You might also like
- Upper Extremity Arterial Protocol 14Document3 pagesUpper Extremity Arterial Protocol 14api-349402240No ratings yet
- LSB658 Clinical PhysiologyDocument27 pagesLSB658 Clinical PhysiologyTess100% (1)
- Underground Clinical Vignettes - Pathophysiology I PDFDocument124 pagesUnderground Clinical Vignettes - Pathophysiology I PDFtwinkle000100% (2)
- Cryptogenic StrokeDocument52 pagesCryptogenic Strokemrabhilekh100% (1)
- Case Presentation On Coronary Artery Disease - 090908Document54 pagesCase Presentation On Coronary Artery Disease - 090908Parth Vasave100% (3)
- 2014 Myocardial Tech Guide PDFDocument128 pages2014 Myocardial Tech Guide PDFSuad ŠataraNo ratings yet
- Manual of NeurosonologyDocument334 pagesManual of NeurosonologyBelen100% (3)
- CHN Non Communicable Diseases and OthersDocument90 pagesCHN Non Communicable Diseases and OthersEllenare Racion100% (1)
- Heart Disease, Ascorbate, Lysine and Linus Pauling by Jeffrey Dach MDDocument33 pagesHeart Disease, Ascorbate, Lysine and Linus Pauling by Jeffrey Dach MDEbook PDF100% (1)
- Computing and Visualization for Intravascular Imaging and Computer-Assisted StentingFrom EverandComputing and Visualization for Intravascular Imaging and Computer-Assisted StentingSimone BaloccoNo ratings yet
- A Hybrid Deep CNN Model For Abnormal Arrhythmia Detection Based On Cardiac ECG SignalDocument13 pagesA Hybrid Deep CNN Model For Abnormal Arrhythmia Detection Based On Cardiac ECG Signal弘元No ratings yet
- A Multitier Deep Learning Model For Arrhythmia DetectionDocument9 pagesA Multitier Deep Learning Model For Arrhythmia DetectionSahil TiwariNo ratings yet
- Remotesensing 12 01685 With Cover PDFDocument15 pagesRemotesensing 12 01685 With Cover PDFSusana MalleaNo ratings yet
- Hybrid LSTM CNNDocument19 pagesHybrid LSTM CNNSathvick BatchuNo ratings yet
- Entropy: ECG Signal Classification Using Deep Learning Techniques Based On The PTB-XL DatasetDocument20 pagesEntropy: ECG Signal Classification Using Deep Learning Techniques Based On The PTB-XL DatasetnadhemNo ratings yet
- MCA-net - A Multi-Task Channel Attention Network For Myocardial Infarction Detection and Location Using 12-Lead ECGsDocument12 pagesMCA-net - A Multi-Task Channel Attention Network For Myocardial Infarction Detection and Location Using 12-Lead ECGs施展No ratings yet
- Deep Learning For Detecting and Locating Myocardial Infarction by Electrocardiogram - A Literature ReviewDocument28 pagesDeep Learning For Detecting and Locating Myocardial Infarction by Electrocardiogram - A Literature ReviewSathvick BatchuNo ratings yet
- Electronics: Multiclass ECG Signal Analysis Using Global Average-Based 2-D Convolutional Neural Network ModelingDocument29 pagesElectronics: Multiclass ECG Signal Analysis Using Global Average-Based 2-D Convolutional Neural Network ModelingHoàng MạnhNo ratings yet
- Deep Learning Algorithm Classifies Heartbeat Events Based On Electrocardiogram SignalsDocument10 pagesDeep Learning Algorithm Classifies Heartbeat Events Based On Electrocardiogram Signalsaryelit velardesNo ratings yet
- 1 s2.0 S0169260722001134 MainDocument15 pages1 s2.0 S0169260722001134 MainBiomed BiomedNo ratings yet
- Arrhythmia Detection Using Deep Convolutional Neural Network With Long Duration ECG SignalsDocument11 pagesArrhythmia Detection Using Deep Convolutional Neural Network With Long Duration ECG SignalsMhd rdbNo ratings yet
- Remote Sensing: Classification of Arrhythmia by Using Deep Learning With 2-D ECG Spectral Image RepresentationDocument14 pagesRemote Sensing: Classification of Arrhythmia by Using Deep Learning With 2-D ECG Spectral Image RepresentationBhargav KodaliNo ratings yet
- Diagnosis of Cardiovascular Disease Using Deep LearningDocument10 pagesDiagnosis of Cardiovascular Disease Using Deep LearningIJRASETPublicationsNo ratings yet
- Unsupervised ECG Analysis A ReviewDocument17 pagesUnsupervised ECG Analysis A ReviewPedro RigueiraNo ratings yet
- Application of Deep Convolutional Neural Network For Automated Detection of Myocardial Infarction Using ECG SignalsDocument19 pagesApplication of Deep Convolutional Neural Network For Automated Detection of Myocardial Infarction Using ECG SignalsAlex LoezaNo ratings yet
- Entropy 23 00119Document13 pagesEntropy 23 00119Firas KACHROUDINo ratings yet
- AI CVD DiagnoseDocument17 pagesAI CVD DiagnoseBurak AcikgozNo ratings yet
- Sensors: Detection of Myocardial Infarction Using ECG and Multi-Scale Feature ConcatenateDocument17 pagesSensors: Detection of Myocardial Infarction Using ECG and Multi-Scale Feature ConcatenateAlex LoezaNo ratings yet
- Classifying Electrocardiograph Waveforms Using Trained Deep Learning Neural Network Based On Wavelet RepresentationDocument9 pagesClassifying Electrocardiograph Waveforms Using Trained Deep Learning Neural Network Based On Wavelet RepresentationIAES IJAINo ratings yet
- JCDD 10 00175Document16 pagesJCDD 10 00175ahmad smadiNo ratings yet
- Innovations in Stroke Identification A Machine Learning-Based Diagnostic Model Using NeuroimagesDocument11 pagesInnovations in Stroke Identification A Machine Learning-Based Diagnostic Model Using Neuroimagesgowthamnm.nieNo ratings yet
- Diagnostics 13 00068Document23 pagesDiagnostics 13 00068MOHAMED IRREEF SNo ratings yet
- Detection of Abnormal Electrocardiogram (ECG) Using Wavelet Decomposition and Support Vector Machine (SVM)Document9 pagesDetection of Abnormal Electrocardiogram (ECG) Using Wavelet Decomposition and Support Vector Machine (SVM)NuruddinEmonNo ratings yet
- TSP CMC 34400Document16 pagesTSP CMC 34400sahad adelmoumenNo ratings yet
- Healthcare 11 01000Document13 pagesHealthcare 11 01000silvalimaaf94No ratings yet
- An Efficient End-To-End Deep Neural Network For Interstitial LungDocument17 pagesAn Efficient End-To-End Deep Neural Network For Interstitial LungMuteen MunawarNo ratings yet
- Stroke Prediction System Using ANN (Artificial Neural Network)Document3 pagesStroke Prediction System Using ANN (Artificial Neural Network)International Journal of Innovative Science and Research TechnologyNo ratings yet
- Base PaperDocument10 pagesBase PaperPENTAMALLA HARIHARANNo ratings yet
- Artificial Intelligence in MedicineDocument8 pagesArtificial Intelligence in Medicinepuneet5246No ratings yet
- Enhanced Myocardial Infarction Identification in Phonocardiogram Signals Using Segmented Feature Extraction and Transfer Learning-Based ClassificationDocument12 pagesEnhanced Myocardial Infarction Identification in Phonocardiogram Signals Using Segmented Feature Extraction and Transfer Learning-Based Classificationbvkarthik2711No ratings yet
- Applsci 12 07592Document22 pagesApplsci 12 07592ahmet buğraNo ratings yet
- ArticlesDocument15 pagesArticlesSena TuncerNo ratings yet
- Research Article: Subha R., Anandakumar K and Bharathi ADocument7 pagesResearch Article: Subha R., Anandakumar K and Bharathi AyetsedawNo ratings yet
- Classification of Cardiac Disorders Based On Electrocardiogram Data Using A Decision Tree Classification Approach With The C45 AlgorithmDocument11 pagesClassification of Cardiac Disorders Based On Electrocardiogram Data Using A Decision Tree Classification Approach With The C45 AlgorithmIAES IJAINo ratings yet
- BiosensorsDocument19 pagesBiosensorsعلاء الدين العولقيNo ratings yet
- Detection and Classification of Leukemia Using Deep LearningDocument5 pagesDetection and Classification of Leukemia Using Deep LearningIJRASETPublicationsNo ratings yet
- Detection and Classification of Arrhythmia Using An Explainable Deep Learning ModelDocument9 pagesDetection and Classification of Arrhythmia Using An Explainable Deep Learning ModelComisión Académica FCM - UNAHNo ratings yet
- Prediction of Cardiovascular Disease Using Machine Learning AlgorithmsDocument11 pagesPrediction of Cardiovascular Disease Using Machine Learning AlgorithmsAnanya DhuriaNo ratings yet
- Classification of Ischemic Stroke Using Machine Learning AlgorithmsDocument6 pagesClassification of Ischemic Stroke Using Machine Learning AlgorithmsdarNo ratings yet
- 1 s2.0 S1110016822005191 MainDocument11 pages1 s2.0 S1110016822005191 MainWided HechkelNo ratings yet
- A Deep Learning Approach With Stack of Sub Classifiers For Multi Label Classification of Obstructive Disease From Myocardial Perfusion SpectDocument8 pagesA Deep Learning Approach With Stack of Sub Classifiers For Multi Label Classification of Obstructive Disease From Myocardial Perfusion Spectsafae afNo ratings yet
- Prediction of Heart Disease at Early Stage Using Data Mining and Big Data Analytics A SurveyDocument6 pagesPrediction of Heart Disease at Early Stage Using Data Mining and Big Data Analytics A SurveymanoNo ratings yet
- Locating Abnormal Heartbeats in ECG Segments Based On Deep Weakly Supervised LearningDocument10 pagesLocating Abnormal Heartbeats in ECG Segments Based On Deep Weakly Supervised Learning施展No ratings yet
- Journal of Electrocardiology: Raymond Bond Dewar Finlay, Salah Sha Fiq Al-Zaiti, Peter MacfarlaneDocument6 pagesJournal of Electrocardiology: Raymond Bond Dewar Finlay, Salah Sha Fiq Al-Zaiti, Peter Macfarlaneputri aprilianiNo ratings yet
- Ijigsp V10 N5 3Document10 pagesIjigsp V10 N5 3Arham SheikhNo ratings yet
- Portable Real Time ECG Monitor and Disease DiagnosDocument6 pagesPortable Real Time ECG Monitor and Disease DiagnosFahim87No ratings yet
- Carnevale, Innovative - MRI - Techniques - in - Neuroimaging - ApproachDocument15 pagesCarnevale, Innovative - MRI - Techniques - in - Neuroimaging - Approachlaila forestaNo ratings yet
- Brain Stroke Computed Tomography Images Analysis Using Image Processing: A ReviewDocument12 pagesBrain Stroke Computed Tomography Images Analysis Using Image Processing: A ReviewIAES IJAINo ratings yet
- BC 09Document6 pagesBC 09poorna1307No ratings yet
- Detection of Heart Attacks Using Machine LearningDocument9 pagesDetection of Heart Attacks Using Machine LearningIJRASETPublicationsNo ratings yet
- Heart Disease rp3Document20 pagesHeart Disease rp3EkanshNo ratings yet
- Three-Heartbeat Multilead ECG Recognition Method FDocument16 pagesThree-Heartbeat Multilead ECG Recognition Method Fbvkarthik2711No ratings yet
- Brain Hemorrhage Diagnosis by Using Deep Learning: Tong Duc Phong Hieu N. Duong Hien T. NguyenDocument6 pagesBrain Hemorrhage Diagnosis by Using Deep Learning: Tong Duc Phong Hieu N. Duong Hien T. NguyenManoj MaggotNo ratings yet
- Cvac 115Document21 pagesCvac 115Theofana MihailaNo ratings yet
- Micromachines 11 00629 v2Document27 pagesMicromachines 11 00629 v2Tanishka AggarwalNo ratings yet
- DDMHSA Dual Deterministic ModelBased Heart Sound Analysis For Daily Life MonitoringSensorsDocument17 pagesDDMHSA Dual Deterministic ModelBased Heart Sound Analysis For Daily Life MonitoringSensorsfrancogarciaramirez1No ratings yet
- Implementation of An Incremental Deep Learning Model For Survival Prediction of Cardiovascular PatientsDocument9 pagesImplementation of An Incremental Deep Learning Model For Survival Prediction of Cardiovascular PatientsIAES IJAINo ratings yet
- Diabetes Detection Using Deep Learning Algorithms: ICT Express November 2018Document5 pagesDiabetes Detection Using Deep Learning Algorithms: ICT Express November 2018Raza khanNo ratings yet
- Sensors 22 04670Document13 pagesSensors 22 04670hiimamanenuNo ratings yet
- Digital Design Lab ReportDocument9 pagesDigital Design Lab ReportSathvick BatchuNo ratings yet
- Vinay ResumeDocument1 pageVinay ResumeSathvick BatchuNo ratings yet
- Trips Hotel DownloadETicketDocument1 pageTrips Hotel DownloadETicketSathvick BatchuNo ratings yet
- Hindi Intent ClassificationDocument12 pagesHindi Intent ClassificationSathvick Batchu100% (1)
- Seminar ReportDocument2 pagesSeminar ReportSathvick BatchuNo ratings yet
- Hindi Intent ClassificationDocument13 pagesHindi Intent ClassificationSathvick BatchuNo ratings yet
- Deep Learning For Detecting and Locating Myocardial Infarction by Electrocardiogram - A Literature ReviewDocument28 pagesDeep Learning For Detecting and Locating Myocardial Infarction by Electrocardiogram - A Literature ReviewSathvick BatchuNo ratings yet
- Myocardial Risk As Preventive MedicineDocument18 pagesMyocardial Risk As Preventive MedicineSathvick BatchuNo ratings yet
- Assignment 2Document6 pagesAssignment 2Sathvick BatchuNo ratings yet
- Dr. Manjusha C B: Manjusha@iiitdwd - Ac.inDocument9 pagesDr. Manjusha C B: Manjusha@iiitdwd - Ac.inSathvick BatchuNo ratings yet
- Nataraj K S: DucationDocument3 pagesNataraj K S: DucationSathvick BatchuNo ratings yet
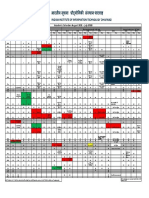
- Academic Calendar: August 2021 - July 2022Document1 pageAcademic Calendar: August 2021 - July 2022Sathvick BatchuNo ratings yet
- Happiness Frequency SurveyDocument6 pagesHappiness Frequency SurveySathvick BatchuNo ratings yet
- DSP Lab RecordDocument37 pagesDSP Lab RecordSathvick BatchuNo ratings yet
- Mini-Project-Report: Indian Institute of Information Technology DharwadDocument14 pagesMini-Project-Report: Indian Institute of Information Technology DharwadSathvick BatchuNo ratings yet
- Knots: India's Premier Crew MagazineDocument34 pagesKnots: India's Premier Crew MagazineSathvick BatchuNo ratings yet
- Linear Integrated Circuits - D. R. ChoudhuryDocument76 pagesLinear Integrated Circuits - D. R. ChoudhurySathvick BatchuNo ratings yet
- EACVI CCT Core SyllabusDocument13 pagesEACVI CCT Core SyllabushgadNo ratings yet
- Esc Cardiomed (3 Edn) : Epidemiology and Risk FactorsDocument12 pagesEsc Cardiomed (3 Edn) : Epidemiology and Risk FactorsNadhila IchwanNo ratings yet
- Good Thesis Statement For Heart DiseaseDocument5 pagesGood Thesis Statement For Heart Diseasemarilynmarieboston100% (2)
- The Past, Present and Future of PeriodontologyDocument182 pagesThe Past, Present and Future of PeriodontologyAlexandru EnacheNo ratings yet
- Abdominal Aortic Aneurysmn FINAL WORDDocument16 pagesAbdominal Aortic Aneurysmn FINAL WORDErica P. ManlunasNo ratings yet
- Revista Médica de ChileDocument8 pagesRevista Médica de ChileLudwigPlateBargielaNo ratings yet
- Coronary Artery AtherosclerosisDocument25 pagesCoronary Artery AtherosclerosisShahrizal Che JamelNo ratings yet
- Al., 2008. American Heart Association American Stroke AssociationDocument6 pagesAl., 2008. American Heart Association American Stroke AssociationPuput mopanggaNo ratings yet
- Human Biological Science 2 BIOL122: National Workshop Manual 2019Document78 pagesHuman Biological Science 2 BIOL122: National Workshop Manual 2019Huge Lovely SmileNo ratings yet
- Zuac 123Document11 pagesZuac 123Nelson Da VegaNo ratings yet
- Prevention of Heart DiseaseDocument43 pagesPrevention of Heart DiseaseamitmokalNo ratings yet
- Color Atlas of Forensic Pathology by Dinesh Fernando and Sulochana Wijetunge. Vol IDocument199 pagesColor Atlas of Forensic Pathology by Dinesh Fernando and Sulochana Wijetunge. Vol IGorka AguirreNo ratings yet
- HEARTDocument11 pagesHEART1NC21IS038 POLATHALA MOUNIKANo ratings yet
- Clubbing Amd Myo InfracDocument7 pagesClubbing Amd Myo InfracokaciaNo ratings yet
- Physical Fitness Short Note (SPSC 1011) Unit One 1. 1. Concepts of Physical Fitness1 1.1. 1. Meanings and Definitions of Physical FitnessDocument62 pagesPhysical Fitness Short Note (SPSC 1011) Unit One 1. 1. Concepts of Physical Fitness1 1.1. 1. Meanings and Definitions of Physical Fitnesseyob astatkeNo ratings yet
- Exercise For Cardiovascular Disease Prevention and Treatment From Molecular To Clinical Part 1Document320 pagesExercise For Cardiovascular Disease Prevention and Treatment From Molecular To Clinical Part 1Diego CardosoNo ratings yet
- Evidence Based Cardiology 4th EdDocument424 pagesEvidence Based Cardiology 4th EdROGER LUDEÑA SALAZARNo ratings yet
- Results: Dashboard Take Test My Progress Study Material My Video Buy Packages My QOD Notification ForumDocument165 pagesResults: Dashboard Take Test My Progress Study Material My Video Buy Packages My QOD Notification ForumMOHAMMED IQBALNo ratings yet
- Cardiovascular SyllabusDocument13 pagesCardiovascular SyllabusBrandonGilbertNo ratings yet
- Atherosclerosis and Its Complications-2Document59 pagesAtherosclerosis and Its Complications-2Kelly YeowNo ratings yet