polytechnica Transportation Engineering February 2018Al Hilal Ikhlasnul AmalNo ratings yet
- Travel Time To Health Facilities As A Marker of Geographical Accessibility Across Heterogeneous Land Coverage in PeruDocument10 pagesTravel Time To Health Facilities As A Marker of Geographical Accessibility Across Heterogeneous Land Coverage in PeruASHUTOSH OJHANo ratings yet
- Transport's impact on health and wellbeingDocument72 pagesTransport's impact on health and wellbeingASHUTOSH OJHANo ratings yet
- The Application of Adaptive Neuro-Fuzzy Inference System and Fuzzy Delphi Technique To Assess Socio-Economic Impacts of Construction of Rural RoadsDocument21 pagesThe Application of Adaptive Neuro-Fuzzy Inference System and Fuzzy Delphi Technique To Assess Socio-Economic Impacts of Construction of Rural RoadsASHUTOSH OJHANo ratings yet
- 004-Guidebook and Research Plan To Help Communities Improve Transportation To Health-Care ServicesDocument191 pages004-Guidebook and Research Plan To Help Communities Improve Transportation To Health-Care ServicesASHUTOSH OJHANo ratings yet
- Primary Health Care and Sustainable Development goals-SDG GoalsDocument9 pagesPrimary Health Care and Sustainable Development goals-SDG GoalsASHUTOSH OJHANo ratings yet
- Review-Health Systems in India PDFDocument4 pagesReview-Health Systems in India PDFTehMarianNo ratings yet
- Accessibility and Site Suitability For Healthcare Services Using GIS Based Hybrid Decision-Making Approach A Study in Murshidabad, IndiaDocument18 pagesAccessibility and Site Suitability For Healthcare Services Using GIS Based Hybrid Decision-Making Approach A Study in Murshidabad, IndiaASHUTOSH OJHANo ratings yet
- 01-Accessibility Analysis of Healthcare Facility Using GIS-Case Study of TrichyDocument8 pages01-Accessibility Analysis of Healthcare Facility Using GIS-Case Study of TrichyASHUTOSH OJHANo ratings yet
- 01 - Chapter-01-TRAFFIC ENG. & TRANSPORT PLANNING - KADIYALIDocument12 pages01 - Chapter-01-TRAFFIC ENG. & TRANSPORT PLANNING - KADIYALIASHUTOSH OJHANo ratings yet
- 03-Chapter-03-TRAFFIC ENG. & TRANSPORT PLANNING - KADIYALIDocument11 pages03-Chapter-03-TRAFFIC ENG. & TRANSPORT PLANNING - KADIYALIASHUTOSH OJHANo ratings yet
- 02-Chapter-02-TRAFFIC ENG. & TRANSPORT PLANNING - KADIYALIDocument8 pages02-Chapter-02-TRAFFIC ENG. & TRANSPORT PLANNING - KADIYALIASHUTOSH OJHANo ratings yet
- 00 - Content-Traffic Eng. & Transport Planning - KadiyaliDocument23 pages00 - Content-Traffic Eng. & Transport Planning - KadiyaliASHUTOSH OJHA100% (5)
- 03-Using A GIS To Support The Spatial Reorganization of Outpatient Care Services Delivery in ItalyDocument16 pages03-Using A GIS To Support The Spatial Reorganization of Outpatient Care Services Delivery in ItalyASHUTOSH OJHANo ratings yet
- 05-GIS and The Future of Public Health - GIS LoungeDocument8 pages05-GIS and The Future of Public Health - GIS LoungeASHUTOSH OJHANo ratings yet
- 06-GIS and Health CareDocument21 pages06-GIS and Health CareASHUTOSH OJHANo ratings yet
- QES164Document7 pagesQES164ASHUTOSH OJHANo ratings yet
- Factors Affecting Access To Primary Health Care Services For Persons With Disabilities in Rural Areas: A "Best-Fit" Framework SynthesisDocument13 pagesFactors Affecting Access To Primary Health Care Services For Persons With Disabilities in Rural Areas: A "Best-Fit" Framework SynthesisASHUTOSH OJHANo ratings yet
- Evaluation of Public Transport-Based Accessibility To Health Facility C... Onsidering Spatial Hetrogenity....... VVIDocument10 pagesEvaluation of Public Transport-Based Accessibility To Health Facility C... Onsidering Spatial Hetrogenity....... VVIASHUTOSH OJHANo ratings yet
- The Lancet Global Health Commission: Executive SummaryDocument57 pagesThe Lancet Global Health Commission: Executive SummaryASHUTOSH OJHANo ratings yet
- "We Are Called The Et Cetera": Experiences of The Poor With Health Financing Reforms That Target Them in KenyaDocument14 pages"We Are Called The Et Cetera": Experiences of The Poor With Health Financing Reforms That Target Them in KenyaASHUTOSH OJHANo ratings yet
- Mhealth and Perceived Quality of Care Delivery: A Conceptual Model and ValidationDocument13 pagesMhealth and Perceived Quality of Care Delivery: A Conceptual Model and ValidationASHUTOSH OJHANo ratings yet
- Acessibility Health PDFDocument13 pagesAcessibility Health PDFClauciane Dias de LimaNo ratings yet
- Spatiotemporal Simulation of Future Land Use/Cover Change Scenarios in The Tokyo Metropolitan AreaDocument18 pagesSpatiotemporal Simulation of Future Land Use/Cover Change Scenarios in The Tokyo Metropolitan AreaASHUTOSH OJHANo ratings yet
- Data and strategies to improve transportation and public healthDocument8 pagesData and strategies to improve transportation and public healthASHUTOSH OJHANo ratings yet
- MSC Programme in Urban Management and Development: Rotterdam, The Netherlands September 2016Document80 pagesMSC Programme in Urban Management and Development: Rotterdam, The Netherlands September 2016ASHUTOSH OJHANo ratings yet
- JD - Graduate Town Planner - Infrastructure Planning - UK FinalDocument6 pagesJD - Graduate Town Planner - Infrastructure Planning - UK FinalASHUTOSH OJHANo ratings yet
- Payment Information: Total Fare INR 7,097.00Document2 pagesPayment Information: Total Fare INR 7,097.00ASHUTOSH OJHANo ratings yet
- Statistical MethodsDocument16 pagesStatistical MethodsyasheshgaglaniNo ratings yet
- Statistics Term Paper ExampleDocument7 pagesStatistics Term Paper Exampleafmzrxbdfadmdq100% (1)
- Control and Estimation of A Quadcopter Dynamical MDocument14 pagesControl and Estimation of A Quadcopter Dynamical MmahendranavionicsNo ratings yet
- Inclined PlanesDocument4 pagesInclined PlanesnotgettingitNo ratings yet
- 2021MATHADVHO9.2 Learning ModuleDocument120 pages2021MATHADVHO9.2 Learning ModuleChang CarelNo ratings yet
- cs301 MCQSDocument6 pagescs301 MCQSfairy9966No ratings yet
- TransformationDocument12 pagesTransformationDevil InsideNo ratings yet
- Naca AnlsysDocument30 pagesNaca AnlsysAli OkumuşNo ratings yet
- Comp Neuro Syl Lab Us 2018Document3 pagesComp Neuro Syl Lab Us 2018Andrej IlićNo ratings yet
- Math 121A: Homework 8 (Due April 10)Document2 pagesMath 121A: Homework 8 (Due April 10)cfisicasterNo ratings yet
- Li 2021Document9 pagesLi 2021Smruti Ranjan PattanayakNo ratings yet
- Std. 12th Perfect Physics Vol. IDocument27 pagesStd. 12th Perfect Physics Vol. Iadhikarybhola50No ratings yet
- Kmpme 2 PDocument889 pagesKmpme 2 PIlie CiorneiNo ratings yet
- How financial incentives impact employee motivationDocument9 pagesHow financial incentives impact employee motivationsisay mamo100% (3)
- Midterm 2 Practice A KeyDocument11 pagesMidterm 2 Practice A KeysalmanshokhaNo ratings yet
- Inception-V4, Inception-ResNet and The Impact of Residual Connections On LearningDocument12 pagesInception-V4, Inception-ResNet and The Impact of Residual Connections On LearningShubham ChaudharyNo ratings yet
- Pre-Bankruptcy Financial Performance of Firms: Do Size and Industry Matter?Document6 pagesPre-Bankruptcy Financial Performance of Firms: Do Size and Industry Matter?Livia PredaNo ratings yet
- BungomaDISTRICT Roadclass SurfTypeDocument1 pageBungomaDISTRICT Roadclass SurfTypeJavan OmitiNo ratings yet
- Attracting and Repelling Lagrangian Coherent Structures From A Single ComputationDocument11 pagesAttracting and Repelling Lagrangian Coherent Structures From A Single ComputationRebeca De la FuenteNo ratings yet
- Little's Law*: *J. D. C. Little, A proof of the queueing formula: L = λW,Document25 pagesLittle's Law*: *J. D. C. Little, A proof of the queueing formula: L = λW,Mariam MassaȜdehNo ratings yet
- IGCSE-I Dec Assessment Syllabus 2023-24Document5 pagesIGCSE-I Dec Assessment Syllabus 2023-24Khadijah AbbasiNo ratings yet
- Fracture Mechanics Study Compact Tension SpecimenDocument7 pagesFracture Mechanics Study Compact Tension SpecimencsmanienNo ratings yet
- Homework Persuasive EssayDocument7 pagesHomework Persuasive Essayafaaoozgf100% (1)
- Whitepaper Laser-Tracker Hydro Jan09Document7 pagesWhitepaper Laser-Tracker Hydro Jan09Sagar PatkiNo ratings yet
- G3 - Math - Study - Guide - 2nd - Midterm TestDocument8 pagesG3 - Math - Study - Guide - 2nd - Midterm Testphuongnguyen21022k5.ewaNo ratings yet