You might also like
- Diagnostics 13 00068Document23 pagesDiagnostics 13 00068MOHAMED IRREEF SNo ratings yet
- Bacterial Brain Abscess: An Outline For Diagnosis and ManagementDocument10 pagesBacterial Brain Abscess: An Outline For Diagnosis and ManagementWIWI HRNo ratings yet
- FCVM 09 1022658Document20 pagesFCVM 09 1022658francogarciaramirez1No ratings yet
- Wa0006.Document13 pagesWa0006.rafggajhNo ratings yet
- Healthcare 11 01803Document25 pagesHealthcare 11 01803Trang PhạmNo ratings yet
- International Journal of Gerontology: Gwo-Chi Hu, Yi-Min ChenDocument5 pagesInternational Journal of Gerontology: Gwo-Chi Hu, Yi-Min Chenluthfia ayu az zahraNo ratings yet
- Healthcare Analytics: Sheida Jabbedari Khiabani, Atefeh Batani, Ehsan KhanmohammadiDocument12 pagesHealthcare Analytics: Sheida Jabbedari Khiabani, Atefeh Batani, Ehsan Khanmohammadiharshitvashisth76No ratings yet
- Life 13 00024Document16 pagesLife 13 00024dmandatari7327No ratings yet
- Heart Attack Risk Prediction Plag Check PDFDocument49 pagesHeart Attack Risk Prediction Plag Check PDFRahul JhaNo ratings yet
- Sensors 22 04670Document13 pagesSensors 22 04670hiimamanenuNo ratings yet
- Detection of Heart Attacks Using Machine LearningDocument9 pagesDetection of Heart Attacks Using Machine LearningIJRASETPublicationsNo ratings yet
- Heart Disease Prediction Using Bio Inspired AlgorithmsDocument7 pagesHeart Disease Prediction Using Bio Inspired Algorithmssanthoshrao19No ratings yet
- Biology: A Comprehensive Survey On The Detection, Classification, and Challenges of Neurological DisordersDocument45 pagesBiology: A Comprehensive Survey On The Detection, Classification, and Challenges of Neurological Disorders1205김민준No ratings yet
- Medi 97 E10919Document4 pagesMedi 97 E10919oktaviaNo ratings yet
- Performance Analysis of Some Se-Lected Machine Learning Algo - Rithms On Heart Disease Predic - Tion Using The Noble Uci DatasetsDocument11 pagesPerformance Analysis of Some Se-Lected Machine Learning Algo - Rithms On Heart Disease Predic - Tion Using The Noble Uci DatasetssanketNo ratings yet
- Heart Disease Prediction Using Effective Machine Learning TechniquesDocument7 pagesHeart Disease Prediction Using Effective Machine Learning Techniquesdr mbaluNo ratings yet
- Journal Pdig 0000012-2Document20 pagesJournal Pdig 0000012-2Liu KenNo ratings yet
- Coronary Illness Hazard Prediction Using Machine Learning (CIHPML)Document6 pagesCoronary Illness Hazard Prediction Using Machine Learning (CIHPML)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Ischemic Stroke A Comparative Retrospective Study: Experience of Military Hospital of MeknesDocument20 pagesIschemic Stroke A Comparative Retrospective Study: Experience of Military Hospital of MeknesIJAR JOURNALNo ratings yet
- Assessing The Severity of Traumatic Brain Injury-Time For A Change?Document12 pagesAssessing The Severity of Traumatic Brain Injury-Time For A Change?Anonymous R6ex8BM0No ratings yet
- Diagnostics 12 02541 With CoverDocument20 pagesDiagnostics 12 02541 With CoverasadprlNo ratings yet
- Correlation of ECG Values To The Behavior of Heart Attack SufferersDocument6 pagesCorrelation of ECG Values To The Behavior of Heart Attack SufferersIJRASETPublicationsNo ratings yet
- Brainsci 11 01171 v2Document25 pagesBrainsci 11 01171 v2Vaibhav BahelNo ratings yet
- Healthcare: Machine-Learning-Based Disease Diagnosis: A Comprehensive ReviewDocument30 pagesHealthcare: Machine-Learning-Based Disease Diagnosis: A Comprehensive ReviewMuhammad WasifNo ratings yet
- 1 s2.0 S0933365722001129 MainDocument12 pages1 s2.0 S0933365722001129 MainNaila AshrafNo ratings yet
- Treatment Efficacy and Risk Factors of NeurobrucellosisDocument8 pagesTreatment Efficacy and Risk Factors of NeurobrucellosisMiguel Pinedo TrujilloNo ratings yet
- Biomarkers in Traumatic Brain Injury (Tbi) : A Review: Neuropsychiatric Disease and Treatment DoveDocument12 pagesBiomarkers in Traumatic Brain Injury (Tbi) : A Review: Neuropsychiatric Disease and Treatment DoveShafira WidiaNo ratings yet
- Treatments in Ischemic StrokeDocument18 pagesTreatments in Ischemic StrokeFercho MedNo ratings yet
- (23005319 - Acta Mechanica Et Automatica) Attribute Selection For Stroke PredictionDocument5 pages(23005319 - Acta Mechanica Et Automatica) Attribute Selection For Stroke PredictionSolomonNo ratings yet
- Book StrokeDocument196 pagesBook Strokemadalena limaNo ratings yet
- IOT Based Heart Disease PredictionDocument4 pagesIOT Based Heart Disease PredictionIJRASETPublicationsNo ratings yet
- Mortality Prediction Gets A "Boost" : P 0.010) - A Cox Regression Model Using A Time-DependentDocument2 pagesMortality Prediction Gets A "Boost" : P 0.010) - A Cox Regression Model Using A Time-DependentJayron SoaresNo ratings yet
- Faizal 2021Document11 pagesFaizal 2021muhammad sajidNo ratings yet
- 2022 - Retinal Imaging in Alzheimer's Disease - Special ArticleDocument10 pages2022 - Retinal Imaging in Alzheimer's Disease - Special Articlepooja barakNo ratings yet
- Stroke Prevention Modifying Risk FactorsDocument21 pagesStroke Prevention Modifying Risk FactorsEchezonaNo ratings yet
- Prevalence of Stroke in The Elderly A Systematic Review and Meta-AnalysisDocument10 pagesPrevalence of Stroke in The Elderly A Systematic Review and Meta-AnalysisMarian J. NietoNo ratings yet
- Microsoft Word - Paper 2021 PDFDocument4 pagesMicrosoft Word - Paper 2021 PDFSumati BaralNo ratings yet
- Finding The Influential Clinical Traits That Impact On The Diagnosis of Heart Disease Using Statistical and Machine Learning TechniquesDocument11 pagesFinding The Influential Clinical Traits That Impact On The Diagnosis of Heart Disease Using Statistical and Machine Learning TechniquesLexandrine GBNo ratings yet
- JCM 10 05912Document8 pagesJCM 10 05912Sandara SamperNo ratings yet
- Diagnosis of Cardiovascular Disease Using Deep LearningDocument10 pagesDiagnosis of Cardiovascular Disease Using Deep LearningIJRASETPublicationsNo ratings yet
- V8i5 1245Document4 pagesV8i5 1245Raunak SoniNo ratings yet
- A Blood-Based Biomarker Panel To Risk-Stratify Mild Traumatic Brain InjuryDocument18 pagesA Blood-Based Biomarker Panel To Risk-Stratify Mild Traumatic Brain InjuryNurul FajriNo ratings yet
- Effect of Photobiomodulation in MultiplesclerosisDocument4 pagesEffect of Photobiomodulation in MultiplesclerosisMuhammad Imam NoorNo ratings yet
- Medical RisksDocument8 pagesMedical RisksAnonymous krQNhsf5No ratings yet
- Nihms 1510131Document59 pagesNihms 1510131ikokalariNo ratings yet
- Big Data Analytics in Heart Attack Prediction 2167 1168 1000393Document9 pagesBig Data Analytics in Heart Attack Prediction 2167 1168 1000393jagadeeswara71No ratings yet
- Time Is Brain: Assessing Emergency Healthcare Workers Knowledge of Early Recognition of Stroke and Warning SignsDocument6 pagesTime Is Brain: Assessing Emergency Healthcare Workers Knowledge of Early Recognition of Stroke and Warning SignsIJAR JOURNALNo ratings yet
- Mobile Psychiatry: Towards Improving The Care For Bipolar DisorderDocument10 pagesMobile Psychiatry: Towards Improving The Care For Bipolar DisorderGustavoNo ratings yet
- Safri 2018 IOP Conf. Ser. Earth Environ. Sci. 125 012125Document7 pagesSafri 2018 IOP Conf. Ser. Earth Environ. Sci. 125 012125Renoldy PapilayaNo ratings yet
- Machine_Learning-Based_Cardiovascular_Disease_Detection_Using_Optimal_Feature_SelectionDocument16 pagesMachine_Learning-Based_Cardiovascular_Disease_Detection_Using_Optimal_Feature_Selectiontutusir1987No ratings yet
- 7 Stroke 2022Document5 pages7 Stroke 2022Vanesa Rubí CamposNo ratings yet
- Pone 0211599Document12 pagesPone 0211599HILA GINANo ratings yet
- 1 s2.0 S1532046420302768 MainDocument10 pages1 s2.0 S1532046420302768 MainDenzo NaldaNo ratings yet
- Identificacion Choque Cardiogenico ERDocument9 pagesIdentificacion Choque Cardiogenico ERZai RojasNo ratings yet
- Precondicionando El Cerebro Nueva Frontera en Neuroterapeutica Stroke 2012Document15 pagesPrecondicionando El Cerebro Nueva Frontera en Neuroterapeutica Stroke 2012jgcardNo ratings yet
- Role of Artificial Intelligence in Kidney DiseaseDocument15 pagesRole of Artificial Intelligence in Kidney Diseasegta game playNo ratings yet
- Adherence To Cardiovascular Therapy: A Meta-Analysis of Prevalence and Clinical ConsequencesDocument9 pagesAdherence To Cardiovascular Therapy: A Meta-Analysis of Prevalence and Clinical Consequencesdaniela NeculmanNo ratings yet
- Artifcial Intelligence and Machine Learning in Precision and GenomicDocument18 pagesArtifcial Intelligence and Machine Learning in Precision and GenomicAditya DebnathNo ratings yet
- 1 s2.0 S0950705112001840 MainDocument13 pages1 s2.0 S0950705112001840 Main1201200152No ratings yet
- Digital Design Lab Report ExperimentsDocument9 pagesDigital Design Lab Report ExperimentsSathvick BatchuNo ratings yet
- Trips Hotel DownloadETicketDocument1 pageTrips Hotel DownloadETicketSathvick BatchuNo ratings yet
- Vinay ResumeDocument1 pageVinay ResumeSathvick BatchuNo ratings yet
- Hindi Intent ClassificationDocument12 pagesHindi Intent ClassificationSathvick Batchu100% (1)
- Seminar ReportDocument2 pagesSeminar ReportSathvick BatchuNo ratings yet
- Assignment 2Document6 pagesAssignment 2Sathvick BatchuNo ratings yet
- Deep Learning For Detecting and Locating Myocardial Infarction by Electrocardiogram - A Literature ReviewDocument28 pagesDeep Learning For Detecting and Locating Myocardial Infarction by Electrocardiogram - A Literature ReviewSathvick BatchuNo ratings yet
- Automated Detection of Myocardial InfarctionDocument14 pagesAutomated Detection of Myocardial InfarctionSathvick BatchuNo ratings yet
- Hindi Intent ClassificationDocument13 pagesHindi Intent ClassificationSathvick BatchuNo ratings yet
- ProfileDocument1 pageProfileSathvick BatchuNo ratings yet
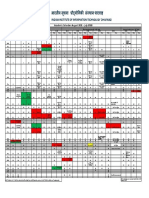
- Academic Calendar: August 2021 - July 2022Document1 pageAcademic Calendar: August 2021 - July 2022Sathvick BatchuNo ratings yet
- Hybrid LSTM CNNDocument19 pagesHybrid LSTM CNNSathvick BatchuNo ratings yet
- Happiness Frequency SurveyDocument6 pagesHappiness Frequency SurveySathvick BatchuNo ratings yet
- Dr. Manjusha C B: Manjusha@iiitdwd - Ac.inDocument9 pagesDr. Manjusha C B: Manjusha@iiitdwd - Ac.inSathvick BatchuNo ratings yet
- Nataraj K S: DucationDocument3 pagesNataraj K S: DucationSathvick BatchuNo ratings yet
- Indian Aviation Industry Statistics and New TechnologyDocument34 pagesIndian Aviation Industry Statistics and New TechnologySathvick BatchuNo ratings yet
- DSP Lab RecordDocument37 pagesDSP Lab RecordSathvick BatchuNo ratings yet
- Scilab Textbook Companion for Linear Integrated CircuitsDocument76 pagesScilab Textbook Companion for Linear Integrated CircuitsSathvick BatchuNo ratings yet
- Movie Recommendation ReportDocument14 pagesMovie Recommendation ReportSathvick BatchuNo ratings yet
- Score Predicting The Need For Hospitalization in Scorpion EnvenomationDocument7 pagesScore Predicting The Need For Hospitalization in Scorpion EnvenomationWalaa YousefNo ratings yet
- Zhang Et Al. - 2022 - A Multi-Channel Deep Convolutional Neural NetworkDocument11 pagesZhang Et Al. - 2022 - A Multi-Channel Deep Convolutional Neural NetworkJamesLeeNo ratings yet
- Criterion and Concurrent Validity of Conners Adult Adhd Diagnostic Interview For Dsm-Iv (Caadid) SpanishDocument7 pagesCriterion and Concurrent Validity of Conners Adult Adhd Diagnostic Interview For Dsm-Iv (Caadid) SpanishG OrangeNo ratings yet
- System: Customer Service United States: 1-877-4ABBOTT International: Call Your Abbott RepresentativeDocument7 pagesSystem: Customer Service United States: 1-877-4ABBOTT International: Call Your Abbott Representativetesteste testeNo ratings yet
- Ann CripsDocument5 pagesAnn CripssuryaNo ratings yet
- Precision and Accuracy in ATP Hygiene TestingDocument3 pagesPrecision and Accuracy in ATP Hygiene TestingGaganpreet KaurNo ratings yet
- Weighing The Merits of The Wagner SystemDocument8 pagesWeighing The Merits of The Wagner SystemSonish KhatriNo ratings yet
- Code Practice ASP SystemsDocument72 pagesCode Practice ASP SystemsmohammadNo ratings yet
- Calibration of Helium Leak Detectors by Use of Secondary StandardsDocument7 pagesCalibration of Helium Leak Detectors by Use of Secondary StandardsCarlos SaldanaNo ratings yet
- Discovery 3.0 Litre V6 Diesel (10my Eu5) On-Board Diagnostics Engine Management SystemDocument70 pagesDiscovery 3.0 Litre V6 Diesel (10my Eu5) On-Board Diagnostics Engine Management SystemVladimirAgeevNo ratings yet
- Classification EvaluationDocument28 pagesClassification EvaluationKathy KgNo ratings yet
- Noninvasive Evaluation of Liver FibrosisDocument70 pagesNoninvasive Evaluation of Liver FibrosisiriscelNo ratings yet
- Principles of Analytical Method ValidationDocument34 pagesPrinciples of Analytical Method ValidationAce Alberca100% (2)
- A Comparison of Emergence Delirium Scales Following General Anesthesia in ChildrenDocument8 pagesA Comparison of Emergence Delirium Scales Following General Anesthesia in ChildrenNongnapat KettungmunNo ratings yet
- USMLE Epidemiology and BiostatisticsDocument30 pagesUSMLE Epidemiology and Biostatisticsamir ali100% (1)
- Journal of Clinical and Experimental Neuropsychology: Merve Çebi, Gülsen Babacan, Öget Öktem Tanör & Hakan GürvitDocument10 pagesJournal of Clinical and Experimental Neuropsychology: Merve Çebi, Gülsen Babacan, Öget Öktem Tanör & Hakan GürvitDR RISKA WAHYUNo ratings yet
- Model Perf Cheat SheetDocument2 pagesModel Perf Cheat SheetvinodhewardsNo ratings yet
- Nirvana Intrinsic Trend ModuleDocument25 pagesNirvana Intrinsic Trend ModuleLucky ChopraNo ratings yet
- Artificial Intelligence Assisted Potato Disease DetectionDocument15 pagesArtificial Intelligence Assisted Potato Disease DetectionTefeNo ratings yet
- Errors, Omissions and Infelicities in Broadcast InterpretingDocument20 pagesErrors, Omissions and Infelicities in Broadcast InterpretingDario Matteo Sparanero100% (1)
- PET Performance Measurements Using The NEMA NU 2-2001 StandardDocument12 pagesPET Performance Measurements Using The NEMA NU 2-2001 StandardCiro LeonNo ratings yet
- Bioepi Finals Module 5Document84 pagesBioepi Finals Module 5Jamie SalvadorNo ratings yet
- Neet Preventive & Social MedicineDocument871 pagesNeet Preventive & Social Medicinewilliamsjoseff0No ratings yet
- UntitledDocument311 pagesUntitledDjbr MohNo ratings yet
- EpidemiologyDocument16 pagesEpidemiologyKatina CamposNo ratings yet
- Speis Tradia Neo ReviewDocument18 pagesSpeis Tradia Neo ReviewGunther OrosNo ratings yet
- Version FinalDocument12 pagesVersion FinalMaria Fernanda BahamondezNo ratings yet
- Cleland Et. Al. (2009) - CPR para MobilizaDocument15 pagesCleland Et. Al. (2009) - CPR para MobilizaFrancieleNo ratings yet
- Ss 5Document13 pagesSs 5Ahmed QasimNo ratings yet
- Chamberlin 2021Document14 pagesChamberlin 2021EthanNo ratings yet
- ChatGPT Millionaire 2024 - Bot-Driven Side Hustles, Prompt Engineering Shortcut Secrets, and Automated Income Streams that Print Money While You Sleep. The Ultimate Beginner’s Guide for AI BusinessFrom EverandChatGPT Millionaire 2024 - Bot-Driven Side Hustles, Prompt Engineering Shortcut Secrets, and Automated Income Streams that Print Money While You Sleep. The Ultimate Beginner’s Guide for AI BusinessNo ratings yet
- Scary Smart: The Future of Artificial Intelligence and How You Can Save Our WorldFrom EverandScary Smart: The Future of Artificial Intelligence and How You Can Save Our WorldRating: 4.5 out of 5 stars4.5/5 (55)
- ChatGPT Side Hustles 2024 - Unlock the Digital Goldmine and Get AI Working for You Fast with More Than 85 Side Hustle Ideas to Boost Passive Income, Create New Cash Flow, and Get Ahead of the CurveFrom EverandChatGPT Side Hustles 2024 - Unlock the Digital Goldmine and Get AI Working for You Fast with More Than 85 Side Hustle Ideas to Boost Passive Income, Create New Cash Flow, and Get Ahead of the CurveNo ratings yet
- Generative AI: The Insights You Need from Harvard Business ReviewFrom EverandGenerative AI: The Insights You Need from Harvard Business ReviewRating: 4.5 out of 5 stars4.5/5 (2)
- Artificial Intelligence: The Insights You Need from Harvard Business ReviewFrom EverandArtificial Intelligence: The Insights You Need from Harvard Business ReviewRating: 4.5 out of 5 stars4.5/5 (104)
- Mastering Large Language Models: Advanced techniques, applications, cutting-edge methods, and top LLMs (English Edition)From EverandMastering Large Language Models: Advanced techniques, applications, cutting-edge methods, and top LLMs (English Edition)No ratings yet
- ChatGPT Money Machine 2024 - The Ultimate Chatbot Cheat Sheet to Go From Clueless Noob to Prompt Prodigy Fast! Complete AI Beginner’s Course to Catch the GPT Gold Rush Before It Leaves You BehindFrom EverandChatGPT Money Machine 2024 - The Ultimate Chatbot Cheat Sheet to Go From Clueless Noob to Prompt Prodigy Fast! Complete AI Beginner’s Course to Catch the GPT Gold Rush Before It Leaves You BehindNo ratings yet
- AI Money Machine: Unlock the Secrets to Making Money Online with AIFrom EverandAI Money Machine: Unlock the Secrets to Making Money Online with AINo ratings yet
- The Master Algorithm: How the Quest for the Ultimate Learning Machine Will Remake Our WorldFrom EverandThe Master Algorithm: How the Quest for the Ultimate Learning Machine Will Remake Our WorldRating: 4.5 out of 5 stars4.5/5 (107)
- Who's Afraid of AI?: Fear and Promise in the Age of Thinking MachinesFrom EverandWho's Afraid of AI?: Fear and Promise in the Age of Thinking MachinesRating: 4.5 out of 5 stars4.5/5 (13)
- Midjourney Mastery - The Ultimate Handbook of PromptsFrom EverandMidjourney Mastery - The Ultimate Handbook of PromptsRating: 4.5 out of 5 stars4.5/5 (2)
- Artificial Intelligence: A Guide for Thinking HumansFrom EverandArtificial Intelligence: A Guide for Thinking HumansRating: 4.5 out of 5 stars4.5/5 (30)
- Power and Prediction: The Disruptive Economics of Artificial IntelligenceFrom EverandPower and Prediction: The Disruptive Economics of Artificial IntelligenceRating: 4.5 out of 5 stars4.5/5 (38)
- Artificial Intelligence: The Complete Beginner’s Guide to the Future of A.I.From EverandArtificial Intelligence: The Complete Beginner’s Guide to the Future of A.I.Rating: 4 out of 5 stars4/5 (15)
- The AI Advantage: How to Put the Artificial Intelligence Revolution to WorkFrom EverandThe AI Advantage: How to Put the Artificial Intelligence Revolution to WorkRating: 4 out of 5 stars4/5 (7)
- 100M Offers Made Easy: Create Your Own Irresistible Offers by Turning ChatGPT into Alex HormoziFrom Everand100M Offers Made Easy: Create Your Own Irresistible Offers by Turning ChatGPT into Alex HormoziNo ratings yet
- 2084: Artificial Intelligence and the Future of HumanityFrom Everand2084: Artificial Intelligence and the Future of HumanityRating: 4 out of 5 stars4/5 (81)
- Machine Learning: The Ultimate Beginner's Guide to Learn Machine Learning, Artificial Intelligence & Neural Networks Step by StepFrom EverandMachine Learning: The Ultimate Beginner's Guide to Learn Machine Learning, Artificial Intelligence & Neural Networks Step by StepRating: 4.5 out of 5 stars4.5/5 (19)
- Demystifying Prompt Engineering: AI Prompts at Your Fingertips (A Step-By-Step Guide)From EverandDemystifying Prompt Engineering: AI Prompts at Your Fingertips (A Step-By-Step Guide)Rating: 4 out of 5 stars4/5 (1)
- AI and Machine Learning for Coders: A Programmer's Guide to Artificial IntelligenceFrom EverandAI and Machine Learning for Coders: A Programmer's Guide to Artificial IntelligenceRating: 4 out of 5 stars4/5 (2)
- 100+ Amazing AI Image Prompts: Expertly Crafted Midjourney AI Art Generation ExamplesFrom Everand100+ Amazing AI Image Prompts: Expertly Crafted Midjourney AI Art Generation ExamplesNo ratings yet
- Make Money with ChatGPT: Your Guide to Making Passive Income Online with Ease using AI: AI Wealth MasteryFrom EverandMake Money with ChatGPT: Your Guide to Making Passive Income Online with Ease using AI: AI Wealth MasteryNo ratings yet
- 1200+ AI Prompts for Everyone.: Artificial Intelligence Prompt Library.From Everand1200+ AI Prompts for Everyone.: Artificial Intelligence Prompt Library.No ratings yet