You might also like
- BELLA Automatic Electric Spiralizer Recipe Book PDFDocument28 pagesBELLA Automatic Electric Spiralizer Recipe Book PDFJai's EpicenterNo ratings yet
- Ppii Tutorial ManualDocument145 pagesPpii Tutorial ManualFabio BolivarNo ratings yet
- Jurnal Anastesi 3Document9 pagesJurnal Anastesi 3ainunNo ratings yet
- Impact of Postoperative Dexmedetomidine Infusion On Incidence of Delirium in Elderly Patients Undergoing Major Elective Noncardiac Surgery2019Document12 pagesImpact of Postoperative Dexmedetomidine Infusion On Incidence of Delirium in Elderly Patients Undergoing Major Elective Noncardiac Surgery2019Cláudia Regina FernandesNo ratings yet
- Dexmedetomidina Prevencion Delirium PostoperatorioDocument8 pagesDexmedetomidina Prevencion Delirium PostoperatorioJoelGámezNo ratings yet
- Bo-Jie Wang, Chun-Jing Li, Jian Hu, Huai-Jin Li, Chao Guo, Zhen-Han Wang, Qiao-Chu Zhang, Dong-Liang Mu, Dong-Xin WangDocument6 pagesBo-Jie Wang, Chun-Jing Li, Jian Hu, Huai-Jin Li, Chao Guo, Zhen-Han Wang, Qiao-Chu Zhang, Dong-Liang Mu, Dong-Xin WangferrevNo ratings yet
- Kelompok 4Document8 pagesKelompok 4TaraaNo ratings yet
- Intranasal Premedication With Dexmedetomidine Versus Midazolam For Pediatric Patients in Ophthalmic Surgery: A Randomized Controlled StudyDocument8 pagesIntranasal Premedication With Dexmedetomidine Versus Midazolam For Pediatric Patients in Ophthalmic Surgery: A Randomized Controlled StudyPablo Segales BautistaNo ratings yet
- Dexmedetomidine Versus Propofol Sedation In.8Document11 pagesDexmedetomidine Versus Propofol Sedation In.8antoine.dovalNo ratings yet
- Hipofisis 7Document13 pagesHipofisis 7RafaelPetitNo ratings yet
- JPM 12 01451 v2Document7 pagesJPM 12 01451 v2Nenad VujosevicNo ratings yet
- Role of Dexmedetomidine Infusion After Coronary Artery Bypass GraftingDocument6 pagesRole of Dexmedetomidine Infusion After Coronary Artery Bypass GraftingWidya KusumaNo ratings yet
- Dexmedetomidine Administration During Brain Tumour Resection andDocument2 pagesDexmedetomidine Administration During Brain Tumour Resection andABRAHAM MANUEL MEDINA LEYTONNo ratings yet
- Current and Emerging Treatment Strategies For Duchenne Muscular DystrophyDocument14 pagesCurrent and Emerging Treatment Strategies For Duchenne Muscular DystrophyANAMIKA ANANDINo ratings yet
- Hemodynamic Effects of Propofol and Dexmedetomidine in Septic Patients Without ShockDocument8 pagesHemodynamic Effects of Propofol and Dexmedetomidine in Septic Patients Without ShockSulindri IntanNo ratings yet
- Meyfroidt-Smith2019 Article FocusOnDeliriumSedationAndNeurDocument3 pagesMeyfroidt-Smith2019 Article FocusOnDeliriumSedationAndNeurmedicnanaNo ratings yet
- Articulo PrecedexDocument12 pagesArticulo PrecedexRicardo GarciaNo ratings yet
- Articulo 9 JulioDocument10 pagesArticulo 9 JulioPaloma AroliNo ratings yet
- Abdul-Razak Et Al. 2016 - DMD Gene TherapyDocument7 pagesAbdul-Razak Et Al. 2016 - DMD Gene TherapyVassili CrispiNo ratings yet
- Midazolan Intranasal en AdultoDocument10 pagesMidazolan Intranasal en Adultoheiddy MendozaNo ratings yet
- Clinical Features of COVID-19 PatientsDocument9 pagesClinical Features of COVID-19 PatientsCITRA AYU APRILIANo ratings yet
- Molnupiravir Non-Hospitalised Patients EVIDoa2100043Document10 pagesMolnupiravir Non-Hospitalised Patients EVIDoa2100043Doug StevensNo ratings yet
- Donepezil and Life Expectancy in Alzheimer's DiseaseDocument6 pagesDonepezil and Life Expectancy in Alzheimer's DiseaseDian GbligNo ratings yet
- Dexmedetomidine As An Adjunct For Sedation in Patients With Traumatic Brain InjuryDocument7 pagesDexmedetomidine As An Adjunct For Sedation in Patients With Traumatic Brain InjuryMárcia SanchesNo ratings yet
- Aapm 11 3 113802Document7 pagesAapm 11 3 113802kawaii fullmoonNo ratings yet
- NDT 12 1795 PDFDocument13 pagesNDT 12 1795 PDFAdrian KhomanNo ratings yet
- Use of Dexmedetomidine As A Sedative and Analgesic Agent in Critically Ill Adult Patients: A Meta-AnalysisDocument14 pagesUse of Dexmedetomidine As A Sedative and Analgesic Agent in Critically Ill Adult Patients: A Meta-AnalysisPatty Alarcón ParraNo ratings yet
- PLDD PublicationIrangroupDocument9 pagesPLDD PublicationIrangroupYAŞAR TÜRKNo ratings yet
- 2022 Article 3764Document16 pages2022 Article 3764LSGNo ratings yet
- Molecules 27 071103Document29 pagesMolecules 27 071103sorin.morosan64No ratings yet
- Conservative Management Spontaneous Subarachnoid Hemorrhage Grade IV: A Case ReportDocument3 pagesConservative Management Spontaneous Subarachnoid Hemorrhage Grade IV: A Case ReportRatna mellaNo ratings yet
- Effect of Intravenous Dexmedetomidine Infusion On Some Proinflammatory Cytokines Stress Hormones and Recovery Profile in Major Abdominal SurgeryDocument7 pagesEffect of Intravenous Dexmedetomidine Infusion On Some Proinflammatory Cytokines Stress Hormones and Recovery Profile in Major Abdominal SurgeryFitra HayatiNo ratings yet
- High-Dose Midazolam Infusion ForDocument7 pagesHigh-Dose Midazolam Infusion Forbobobo22No ratings yet
- Delirium After Deep Brain Stimulation in Parkinson's DiseaseDocument10 pagesDelirium After Deep Brain Stimulation in Parkinson's DiseaseMikeVDCNo ratings yet
- Fmed 08 645975Document16 pagesFmed 08 645975Ana Belén Artero CastañoNo ratings yet
- Metformin in Patients With Type 2 Diabetes Mellitus and Heart Failure: A ReviewDocument10 pagesMetformin in Patients With Type 2 Diabetes Mellitus and Heart Failure: A ReviewShaeli MalikNo ratings yet
- Anesth Analg 2019 129 6 1504-11Document8 pagesAnesth Analg 2019 129 6 1504-11Fernando SousaNo ratings yet
- Dexmedetomidine Nasal Administration Improves Perioperative Sleep Quality and Neurocognitive Deficits in Elderly Patients Undergoing General AnesthesiaBMC AnesthesiologyDocument10 pagesDexmedetomidine Nasal Administration Improves Perioperative Sleep Quality and Neurocognitive Deficits in Elderly Patients Undergoing General AnesthesiaBMC AnesthesiologyFrancisco Javier Diaz PincheiraNo ratings yet
- Postoperative Cognitive Dysfunction: Ingrid RundshagenDocument7 pagesPostoperative Cognitive Dysfunction: Ingrid RundshagenfaisaldanyaniNo ratings yet
- C C P L U: Ritical ARE Harmacotherapy Iterature PdateDocument9 pagesC C P L U: Ritical ARE Harmacotherapy Iterature PdateIgnacio NamuncuraNo ratings yet
- Propofol Versus Dexmedetomidine in Reducing Emergence Agitation After Sevoflurane AnaesthesiaDocument4 pagesPropofol Versus Dexmedetomidine in Reducing Emergence Agitation After Sevoflurane AnaesthesiaBIOMEDSCIDIRECT PUBLICATIONSNo ratings yet
- Deep Brain Stimulation in TheDocument17 pagesDeep Brain Stimulation in Thefelix08121992No ratings yet
- A Comparison of Methylprednisolone and Dexamethasone in Intensive Care Patients With COVID-19Document22 pagesA Comparison of Methylprednisolone and Dexamethasone in Intensive Care Patients With COVID-19SupriNo ratings yet
- Sino-Orbital Mucormycosis in A COVID-19 Patient: A Case ReportDocument5 pagesSino-Orbital Mucormycosis in A COVID-19 Patient: A Case Reportkarol castellonNo ratings yet
- Effectiveness of Bolus Administration of Continuous Intravenous Lidocaine On Pain Intensity After Mastectomy SurgeryDocument6 pagesEffectiveness of Bolus Administration of Continuous Intravenous Lidocaine On Pain Intensity After Mastectomy SurgeryInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Diagnostics 12 02064Document25 pagesDiagnostics 12 02064dptofisicaflorestaNo ratings yet
- Myocardial Risk As Preventive MedicineDocument18 pagesMyocardial Risk As Preventive MedicineSathvick BatchuNo ratings yet
- Mitochondrial Disease and Anesthesia: Vincent C. Hsieh, MD, Elliot J. Krane, MD, and Philip G. Morgan, MDDocument5 pagesMitochondrial Disease and Anesthesia: Vincent C. Hsieh, MD, Elliot J. Krane, MD, and Philip G. Morgan, MDJZNo ratings yet
- Cancer Pain Management: Opioid Analgesics, Part 2Document20 pagesCancer Pain Management: Opioid Analgesics, Part 2azkiel fikrieNo ratings yet
- Commentary: Digoxin in Chronic Heart Failure: Possibility of A Second Chance?Document3 pagesCommentary: Digoxin in Chronic Heart Failure: Possibility of A Second Chance?Della Puspita SariNo ratings yet
- WJCCM 11 33Document8 pagesWJCCM 11 33medicshinobiNo ratings yet
- Tugas Jurnal 3Document9 pagesTugas Jurnal 3Aulia Putri ANo ratings yet
- Surve Rohini 2016Document7 pagesSurve Rohini 2016Amro MahmoudNo ratings yet
- Biomarkers in Traumatic Brain Injury (Tbi) : A Review: Neuropsychiatric Disease and Treatment DoveDocument12 pagesBiomarkers in Traumatic Brain Injury (Tbi) : A Review: Neuropsychiatric Disease and Treatment DoveShafira WidiaNo ratings yet
- Dermatologic Therapy - 2021 - Melo - Frontal Edema Due To Mesotherapy For Androgenetic Alopecia A Case SeriesDocument3 pagesDermatologic Therapy - 2021 - Melo - Frontal Edema Due To Mesotherapy For Androgenetic Alopecia A Case SeriesAlejandra BenavidezNo ratings yet
- DDDT 14 4695Document7 pagesDDDT 14 4695IvanGómezNo ratings yet
- Advcance Neuroimaging GlioblastomaDocument19 pagesAdvcance Neuroimaging Glioblastomaafdhal.888980No ratings yet
- BPA 32 E13062Document12 pagesBPA 32 E13062Jessica MiakeNo ratings yet
- 5 Ijca - 3 (2) - 316-323Document8 pages5 Ijca - 3 (2) - 316-323Mythology KingdomNo ratings yet
- What 'S New in The Treatment of Migraine?: Kathleen B. Digre, MDDocument8 pagesWhat 'S New in The Treatment of Migraine?: Kathleen B. Digre, MDFábio JrNo ratings yet
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19From EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19No ratings yet
- Nanomedicine and Cancer Research And Textbook 5From EverandNanomedicine and Cancer Research And Textbook 5No ratings yet
- Science 7 DLP q3w9d4 & w10d1Document4 pagesScience 7 DLP q3w9d4 & w10d1Tammy SelaromNo ratings yet
- Posi BraceDocument2 pagesPosi BraceBenNo ratings yet
- Assessing The Feasibility of Achieving Functional Recovery Goals Through Seismic Retrofit of Existing Reinforced Concrete BuildingsEarthquake SpectraDocument29 pagesAssessing The Feasibility of Achieving Functional Recovery Goals Through Seismic Retrofit of Existing Reinforced Concrete BuildingsEarthquake SpectraRay CTNo ratings yet
- CHARCUTERIE and FORCEMEATDocument4 pagesCHARCUTERIE and FORCEMEATCheska PatduNo ratings yet
- FAHM 2018 Programme v4Document16 pagesFAHM 2018 Programme v4Aviation Events InternationalNo ratings yet
- 1.smart Light, Temperature, Air Condition ControlDocument4 pages1.smart Light, Temperature, Air Condition ControlFatin Nur Syahirah AzharNo ratings yet
- Jurnal EntropionDocument7 pagesJurnal EntropionOgiesilaenNo ratings yet
- An Alien HandDocument3 pagesAn Alien HandRini Sanjay PanikarNo ratings yet
- Red PandaDocument24 pagesRed PandaDaphne Tan 丽文50% (2)
- Steel Estimate-DeskDocument9 pagesSteel Estimate-Desksaiful islamNo ratings yet
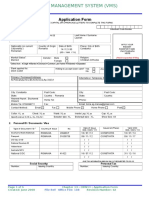
- Vships Application FormDocument6 pagesVships Application FormToma MariusNo ratings yet
- Activity No. 4 Amino Acids and ProteinsDocument6 pagesActivity No. 4 Amino Acids and ProteinsAngel EspanolNo ratings yet
- Should We Encourage Research and Practice On Human CloningDocument3 pagesShould We Encourage Research and Practice On Human CloningMark Anthony Dela Cruz100% (1)
- Call For Papers-International Journal of Wireless & Mobile Networks (IJWMN)Document2 pagesCall For Papers-International Journal of Wireless & Mobile Networks (IJWMN)John BergNo ratings yet
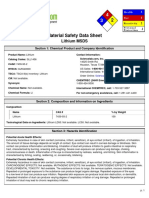
- Msds LiDocument5 pagesMsds Linaren_013No ratings yet
- Gepard M6 .50BMG RifleDocument9 pagesGepard M6 .50BMG RifleGautam Natrajan100% (1)
- Group 4: Diet For Healthy Teath BonesDocument26 pagesGroup 4: Diet For Healthy Teath Bonesknowledge chanall chanallNo ratings yet
- Streamwood Community Newsletter, May 2024Document8 pagesStreamwood Community Newsletter, May 2024scaddiganNo ratings yet
- Generator Breaker Equipped With Vacuum InterruptersDocument4 pagesGenerator Breaker Equipped With Vacuum InterruptersVenna Karthik ReddyNo ratings yet
- Read The Text Carefully and Then Answer The Questions That Follow! Floods Force Thousands of People To Evacuate in GorontaloDocument2 pagesRead The Text Carefully and Then Answer The Questions That Follow! Floods Force Thousands of People To Evacuate in GorontaloDella SagitaNo ratings yet
- Grade 6 - Worksheet - Mid Term ExamDocument3 pagesGrade 6 - Worksheet - Mid Term ExamSharmila Kumari RNo ratings yet
- Electrix TweakerDocument1 pageElectrix TweakerUSER58679No ratings yet
- Concrete Construction Article PDF - Quality Control in Concrete ConstructionDocument3 pagesConcrete Construction Article PDF - Quality Control in Concrete ConstructionJeremiah ObiacoroNo ratings yet
- PC Bahasa Inggris UPK 22.Document16 pagesPC Bahasa Inggris UPK 22.Blackes HoleNo ratings yet
- Kukko CatalogueDocument109 pagesKukko CatalogueAlexandre Anderson AlvesNo ratings yet
- FUFENG-AF 80 Xanthan Gum SDSDocument6 pagesFUFENG-AF 80 Xanthan Gum SDSDheyne TellesNo ratings yet
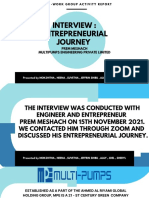
- Mba Group ActivityDocument14 pagesMba Group ActivitySHERYL SHEKINAH E ARCH-2019 BATCHNo ratings yet